
International Journal of
Reproductive Biomedicine
Fri, Apr 26, 2024
[Archive]
Volume 20, Issue 1 (January 2022)
IJRM 2022, 20(1): 37-46 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Borumandnia N, Alavi Majd H, Khadembashi N, Alaii H. Worldwide trend analysis of primary and secondary infertility rates over past decades: A cross-sectional study. IJRM 2022; 20 (1) :37-46
URL: http://ijrm.ir/article-1-2075-en.html
URL: http://ijrm.ir/article-1-2075-en.html



1- Urology and Nephrology Research Centre, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. , alavimajd@gmail.com
3- Department of Foreign Languages Education, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. , alavimajd@gmail.com
3- Department of Foreign Languages Education, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 3713 kb]
(2140 Downloads)
| Abstract (HTML) (1356 Views)
1. Introduction
Primary infertility is considered as occurring in a couple who have not had a live birth for more than five yr while they have been in a relationship without contraceptives. A couple with the desire to have a child who have been in a relationship for more than five years without using contraceptives, and without a live birth since a previous live birth are referred to as having secondary infertility (1).
Infertility is a global public health issue with a high impact on individuals of both sexes and society. Infertility is ranked as the 5th highest serious global disability with a negative impact on the self-esteem of those who are involved. These negative side effects remain a higher social burden for women than men (2).
More than half of infertility occurs in men (3). According to reports, some areas such as North Africa and the Middle East have witnessed a high rate of primary infertility prevalence, while secondary infertility has had a low prevalence. On the other hand, other regions such as Central and Western Europe have witnessed the opposite (4). The global prevalence of primary infertility and secondary infertility during 1990 to 2010 were reported in one study to be between 0.6-3.4% and 8.7-32.6%, respectively (5). Another study estimated the primary infertility prevalence to be within the range of 1.5-2.6%, which was lower than secondary infertility (7.2-18%) in 2009-2010 (6). According to another study, approximately 10.5% (with a range from less than 6% to greater than 16% by region and country) and 2% of women have experienced primary and secondary infertility, respectively, across the world during 1982-2010 (7). Infertility rates have been reported to be various in developed nations comparing with non-developed ones. Based on meta-analysis on population surveys published since 1990, the infertility prevalence is estimated to range from 3.5-16.7% in developed regions and from 6.9%-9.3% in developing nations (8). There are sparse data about the primary and secondary infertility prevalence in different regions of the world, and this statistic does not accurately represent infertility across regions in the world. In other words, there is no single outbreak, and great variations exist within and across different countries in each continent and region. Few comparative analyses have been conducted to explore the trends of primary and secondary infertility rates as regionally and globally in both sexes over multiple decades.
Therefore, this study was designed to investigate the trend of primary and secondary infertility prevalence rates over the past three decades, in the various epidemiological regions of the world. To achieve this goal, longitudinal data of primary and secondary infertility prevalence rates in previous years were compiled from the global burden of disease (GBD) database across the epidemiological sub-regions designated by the GBD.
2. Materials and Methods
2.1. Data source
This is a cross-sectional study, which longitudinal data from 1993-2017 for prevalence rates of primary and secondary infertility (per 100,000 peoples) for 195 countries and territories were extract from the GBD database, from the Institute for Health Metrics and Evaluation. The GBD is the most comprehensive observational epidemiological study, which report the prevalence, incidence, disability-adjusted life-years, death, etc. for diseases, and risk factors for all countries worldwide (9). The information used in this study includes the prevalence rates of both primary and secondary infertility for males and females, from 1993 to 2017. Seven regions were considered, including ‘High Income’, ‘Central Asia and Central and Eastern Europe’, ‘Latin America and Caribbean’, ‘North Africa and Middle East’, ‘South-East Asia, ‘South Asia’, East Asia and Oceania’ and ‘Sub-Saharan Africa’. The mentioned regions were designated by the GDB study. The trend of primary and secondary infertility prevalence rates was assessed in the regions, separately in males and females.
2.2. Ethical considerations
The approval ethics was done in Ethics Committee of Shahid Beheshti University of Medical Sciences (Code: IR.SBMU.RETECH.REC.1398.099).
2.3. Statistical analysis
The prevalence of primary and secondary infertility in regions and year (at six-year intervals which was considered due to statistical modelling and data structure considerations) were described together with the mean and standard deviation. The latent growth method (LGM) was used to estimate the change in prevalence rate of primary and secondary infertility in different regions, separately in males and females. The growth trajectory of prevalence rates over time was also estimated through LGM methods. The LGM regression coefficients showed the change rate of prevalence rate over time (10). The statistical analysis was performed using the M-plus version 6.12 (www.statmodel.com).
