
International Journal of
Reproductive Biomedicine
Tue, May 7, 2024
[Archive]
Volume 19, Issue 9 (September 2021)
IJRM 2021, 19(9): 837-844 |
Back to browse issues page




![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Vahidi S, Narimani N, Abouei S, Sadeghi A, Lorian K, Rahavian A. Comparison of intracytoplasmic sperm injection outcomes in azoospermic men who underwent testicular sperm extraction vs. microdissection testicular sperm extraction: A cross-sectional study. IJRM 2021; 19 (9) :837-844
URL: http://ijrm.ir/article-1-2315-en.html
URL: http://ijrm.ir/article-1-2315-en.html
Serajoddin Vahidi1 

 , Nima Narimani2 , Saeid Abouei3 , Ali Sadeghi4 , Keivan Lorian5 , Amirhossein Rahavian * 6
, Nima Narimani2 , Saeid Abouei3 , Ali Sadeghi4 , Keivan Lorian5 , Amirhossein Rahavian * 6
, Nima Narimani2 , Saeid Abouei3 , Ali Sadeghi4 , Keivan Lorian5 , Amirhossein Rahavian * 6
1- Andrology Research Center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2- Hasheminejad Kidney Center, Iran University of Medical Sciences, Tehran, Iran.
3- Student Research Committee, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Department of Surgical Technology, Faculty of Paramedical, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
6- Andrology Research Center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. , amirrahavian@yahoo.com
2- Hasheminejad Kidney Center, Iran University of Medical Sciences, Tehran, Iran.
3- Student Research Committee, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Department of Surgical Technology, Faculty of Paramedical, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
6- Andrology Research Center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. , amirrahavian@yahoo.com
Keywords: Intracytoplasmic sperm injection, Azoospermia, Testicular sperm extraction, Microdissection testicular sperm extraction, Pregnancy outcome.
Full-Text [PDF 269 kb]
(637 Downloads)
| Abstract (HTML) (1399 Views)
1. Introduction
The worldwide estimated prevalence of infertility is about 10-15% (1); however, primary infertility in Iran is about 25% (2). About 10-15% of infertile men are azoospermic (3). Azoospermia is defined as the complete absence of sperm in the semen sample and is categorized into two groups: obstructive (OA) and nonobstructive (NOA) (4, 5). With the advent of intracytoplasmic sperm injection (ICSI) in 1992, the azoospermic men who once were considered sterile, regained the chance to have their own biological children (6). OA is further categorized as primary (congenital) or secondary (acquired). Assisted reproductive techniques are commonly advised in cases of the primary form and when the reconstruction of the complex secondary structure is impossible. Given that there is normal spermatogenesis in the testes in OA, sperms can be retrieved through different methods (5).
Conversely, azoospermia in NOA may be due to disrupted spermatogenesis. Given the aggressiveness and low success rate of sperm retrieval by testicular sperm extraction (TESE) in NOA, Schlegel introduced microdissection sperm retrieval (micro-TESE) to improve the sperm recovery rate and testis viability preservation. The sperm retrieval rate of micro-TESE is about 16%–63% (7, 8).
Different studies have reported different fertilization, pregnancy, miscarriage and live birth rates between these two groups. For instance, one study found lower fertilization rates in men with NOA but similar clinical pregnancy rates between OA and NOA groups (5). Some studies have reported similar ICSI outcomes in men with OA vs. NOA, including a retrospective study in 2008 which found that the miscarriage rate did not significantly differ between the NOA and OA groups (9). Other studies have shown higher pregnancy rates in OA cases (10-12). Furthermore, some studies have revealed that factors like maternal age can influence the success rate of ICSI (13).
For successful in vitro fertilization, it is necessary for both the sperm and oocyte to be high quality (14, 15). Some oocyte quality criteria that can be assessed non-invasively are the dispersion cumulus cell, and the existence of a first polar body which shows nuclear maturity and no sign of atresia. Other abnormalities which can affect oocyte quality and total fertilization failure (TFF) are the accumulation of smooth endoplasmic reticulum discs and asynchronous nuclear and cytoplasmic maturation (16).