3. Results
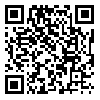
The mean and standard deviation of the primary and secondary infertility prevalence rates in seven regions are reported in tables I and II, respectively. The plots in figure 1 show the mean rates of infertility in various regions over this period. Also, the regression coefficients estimated from the LGM are presented in the last column of the tables. The intercepts coefficients in the table show the estimated mean of the initial infertility rate in 1993. The average change in the infertility rate over time in regions is reported as the slope. The sign of slope coefficients shows that the infertility rate had an increasing (positive sign) and decreasing (negative sign) trend over the period, respectively. For instance, the estimate of primary infertility of females in High-Income countries (intercept = 398.1, slope = -11.6) revealed that the initial prevalence rate of infertility was estimated to be 398.1 per 100,000 people in 1993 and it had a decreasing trend by -11.6 per six-year period until 2017. For another example, the LGM result for North Africa & Middle East females indicated that the initial prevalence rate of infertility was 630.3 per 100,000 and it had an increasing trend with a slope of about 38.5 until 2017.
The results of table I showed that in all areas, the primary infertility prevalence rate at the beginning of the study period was slightly lower among men than women. Also, the prevalence of primary infertility in men and women in High-Income countries has had a decreasing trend, with an average rate of change of -9.3 and -11.6 per 100,000 persons, respectively. Other regions have seen an increase in the prevalence of primary infertility. South Asian women had the highest average rate of change (40.9 per 100,000), followed by females in North Africa and Middle East (with an average rate of change of 38.5 per 100,000). Regarding primary infertility in men, North Africa and Middle East (with a rate of change of 19.0 per 100,000) and South Asia (with an average rate of change of 16.5 per 100,000) had the highest increasing rates.
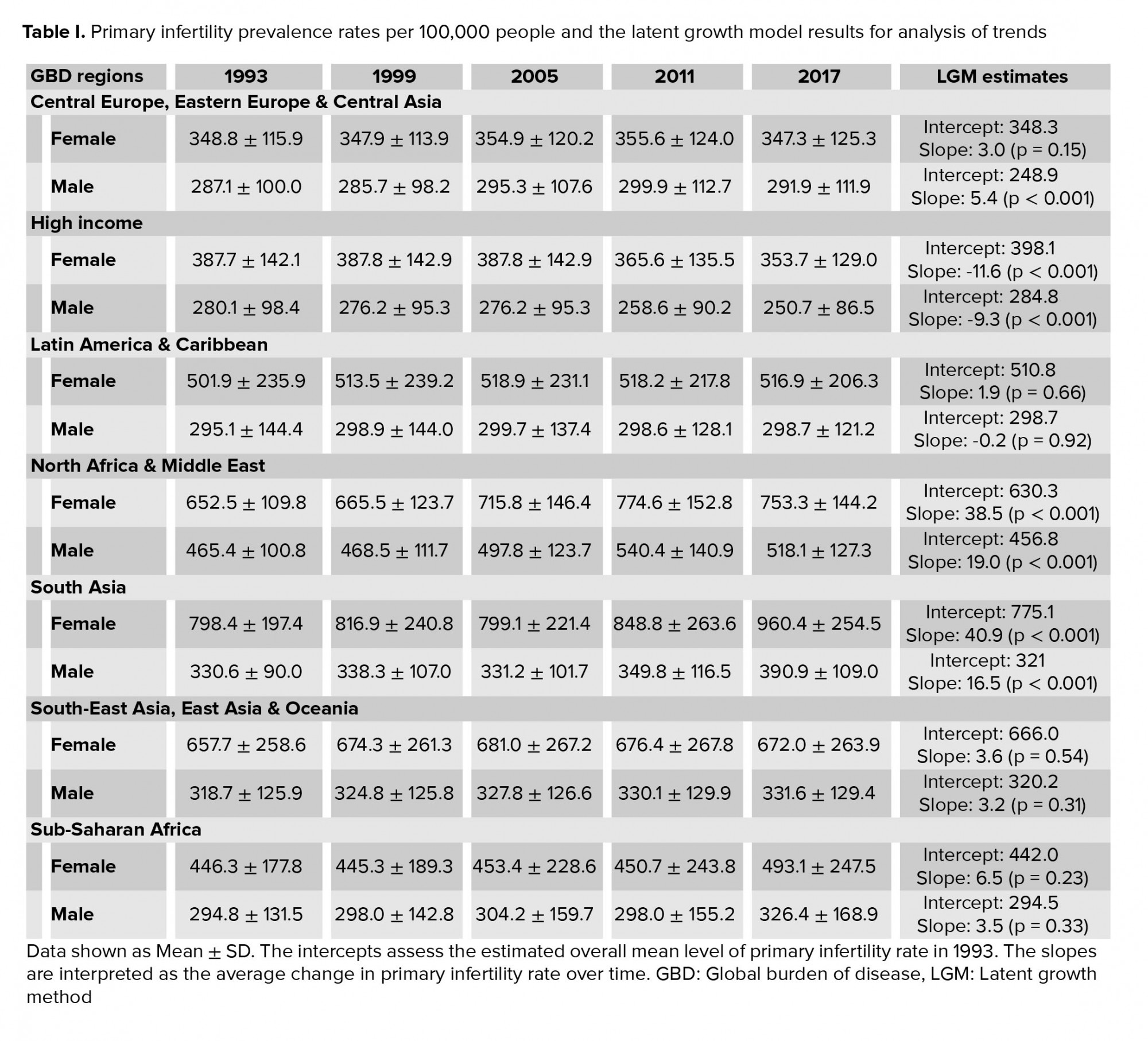
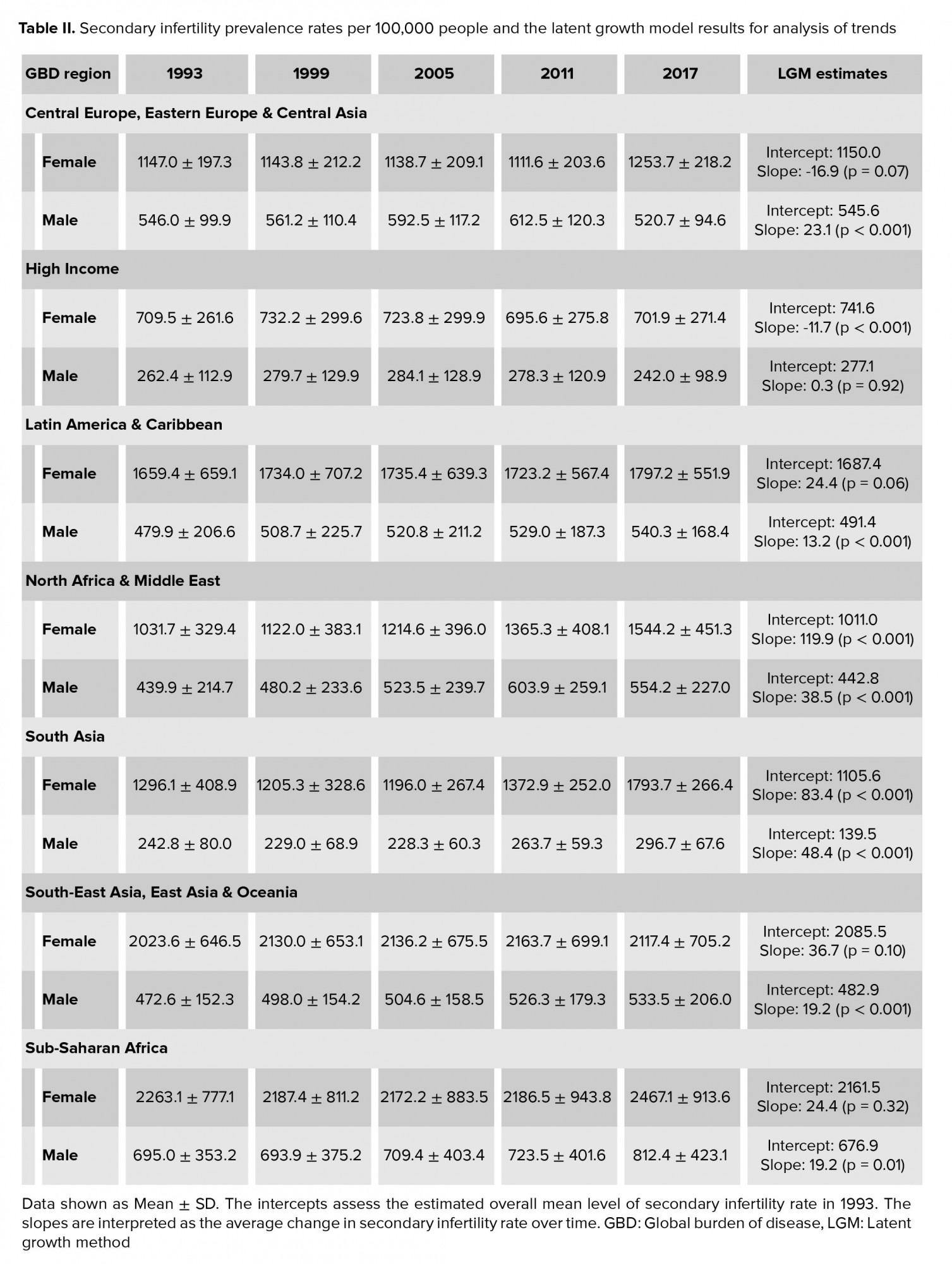
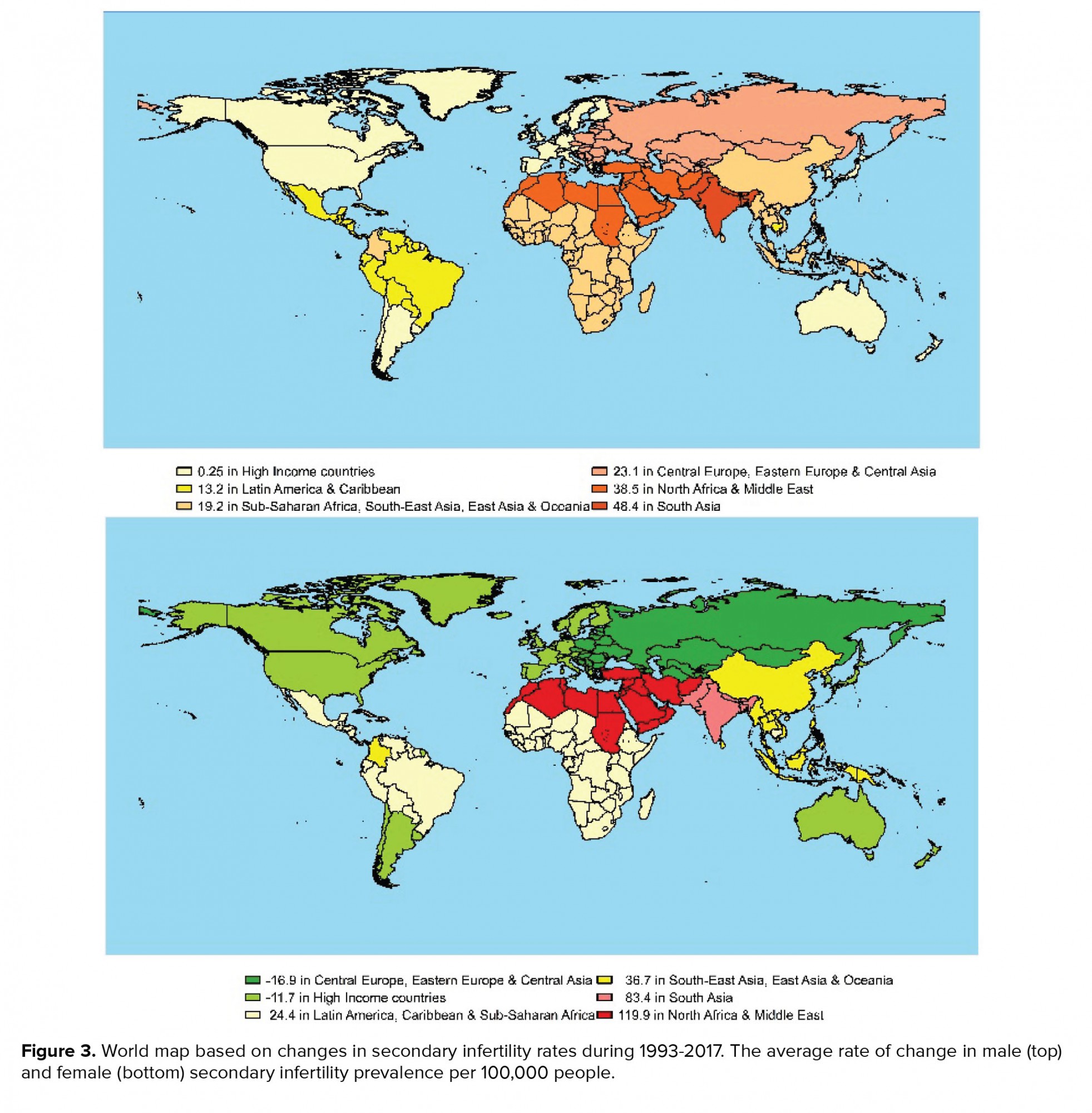
According to the results of secondary infertility shown in table II, once more, in all regions, the prevalence of secondary infertility at the beginning of the study period was higher among female compare with men. Over time, the rate of secondary infertility prevalence in women in Eastern and Central Europe, and Central Asia, as well as in High-Income countries have declinined with an average rate of change of -16.9 and -11.7 (per 100,000 persons), respectively. Other regions have been on the rise, with the highest increase in North Africa & Middle East among women (average rate of change: 119.9 per 100,000), followed by South Asian women (average rate of change: 83.4 per 100,000) and women in South-East Asia & Oceania (average rate of change: 36.7 per 100,000). Regarding secondary infertility in males, the prevalence rates have been increasing in all regions. The highest increase was found in South Asian men (with an average rate of change of 48.4 per 100,000) and the lowest increase was observed among men in High-Income regions (with an average rate of change of 0.25 per 100,000). The maps in figures 2 and 3 reveal the estimated trend of primary and secondary infertility rates from 1993 up to 2017 in the GBD regions.

4. Discussion
Infertility complications have been a concern across recent decades and are also a significant clinical problem today. In the present study, the infertility rate trend was explored in seven geographic regions designated by the GBD study.
The results demonstrated that during 1993-2017, the rate of primary infertility among men and women in High-Income countries declined. Although this trend also declined among Latin American & Caribbean men, this was not statistically significant. Other studies have claimed that male infertility has increased in developed countries and has become a problem worldwide during past decades (11). In the present study, it was observed that secondary male infertility increased over the time period, but primary male infertility decreased in the developed countries. In addition, the results showed that secondary infertility also decreased among women in Eastern and Central Europe and Central Asia, as well as High-Income regions.
However, some studies have claimed that Central and Eastern European and Central Asian countries, along with African countries, have high infertility rates, but this study suggested that infertility rates in these countries were lower than rates in African and Asian countries (12).
The reason for the decrease of infertility in these regions may be that Europe is the continent with the lowest total fertility rate (13). In other words, because the tendency for having children is low, infertility remains unrecognized. In fact, it seems that there is a straight relationship between infertility and the fertility rate. Although this seems to be a contradiction, it may be because by reducing fertility among communities, many cases of infertility remain unknown. Some factors lead to lower fertility, including the instability of modern partnerships and value changes in these countries. A notable point is that the United States offers significant services to people in the treatment of infertility (14, 15).