Two important parameters for the oocyte’s developmental potential are mitochondrial function and intracellular Ca2+. The activity of the mitochondria and mitochondrial metabolism are regulated by mitochondrial Ca2+. Sperm-oocyte fusion activates Ca2+ oscillation, which plays a critical role in changing the state of the fertilized oocyte’s mitochondria from its resting state to the active state. Then the mitochondrial activity maintains the Ca2+ oscillations (17).
So, we conducted this study to evaluate differences in the results of ICSI between OA cases who underwent TESE vs. NOA cases who underwent micro-TESE for sperm extraction.
2. Materials and Methods
A total of 310 azoospermic men who underwent ICSI for the first time from September 2016 to September 2020 in the Yazd Reproductive Sciences Institute, a tertiary referral center for infertility in Iran, were enrolled in this retrospective cross-sectional study. Cases were divided into two groups: one group underwent TESE for sperm extraction (n = 172) and the other group underwent micro-TESE (n = 138). The inclusion criteria for the TESE group were normal testes volume and acceptable hormonal assay (which was defined as blood luteinizing hormone (LH) and follicle stimulating hormone (FSH) levels < two times higher than the normal range). The inclusion criteria for the micro-TESE group were low testicular volume and high hormonal assay (blood LH and FSH levels ≥ two times higher than the normal range). The inclusion criterion of the female partner was the best quality of oocyte (spherical, no cytoplasmic granules, no aggregation of the smooth endoplasmic reticulum discs, no vacuoles). The included women were aged < 40 yr and the men were < 50 yr. Men with a history of bilateral vasectomy, varicocelectomy, a testicular tumor, chemo-radiation, hypogonadotropic hypogonadism, epididymo-orchitis, or genetic abnormality were excluded from the study.
Medical records of these individuals were reviewed, and the maternal and paternal age, and the fertilization, biochemical pregnancy, abortion and live birth rates were extracted from the files and compared between the groups. The effect of maternal and paternal age on ICSI outcomes was analyzed.
Biochemical pregnancy and abortion were defined as a positive human chorionic gonadotropin (hCG) test three weeks after implantation and a miscarriage at least three months after implantation, respectively. Semen analysis was performed and only azoospermia cases were selected. TFF occurred in 41% of TESE cases and 55% of micro-TESE cases.
2.1. Ethical considerations
This study was approved by the ethics committee of Research and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.RSI.REC.1400.006). Consent was obtained from all participants orally.
2.2. Statistical analysis
The Statistical Package for the Social Sciences (SPSS) version 20 (IBM, California, United States) was used to perform Chi-square tests for the qualitative data, and the quantitative outcomes were analyzed through descriptive statistics (mean ± standard deviation) and independent t tests. Regression analysis was performed to determine the association of maternal and paternal age with ICSI outcomes. P < 0.05 was considered the statistical significance level.