Among other regions, both men and women in Middle East and North Africa and also in South Asia have the highest trend in rates of primary and secondary infertility in recent years. These results are in line with the a systematic review related to increasing infertility in Africa (16). Various factors may be responsible for high infertility in the mentioned regions; in these regions, compared with the High-Income and other European countries, couples who already have a child go on to experience secondary infertility. Therefore, secondary infertility may be more commonly diagnosed in these countries, and the prevalence may be higher. Also, regions with a high prevalence of infectious diseases like HIV and also less industrialized nations have markedly higher infertility rates (17, 18).
The results indicated that the increase in infertility in developing countries was higher than in the developed ones. Various factors may cause a higher increase in infertility rates in these countries. Some of the factors that have been linked to an increase of infertility are dietary insufficiencies of iodine and selenium, and environmental and work-related toxicants including heavy metals, pesticides, arsenic, solvents, industrial chemicals and lead (19-22). Moreover, infertility treatment facilities in low- and middle-income countries are usually available only to wealthy people, so few have access to them (23, 24). Such populations tend to be conservative regarding things like sexuality, infertility and infectious diseases such as HIV. The silence around these issues contributes to accessibility disparities (25). This emphasizes the importance of infertility care availability and the socio-cultural value of childlessness and procreation in developing countries. Currently, there are differences between developed and developing populations in terms of these factors.
The other considerable finding in this research was that, not only was the growing trend of infertility in males estimated as lower than that of females, but also, women have had higher rates of infertility than men. In particular, in all regions, secondary infertility rates were several times higher in women than in men. In some studies, Sub-Saharan Africa has been named as the region with the highest prevalence of infertility (24). In this study, although the number of cases was high in women in Sub-Saharan Africa, the rate of growth was higher in the other regions, except for the High-Income and European and Central Asia regions. Obesity as an increasing problem in urban women which are poor, is a risk factor for infertility in these countries in developing countries (3). However, it is important to note that childbearing is considered a woman's duty in many countries, and men's information might not be collected. Infertility studies are generally performed on women (26). Also, the gold standard used for determining infertility in men makes it impossible to estimate the epidemiology of male infertility accurately (27).
One limitation in this study is about the not-existing accurate and reliable information about the infertility rate in some countries. In developing countries, the infertility rates may be more accurate comparing to developed ones. In some populations, infertility is a less-discussed topic where getting support seems difficult, and due to the lack of information, there is a sense of shame tied to fertility challenges; hence, this may be the reason that infertility has not been explored and recorded correctly in these communities.
5. Conclusion
Although the infertility rate is reported differently worldwide, the overall trend of infertility prevalence shows a downward fashion in high-income and developed countries and an upward trend in other regions. This may be because in these regions there may be unrecognized infertility due to a low tendency for reproduction and these regions have more infertility treatment facilities compared to the others. Clarification of the causes of these findings calls for more epidemiological studies.
Acknowledgements
We thank the Institute for Health Metrics and Evaluation for presenting the data. This study has not financial support.
Conflict of Interest
The authors declare that there is no conflict of interest.
Full-Text: (459 Views)
1. Introduction
Primary infertility is considered as occurring in a couple who have not had a live birth for more than five yr while they have been in a relationship without contraceptives. A couple with the desire to have a child who have been in a relationship for more than five years without using contraceptives, and without a live birth since a previous live birth are referred to as having secondary infertility (1).
Infertility is a global public health issue with a high impact on individuals of both sexes and society. Infertility is ranked as the 5th highest serious global disability with a negative impact on the self-esteem of those who are involved. These negative side effects remain a higher social burden for women than men (2).
More than half of infertility occurs in men (3). According to reports, some areas such as North Africa and the Middle East have witnessed a high rate of primary infertility prevalence, while secondary infertility has had a low prevalence. On the other hand, other regions such as Central and Western Europe have witnessed the opposite (4). The global prevalence of primary infertility and secondary infertility during 1990 to 2010 were reported in one study to be between 0.6-3.4% and 8.7-32.6%, respectively (5). Another study estimated the primary infertility prevalence to be within the range of 1.5-2.6%, which was lower than secondary infertility (7.2-18%) in 2009-2010 (6). According to another study, approximately 10.5% (with a range from less than 6% to greater than 16% by region and country) and 2% of women have experienced primary and secondary infertility, respectively, across the world during 1982-2010 (7). Infertility rates have been reported to be various in developed nations comparing with non-developed ones. Based on meta-analysis on population surveys published since 1990, the infertility prevalence is estimated to range from 3.5-16.7% in developed regions and from 6.9%-9.3% in developing nations (8). There are sparse data about the primary and secondary infertility prevalence in different regions of the world, and this statistic does not accurately represent infertility across regions in the world. In other words, there is no single outbreak, and great variations exist within and across different countries in each continent and region. Few comparative analyses have been conducted to explore the trends of primary and secondary infertility rates as regionally and globally in both sexes over multiple decades.