3. Results
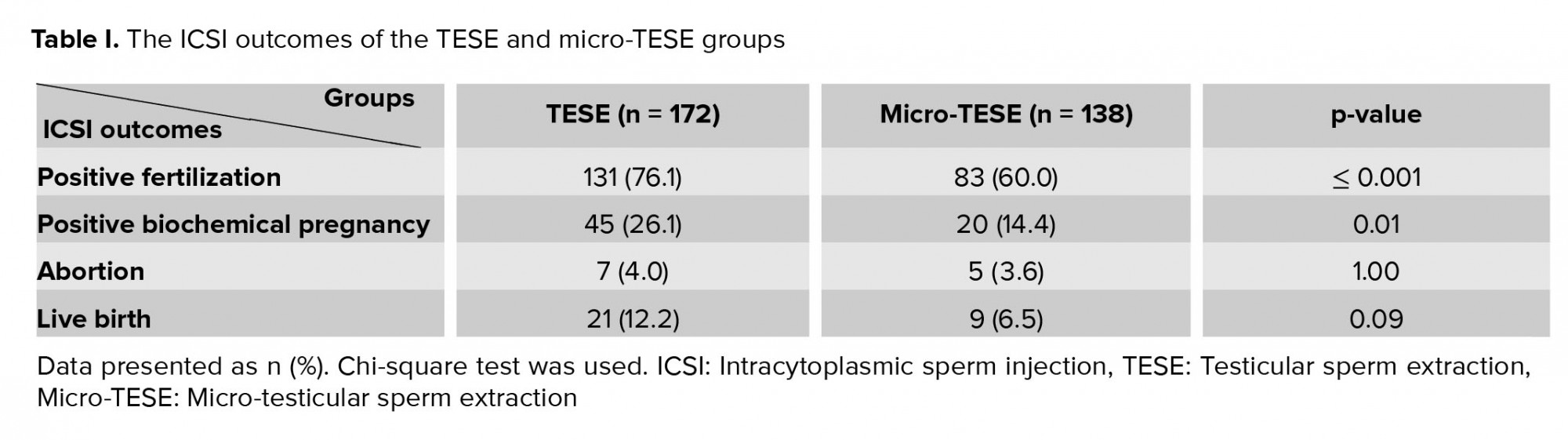
Over four years, a total of 555 ICSI procedures were performed in our Center. 254 (46%) cases underwent micro-TESE for sperm extraction, and the others underwent TESE and percutaneous epididymal sperm aspiration. 245 (44.1%) cases were excluded from the study based on the inclusion and exclusion criteria, and the remaining cases were categorized into two groups (TESE and micro-TESE). The mean paternal age was significantly different between the two groups (40.65 ± 9.22 yr vs. 36.70 ± 5.86 yr for the TESE and micro-TESE groups, respectively, with a range of 24-50 yr; p ≤ 0.001). Also, the mean age of women was significantly higher in the TESE group (34.97 ± 4.22 yr vs. 32.35 ± 5.77 yr, with a range of 18-40 yr; p ≤ 0.001). The ICSI outcomes of the two groups are shown in Table I.
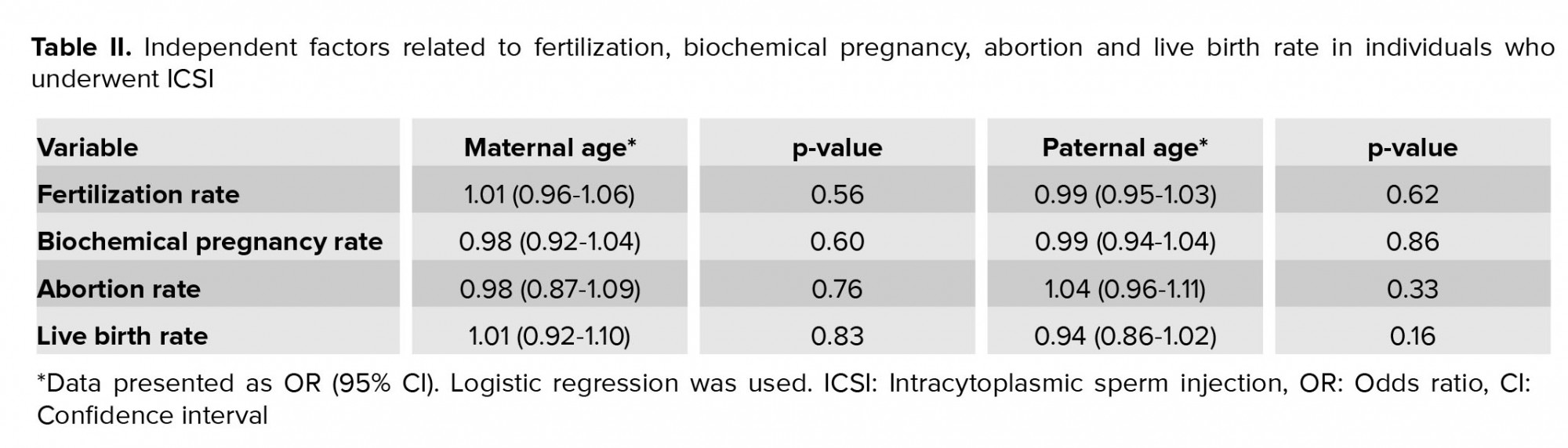
Logistic regression analysis was done to evaluate the impact of maternal and paternal age on ICSI outcomes, and it revealed that there was no relationship between these variables (Table II).
4. Discussion
In the present study, the outcomes of ICSI in OA cases who underwent TESE and NOA cases who underwent micro-TESE for sperm extraction were investigated. In total, 555 men with OA and NOA were involved in the ICSI technique and 310 of these were included in this study. The data analysis demonstrated that the individuals with OA had a 76.1% positive fertilization rate and individuals with NOA had a 60.0% fertilization rate. Moreover, the positive biochemical pregnancy rate was significantly higher in OA individuals. The live birth rate was also higher in OA individuals compared to the individuals with NOA, but the abortion rate was similar. In addition, the mean paternal age was significantly different between the two groups. Also, the mean age of the women was significantly higher in the TESE group.
NOA individuals are classified into two groups: hypogonadotropic hypogonadism and hypergonadotropic hypogonadism or eugonadism. Individuals with hypogonadotropic hypogonadism are characterized by low FSH, low LH and low testosterone levels. The congenital cause for this group is Kallmann syndrome (hypothalamic GnRH deficiency) and the acquired cause is pituitary tumors. In hypogonadotropic hypogonadism cases, gonadotropin therapy is started for three to six months to induce spermatogenesis. hCG and FSH are used. hCG is sufficient to induce spermatogenesis but FSH optimizes this process, especially in individuals with congenital abnormalities. Pulsatile GnRH injection is another therapy for this group. The hypergonadotropic hypogonadism or eugonadism group can be diagnosed by normal/high FSH, normal/high LH and normal/low testosterone levels. Genetic abnormalities (chromosomal) are the congenital cause of this group, and varicocele, orchitis, gonadotoxins (chemotherapy/radiation), trauma/torsion and idiopathic reasons are the acquired causes of these cases.
The spermatogenesis process requires high levels of intra-testicular testosterone. The aromatase enzyme converts androgens to estrogens in men. Aromatase inhibitors block this conversion and have a potential role in NOA individuals (18). Antiestrogens and gonadotropins are also used in the treatment of this group. Microsurgical reconstruction or sperm retrieval processes that are used in assisted reproductive techniques are the main treatments for men with OA (19).
Para-clinical tests such as hormone and genetic assessments help to understand the causes of azoospermia, especially NOA. Through hormone assessment, the condition can be properly diagnosed and the physician can better initiate hormone therapy. Moreover, these tests can help to predict the success of medical therapy and surgical sperm retrieval (18).
In this study, it was proposed that men with NOA who underwent ICSI would have poorer outcomes in all parameters than men with OA. According to the results, the men with NOA had a significantly lower fertilization and clinical pregnancy rate than the men with OA. The reason for the lower fertilization rate in NOA cases is the early paternal effect, which can be caused by dysregulation and dysfunction of oocyte-activating factors, centrosomes, and cytoskeletal components (20, 21).
It has been shown that miscarriage rates may be higher in men with NOA due to aneuploidy and DNA damage in NOA spermatozoa that may contribute to a late paternal effect, leading to pregnancy loss (20, 22, 23). The results of the present study are similar to those of several other studies that revealed significant higher fertilization rates in the men with OA compared with in those with NOA (11, 24, 25). These results can be explained by the sperm functional impairment in men with NOA, which increases genetic abnormalities in these men (26). However, in research conducted in 2015, no differences were observed in the fertility rate or clinical pregnancy rate between the OA and NOA groups (27). In 2005 a metaanalysis revealed that fertilization rate is lower in NOA cases (5). A retrospective study showed lower pregnancy rates in men with NOA than in men with OA (9). In another study, it was indicated that the clinical pregnancy rate in men with NOA was lower than in men with OA (28). In another comparison of NOA and OA outcomes, the implantation rate was found to be lower in the NOA group (29).