Therefore, this study was designed to investigate the trend of primary and secondary infertility prevalence rates over the past three decades, in the various epidemiological regions of the world. To achieve this goal, longitudinal data of primary and secondary infertility prevalence rates in previous years were compiled from the global burden of disease (GBD) database across the epidemiological sub-regions designated by the GBD.
2. Materials and Methods
2.1. Data source
This is a cross-sectional study, which longitudinal data from 1993-2017 for prevalence rates of primary and secondary infertility (per 100,000 peoples) for 195 countries and territories were extract from the GBD database, from the Institute for Health Metrics and Evaluation. The GBD is the most comprehensive observational epidemiological study, which report the prevalence, incidence, disability-adjusted life-years, death, etc. for diseases, and risk factors for all countries worldwide (9). The information used in this study includes the prevalence rates of both primary and secondary infertility for males and females, from 1993 to 2017. Seven regions were considered, including ‘High Income’, ‘Central Asia and Central and Eastern Europe’, ‘Latin America and Caribbean’, ‘North Africa and Middle East’, ‘South-East Asia, ‘South Asia’, East Asia and Oceania’ and ‘Sub-Saharan Africa’. The mentioned regions were designated by the GDB study. The trend of primary and secondary infertility prevalence rates was assessed in the regions, separately in males and females.
2.2. Ethical considerations
The approval ethics was done in Ethics Committee of Shahid Beheshti University of Medical Sciences (Code: IR.SBMU.RETECH.REC.1398.099).
2.3. Statistical analysis
The prevalence of primary and secondary infertility in regions and year (at six-year intervals which was considered due to statistical modelling and data structure considerations) were described together with the mean and standard deviation. The latent growth method (LGM) was used to estimate the change in prevalence rate of primary and secondary infertility in different regions, separately in males and females. The growth trajectory of prevalence rates over time was also estimated through LGM methods. The LGM regression coefficients showed the change rate of prevalence rate over time (10). The statistical analysis was performed using the M-plus version 6.12 (www.statmodel.com).
3. Results
The mean and standard deviation of the primary and secondary infertility prevalence rates in seven regions are reported in tables I and II, respectively. The plots in figure 1 show the mean rates of infertility in various regions over this period. Also, the regression coefficients estimated from the LGM are presented in the last column of the tables. The intercepts coefficients in the table show the estimated mean of the initial infertility rate in 1993. The average change in the infertility rate over time in regions is reported as the slope. The sign of slope coefficients shows that the infertility rate had an increasing (positive sign) and decreasing (negative sign) trend over the period, respectively. For instance, the estimate of primary infertility of females in High-Income countries (intercept = 398.1, slope = -11.6) revealed that the initial prevalence rate of infertility was estimated to be 398.1 per 100,000 people in 1993 and it had a decreasing trend by -11.6 per six-year period until 2017. For another example, the LGM result for North Africa & Middle East females indicated that the initial prevalence rate of infertility was 630.3 per 100,000 and it had an increasing trend with a slope of about 38.5 until 2017.
The results of table I showed that in all areas, the primary infertility prevalence rate at the beginning of the study period was slightly lower among men than women. Also, the prevalence of primary infertility in men and women in High-Income countries has had a decreasing trend, with an average rate of change of -9.3 and -11.6 per 100,000 persons, respectively. Other regions have seen an increase in the prevalence of primary infertility. South Asian women had the highest average rate of change (40.9 per 100,000), followed by females in North Africa and Middle East (with an average rate of change of 38.5 per 100,000). Regarding primary infertility in men, North Africa and Middle East (with a rate of change of 19.0 per 100,000) and South Asia (with an average rate of change of 16.5 per 100,000) had the highest increasing rates.
According to the results of secondary infertility shown in table II, once more, in all regions, the prevalence of secondary infertility at the beginning of the study period was higher among female compare with men. Over time, the rate of secondary infertility prevalence in women in Eastern and Central Europe, and Central Asia, as well as in High-Income countries have declinined with an average rate of change of -16.9 and -11.7 (per 100,000 persons), respectively. Other regions have been on the rise, with the highest increase in North Africa & Middle East among women (average rate of change: 119.9 per 100,000), followed by South Asian women (average rate of change: 83.4 per 100,000) and women in South-East Asia & Oceania (average rate of change: 36.7 per 100,000). Regarding secondary infertility in males, the prevalence rates have been increasing in all regions. The highest increase was found in South Asian men (with an average rate of change of 48.4 per 100,000) and the lowest increase was observed among men in High-Income regions (with an average rate of change of 0.25 per 100,000). The maps in figures 2 and 3 reveal the estimated trend of primary and secondary infertility rates from 1993 up to 2017 in the GBD regions.
4. Discussion
Infertility complications have been a concern across recent decades and are also a significant clinical problem today. In the present study, the infertility rate trend was explored in seven geographic regions designated by the GBD study.