Factors that can affect the outcome of ICSI when using non-ejaculated sperm include the azoospermia etiology, the age of the female partner, and the sperm status (fresh or thawed) (30). A younger maternal age has been found to have a positive effect on the fertilization and clinical pregnancy rates of OA men (30). However, some studies have suggested that maternal age does not impact fertilization rates but only affects pregnancy rates (13, 31). Overall, both men with OA and NOA can have successful pregnancies. More research is required to understand the impact of variables such as maternal age and paternal effect on the fertilization rate and miscarriage in men with OA and NOA. Finding and understanding more about factors that affect ICSI outcomes can help us to predict the outcome of fertility procedures and advise our cases better.
5. Conclusion
This study confirmed previous findings that men with OA had significantly higher fertilization and biochemical pregnancy rates than men with NOA. The live birth rate was higher in men with OA, but this difference was not significant.
Acknowledgements
We thank all our patients and their relatives. This research was financially supported by the Research and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Conflict of Interest
There is no conflict of interest.
Full-Text: (249 Views)
1. Introduction
The worldwide estimated prevalence of infertility is about 10-15% (1); however, primary infertility in Iran is about 25% (2). About 10-15% of infertile men are azoospermic (3). Azoospermia is defined as the complete absence of sperm in the semen sample and is categorized into two groups: obstructive (OA) and nonobstructive (NOA) (4, 5). With the advent of intracytoplasmic sperm injection (ICSI) in 1992, the azoospermic men who once were considered sterile, regained the chance to have their own biological children (6). OA is further categorized as primary (congenital) or secondary (acquired). Assisted reproductive techniques are commonly advised in cases of the primary form and when the reconstruction of the complex secondary structure is impossible. Given that there is normal spermatogenesis in the testes in OA, sperms can be retrieved through different methods (5).
Conversely, azoospermia in NOA may be due to disrupted spermatogenesis. Given the aggressiveness and low success rate of sperm retrieval by testicular sperm extraction (TESE) in NOA, Schlegel introduced microdissection sperm retrieval (micro-TESE) to improve the sperm recovery rate and testis viability preservation. The sperm retrieval rate of micro-TESE is about 16%–63% (7, 8).
Different studies have reported different fertilization, pregnancy, miscarriage and live birth rates between these two groups. For instance, one study found lower fertilization rates in men with NOA but similar clinical pregnancy rates between OA and NOA groups (5). Some studies have reported similar ICSI outcomes in men with OA vs. NOA, including a retrospective study in 2008 which found that the miscarriage rate did not significantly differ between the NOA and OA groups (9). Other studies have shown higher pregnancy rates in OA cases (10-12). Furthermore, some studies have revealed that factors like maternal age can influence the success rate of ICSI (13).
For successful in vitro fertilization, it is necessary for both the sperm and oocyte to be high quality (14, 15). Some oocyte quality criteria that can be assessed non-invasively are the dispersion cumulus cell, and the existence of a first polar body which shows nuclear maturity and no sign of atresia. Other abnormalities which can affect oocyte quality and total fertilization failure (TFF) are the accumulation of smooth endoplasmic reticulum discs and asynchronous nuclear and cytoplasmic maturation (16).
Two important parameters for the oocyte’s developmental potential are mitochondrial function and intracellular Ca2+. The activity of the mitochondria and mitochondrial metabolism are regulated by mitochondrial Ca2+. Sperm-oocyte fusion activates Ca2+ oscillation, which plays a critical role in changing the state of the fertilized oocyte’s mitochondria from its resting state to the active state. Then the mitochondrial activity maintains the Ca2+ oscillations (17).
So, we conducted this study to evaluate differences in the results of ICSI between OA cases who underwent TESE vs. NOA cases who underwent micro-TESE for sperm extraction.