The results demonstrated that during 1993-2017, the rate of primary infertility among men and women in High-Income countries declined. Although this trend also declined among Latin American & Caribbean men, this was not statistically significant. Other studies have claimed that male infertility has increased in developed countries and has become a problem worldwide during past decades (11). In the present study, it was observed that secondary male infertility increased over the time period, but primary male infertility decreased in the developed countries. In addition, the results showed that secondary infertility also decreased among women in Eastern and Central Europe and Central Asia, as well as High-Income regions.
However, some studies have claimed that Central and Eastern European and Central Asian countries, along with African countries, have high infertility rates, but this study suggested that infertility rates in these countries were lower than rates in African and Asian countries (12).
The reason for the decrease of infertility in these regions may be that Europe is the continent with the lowest total fertility rate (13). In other words, because the tendency for having children is low, infertility remains unrecognized. In fact, it seems that there is a straight relationship between infertility and the fertility rate. Although this seems to be a contradiction, it may be because by reducing fertility among communities, many cases of infertility remain unknown. Some factors lead to lower fertility, including the instability of modern partnerships and value changes in these countries. A notable point is that the United States offers significant services to people in the treatment of infertility (14, 15).
Among other regions, both men and women in Middle East and North Africa and also in South Asia have the highest trend in rates of primary and secondary infertility in recent years. These results are in line with the a systematic review related to increasing infertility in Africa (16). Various factors may be responsible for high infertility in the mentioned regions; in these regions, compared with the High-Income and other European countries, couples who already have a child go on to experience secondary infertility. Therefore, secondary infertility may be more commonly diagnosed in these countries, and the prevalence may be higher. Also, regions with a high prevalence of infectious diseases like HIV and also less industrialized nations have markedly higher infertility rates (17, 18).
The results indicated that the increase in infertility in developing countries was higher than in the developed ones. Various factors may cause a higher increase in infertility rates in these countries. Some of the factors that have been linked to an increase of infertility are dietary insufficiencies of iodine and selenium, and environmental and work-related toxicants including heavy metals, pesticides, arsenic, solvents, industrial chemicals and lead (19-22). Moreover, infertility treatment facilities in low- and middle-income countries are usually available only to wealthy people, so few have access to them (23, 24). Such populations tend to be conservative regarding things like sexuality, infertility and infectious diseases such as HIV. The silence around these issues contributes to accessibility disparities (25). This emphasizes the importance of infertility care availability and the socio-cultural value of childlessness and procreation in developing countries. Currently, there are differences between developed and developing populations in terms of these factors.
The other considerable finding in this research was that, not only was the growing trend of infertility in males estimated as lower than that of females, but also, women have had higher rates of infertility than men. In particular, in all regions, secondary infertility rates were several times higher in women than in men. In some studies, Sub-Saharan Africa has been named as the region with the highest prevalence of infertility (24). In this study, although the number of cases was high in women in Sub-Saharan Africa, the rate of growth was higher in the other regions, except for the High-Income and European and Central Asia regions. Obesity as an increasing problem in urban women which are poor, is a risk factor for infertility in these countries in developing countries (3). However, it is important to note that childbearing is considered a woman's duty in many countries, and men's information might not be collected. Infertility studies are generally performed on women (26). Also, the gold standard used for determining infertility in men makes it impossible to estimate the epidemiology of male infertility accurately (27).
One limitation in this study is about the not-existing accurate and reliable information about the infertility rate in some countries. In developing countries, the infertility rates may be more accurate comparing to developed ones. In some populations, infertility is a less-discussed topic where getting support seems difficult, and due to the lack of information, there is a sense of shame tied to fertility challenges; hence, this may be the reason that infertility has not been explored and recorded correctly in these communities.
5. Conclusion
Although the infertility rate is reported differently worldwide, the overall trend of infertility prevalence shows a downward fashion in high-income and developed countries and an upward trend in other regions. This may be because in these regions there may be unrecognized infertility due to a low tendency for reproduction and these regions have more infertility treatment facilities compared to the others. Clarification of the causes of these findings calls for more epidemiological studies.
Acknowledgements
We thank the Institute for Health Metrics and Evaluation for presenting the data. This study has not financial support.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Epidemiology
References
1. GBD 2017 disease and injury incidence and prevalence collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018; 392: 1789-1858. [DOI:10.1016/S0140-6736(18)32279-7]
2. Zayed AA, El-Hadidy MA. Sexual satisfaction and self-esteem in women with primary infertility. Middle East Fertil Soc J 2020; 25: 13. [DOI:10.1186/s43043-020-00024-5]
3. Inhorn MC. Local babies, global science: Gender, religion, and in vitro fertilization in Egypt. New York: Routledge; 2003.
4. Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel Sh, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med 2012; 9: e1001356. [DOI:10.1371/journal.pmed.1001356] [PMID] [PMCID]
5. Dhandapani K, Kodavanji B, Vinodini NA. Association of body mass index with primary and secondary infertility among infertile women in Mangalore: A cross-sectional study. Natl J Physiol Pharm Pharmacol 2016; 6: 81-84. [DOI:10.5455/njppp.2015.5.2108201585]
6. Martins AD, Selvam MKP, Agarwal A, Alves MG, Baskaran S. Alterations in seminal plasma proteomic profile in men with primary and secondary infertility. Sci Rep 2020; 10: 7539.
https://doi.org/10.1038/s41598-020-64434-1 [DOI:10.1038/s41598-020-69838-7] [PMID] [PMCID]
7. Chaubey L, Singh TB, Kaithwas K, Doharey N, Peddappolla ShCh. Risk factors associated with primary and secondary infertility in eastern part of north India: A pilot study. J Commun Health Manage 2018; 5: 188-191. [DOI:10.18231/2394-2738.2018.0038]
8. Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: Potential need and demand for infertility medical care. Hum Reprod 2007; 22: 1506-1512.
https://doi.org/10.1093/humrep/dem299 [DOI:10.1093/humrep/dem046] [PMID]
9. Global Burden of Disease Collaborative Network. Global burden of disease study 2016 (GBD 2016) results. Seattle, Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2017. Available at: http://ghdx.healthdata.org/gbd-results-tool.
10. Wang J, Wang X. Structural equation modeling: Applications using Mplus. New York: John Wiley & Sons; 2012. [DOI:10.1002/9781118356258]
11. Janiszewska E, Kratz EM. Could the glycosylation analysis of seminal plasma clusterin become a novel male infertility biomarker? Mol Reprod Dev 2020; 87: 515-524. [DOI:10.1002/mrd.23340] [PMID]
12. Vander Borght M, Wyns Ch. Fertility and infertility: Definition and epidemiology. Clin Biochem 2018; 62: 2-10. [DOI:10.1016/j.clinbiochem.2018.03.012] [PMID]
13. ESHRE capri workshop group. Europe the continent with the lowest fertility. Hum Reprod Update 2010; 16: 590-602. [DOI:10.1093/humupd/dmq023] [PMID]
14. Brezina PR. Fertility treatment in the United States: The case for increased access to care. JFIV Reprod Med Genet 2015; 3: e112.
15. Kissin DM, Boulet ShL, Jamieson DJ, Assisted Reproductive Technology Surveillance and Research Team. Fertility treatments in the United States: Improving access and outcomes. Obstet Gynecol 2016; 128: 387-390. [DOI:10.1097/AOG.0000000000001419] [PMID] [PMCID]
16. Abebe MSh, Afework M, Abaynew Y. Primary and secondary infertility in Africa: Systematic review with meta-analysis. Fertil Res Pract 2020; 6: 20. [DOI:10.1186/s40738-020-00090-3] [PMID] [PMCID]
17. Kumar N, Singh AK. Trends of male factor infertility, an important cause of infertility: A review of literature. J Hum Reprod Sci 2015; 8: 191-196. [DOI:10.4103/0974-1208.170370] [PMID] [PMCID]
18. Zayeri F, Talebi Ghane E, Borumandnia N. Assessing the trend of HIV/AIDS mortality rate in Asia and North Africa: An application of latent growth models. Epidemiol Infect 2016; 144: 548-555. [DOI:10.1017/S0950268815001351] [PMID]
19. Ibeh IN, Uraih N, Ogonar JI. Dietary exposure to aflatoxin in human male infertility in Benin City, Nigeria. Int J Fertil Menopausal Stud 1994; 39: 208-214.
20. Longombe AO, Geelhoed GW. Iodine deficiency disorders and infertility in northeast Zaire. Nutrition 1997; 13: 342-343. [DOI:10.1016/S0899-9007(97)00076-2]
21. Mattison DR, Plowchalk DR, Meadows MJ, Al-Juburi AZ, Gandy J, Malek A. Reproductive toxicity: Male and female reproductive systems as targets for chemical injury. Med Clin North Am 1990; 74: 391-411. [DOI:10.1016/S0025-7125(16)30569-7]
22. Sharara FI, Seifer DB, Flaws JA. Environmental toxicants and female reproduction. Fertil Steril 1998; 70: 613-622. [DOI:10.1016/S0015-0282(98)00253-2]
23. Hall DR, Hanekom G. Assisted reproduction and justice: Threats to a new model in a low‐and middle‐income country. Dev World Bioeth 2020; 20: 167-171. [DOI:10.1111/dewb.12252] [PMID]
24. Chiware TM, Vermeulen N, Blondeel K, Farquharson R, Kiarie J, Lundin K, et al. IVF and other ART in low- and middle-income countries: A systematic landscape analysis. Hum Reprod Update 2021; 27: 213-228. [DOI:10.1093/humupd/dmaa047] [PMID] [PMCID]
25. Walks M. Breaking the silence: Infertility, motherhood, and queer culture. J Motherhood Initiative Res Commun Involvement 2007; 9: 130-143.
26. Fledderjohann J, Roberts CM. Missing men, missing infertility: The enactment of sex/gender in surveys in low-and middle-income countries. Population Horizons 2019; 15: 66-87. [DOI:10.1515/pophzn-2018-0003]
27. Faassse MA, Niederberger CS. Epidemiologic considerations in male infertility. Parekattil SJ, Agarwal A. Male infertility. Germany: Springer; 2020.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