2. Materials and Methods
A total of 310 azoospermic men who underwent ICSI for the first time from September 2016 to September 2020 in the Yazd Reproductive Sciences Institute, a tertiary referral center for infertility in Iran, were enrolled in this retrospective cross-sectional study. Cases were divided into two groups: one group underwent TESE for sperm extraction (n = 172) and the other group underwent micro-TESE (n = 138). The inclusion criteria for the TESE group were normal testes volume and acceptable hormonal assay (which was defined as blood luteinizing hormone (LH) and follicle stimulating hormone (FSH) levels < two times higher than the normal range). The inclusion criteria for the micro-TESE group were low testicular volume and high hormonal assay (blood LH and FSH levels ≥ two times higher than the normal range). The inclusion criterion of the female partner was the best quality of oocyte (spherical, no cytoplasmic granules, no aggregation of the smooth endoplasmic reticulum discs, no vacuoles). The included women were aged < 40 yr and the men were < 50 yr. Men with a history of bilateral vasectomy, varicocelectomy, a testicular tumor, chemo-radiation, hypogonadotropic hypogonadism, epididymo-orchitis, or genetic abnormality were excluded from the study.
Medical records of these individuals were reviewed, and the maternal and paternal age, and the fertilization, biochemical pregnancy, abortion and live birth rates were extracted from the files and compared between the groups. The effect of maternal and paternal age on ICSI outcomes was analyzed.
Biochemical pregnancy and abortion were defined as a positive human chorionic gonadotropin (hCG) test three weeks after implantation and a miscarriage at least three months after implantation, respectively. Semen analysis was performed and only azoospermia cases were selected. TFF occurred in 41% of TESE cases and 55% of micro-TESE cases.
2.1. Ethical considerations
This study was approved by the ethics committee of Research and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.RSI.REC.1400.006). Consent was obtained from all participants orally.
2.2. Statistical analysis
The Statistical Package for the Social Sciences (SPSS) version 20 (IBM, California, United States) was used to perform Chi-square tests for the qualitative data, and the quantitative outcomes were analyzed through descriptive statistics (mean ± standard deviation) and independent t tests. Regression analysis was performed to determine the association of maternal and paternal age with ICSI outcomes. P < 0.05 was considered the statistical significance level.
3. Results
Over four years, a total of 555 ICSI procedures were performed in our Center. 254 (46%) cases underwent micro-TESE for sperm extraction, and the others underwent TESE and percutaneous epididymal sperm aspiration. 245 (44.1%) cases were excluded from the study based on the inclusion and exclusion criteria, and the remaining cases were categorized into two groups (TESE and micro-TESE). The mean paternal age was significantly different between the two groups (40.65 ± 9.22 yr vs. 36.70 ± 5.86 yr for the TESE and micro-TESE groups, respectively, with a range of 24-50 yr; p ≤ 0.001). Also, the mean age of women was significantly higher in the TESE group (34.97 ± 4.22 yr vs. 32.35 ± 5.77 yr, with a range of 18-40 yr; p ≤ 0.001). The ICSI outcomes of the two groups are shown in Table I.
Logistic regression analysis was done to evaluate the impact of maternal and paternal age on ICSI outcomes, and it revealed that there was no relationship between these variables (Table II).
4. Discussion
In the present study, the outcomes of ICSI in OA cases who underwent TESE and NOA cases who underwent micro-TESE for sperm extraction were investigated. In total, 555 men with OA and NOA were involved in the ICSI technique and 310 of these were included in this study. The data analysis demonstrated that the individuals with OA had a 76.1% positive fertilization rate and individuals with NOA had a 60.0% fertilization rate. Moreover, the positive biochemical pregnancy rate was significantly higher in OA individuals. The live birth rate was also higher in OA individuals compared to the individuals with NOA, but the abortion rate was similar. In addition, the mean paternal age was significantly different between the two groups. Also, the mean age of the women was significantly higher in the TESE group.
NOA individuals are classified into two groups: hypogonadotropic hypogonadism and hypergonadotropic hypogonadism or eugonadism. Individuals with hypogonadotropic hypogonadism are characterized by low FSH, low LH and low testosterone levels. The congenital cause for this group is Kallmann syndrome (hypothalamic GnRH deficiency) and the acquired cause is pituitary tumors. In hypogonadotropic hypogonadism cases, gonadotropin therapy is started for three to six months to induce spermatogenesis. hCG and FSH are used. hCG is sufficient to induce spermatogenesis but FSH optimizes this process, especially in individuals with congenital abnormalities. Pulsatile GnRH injection is another therapy for this group. The hypergonadotropic hypogonadism or eugonadism group can be diagnosed by normal/high FSH, normal/high LH and normal/low testosterone levels. Genetic abnormalities (chromosomal) are the congenital cause of this group, and varicocele, orchitis, gonadotoxins (chemotherapy/radiation), trauma/torsion and idiopathic reasons are the acquired causes of these cases.
The spermatogenesis process requires high levels of intra-testicular testosterone. The aromatase enzyme converts androgens to estrogens in men. Aromatase inhibitors block this conversion and have a potential role in NOA individuals (18). Antiestrogens and gonadotropins are also used in the treatment of this group. Microsurgical reconstruction or sperm retrieval processes that are used in assisted reproductive techniques are the main treatments for men with OA (19).
Para-clinical tests such as hormone and genetic assessments help to understand the causes of azoospermia, especially NOA. Through hormone assessment, the condition can be properly diagnosed and the physician can better initiate hormone therapy. Moreover, these tests can help to predict the success of medical therapy and surgical sperm retrieval (18).
In this study, it was proposed that men with NOA who underwent ICSI would have poorer outcomes in all parameters than men with OA. According to the results, the men with NOA had a significantly lower fertilization and clinical pregnancy rate than the men with OA. The reason for the lower fertilization rate in NOA cases is the early paternal effect, which can be caused by dysregulation and dysfunction of oocyte-activating factors, centrosomes, and cytoskeletal components (20, 21).
It has been shown that miscarriage rates may be higher in men with NOA due to aneuploidy and DNA damage in NOA spermatozoa that may contribute to a late paternal effect, leading to pregnancy loss (20, 22, 23). The results of the present study are similar to those of several other studies that revealed significant higher fertilization rates in the men with OA compared with in those with NOA (11, 24, 25). These results can be explained by the sperm functional impairment in men with NOA, which increases genetic abnormalities in these men (26). However, in research conducted in 2015, no differences were observed in the fertility rate or clinical pregnancy rate between the OA and NOA groups (27). In 2005 a metaanalysis revealed that fertilization rate is lower in NOA cases (5). A retrospective study showed lower pregnancy rates in men with NOA than in men with OA (9). In another study, it was indicated that the clinical pregnancy rate in men with NOA was lower than in men with OA (28). In another comparison of NOA and OA outcomes, the implantation rate was found to be lower in the NOA group (29).
Factors that can affect the outcome of ICSI when using non-ejaculated sperm include the azoospermia etiology, the age of the female partner, and the sperm status (fresh or thawed) (30). A younger maternal age has been found to have a positive effect on the fertilization and clinical pregnancy rates of OA men (30). However, some studies have suggested that maternal age does not impact fertilization rates but only affects pregnancy rates (13, 31). Overall, both men with OA and NOA can have successful pregnancies. More research is required to understand the impact of variables such as maternal age and paternal effect on the fertilization rate and miscarriage in men with OA and NOA. Finding and understanding more about factors that affect ICSI outcomes can help us to predict the outcome of fertility procedures and advise our cases better.
5. Conclusion
This study confirmed previous findings that men with OA had significantly higher fertilization and biochemical pregnancy rates than men with NOA. The live birth rate was higher in men with OA, but this difference was not significant.
Acknowledgements
We thank all our patients and their relatives. This research was financially supported by the Research and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Conflict of Interest
There is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Andrology
References
1. Oehninger S. Place of intracytoplasmic sperm injection in management of male infertility. Lancet 2001; 357: 2068-2069. [DOI:10.1016/S0140-6736(00)05223-5]
2. Vahidi S, Ardalan A, Mohammad K. Prevalence of primary infertility in the Islamic Republic of Iran in 2004-2005. Asia Pac J Public Health 2009; 21: 287-293. [DOI:10.1177/1010539509336009] [PMID]
3. Jarow JP, Espeland MA, Lipshultz LI. Evaluation of the azoospermic patient. J Urol 1989; 142: 62-65. [DOI:10.1016/S0022-5347(17)38662-7]
4. Van Peperstraten A, Proctor ML, Johnson NP, Philipson G. Techniques for surgical retrieval of sperm prior to ICSI for azoospermia. Cochrane Database Syst Rev 2008; 2008: CD002807.
5. Ghanem M, Bakr NI, Elgayaar MA, El Mongy Sh, Fathy H, Ibrahim AHA. Comparison of the outcome of intracytoplasmic sperm injection in obstructive and non‐obstructive azoospermia in the first cycle: A report of case series and meta‐analysis. Int J Androl 2005; 28: 16-21. [DOI:10.1111/j.1365-2605.2005.00491.x] [PMID]
6. Esteves SC, Miyaoka R, Agarwal A. An update on the clinical assessment of the infertile male. Clinics 2011; 66: 691-700. [DOI:10.1590/S1807-59322011000400026] [PMID] [PMCID]
7. Donoso P, Tournaye H, Devroey P. Which is the best sperm retrieval technique for non-obstructive azoospermia? A systematic review. Hum Reprod Update 2007; 13: 539-549. [DOI:10.1093/humupd/dmm029] [PMID]
8. Deruyver Y, Vanderschueren D, Van der Aa F. Outcome of microdissection TESE compared with conventional TESE in non‐obstructive azoospermia: A systematic review. Andrology 2014; 2: 20-24. [DOI:10.1111/j.2047-2927.2013.00148.x] [PMID]
9. Verza Jr S, Esteves SC. Sperm defect severity rather than sperm source is associated with lower fertilization rates after intracytoplasmic sperm injection. Int Braz J Urol 2008; 34: 49-56. [DOI:10.1590/S1677-55382008000100008] [PMID]
10. Kanto S, Sugawara J, Masuda H, Sasano H, Arai Y, Kyono K. Fresh motile testicular sperm retrieved from nonobstructive azoospermic patients has the same potential to achieve fertilization and pregnancy via ICSI as sperm retrieved from obstructive azoospermic patients. Fertil Steril 2008; 90: 2010. e5-e7. [DOI:10.1016/j.fertnstert.2008.01.049] [PMID]
11. Vernaeve V, Tournaye H, Osmanagaoglu K, Verheyen G, Van Steirteghem A, Devroey P. Intracytoplasmic sperm injection with testicular spermatozoa is less successful in men with nonobstructive azoospermia than in men with obstructive azoospermia. Fertil Steril 2003; 79: 529-533. [DOI:10.1016/S0015-0282(02)04809-4]
12. Esteves SC, Agarwal A. Reproductive outcomes, including neonatal data, following sperm injection in men with obstructive and nonobstructive azoospermia: Case series and systematic review. Clinics 2013; 68 (Suppl.): 141-150. [DOI:10.6061/clinics/2013(Sup01)16]
13. Bocca S, Moussavi V, Brugh V, Morshedi M, Stadtmauer L, Oehninger S. ICSI outcomes in men undergoing TESE for azoospermia and impact of maternal age. Andrologia 2017; 49: e12617. [DOI:10.1111/and.12617] [PMID]
14. Vahidi S, Moein MR, Yazdinejad F, Ghasemi-Esmailabad S, Narimani N. Iranian temporal changes in semen quality during the past 22 years: A report from an infertility center. Int J Reprod BioMed 2020; 18: 1059-1064. [DOI:10.18502/ijrm.v18i12.8027] [PMID] [PMCID]
15. Vahidi S, Narimani N, Ghanizadeh T, Yazdinejad F, Emami M, Mehravaran K, et al. The short abstinence may have paradoxical effects on sperms with different level of DNA integrity: A prospective study. Urol J 2021; in Press.
16. Pandit S, Sharma R. Non invasive assessment of human oocytes and embryos in assisted reproduction: Review on present practices and future trends. Medical Journal Armed Forces India 2021; in Press. [DOI:10.1016/j.mjafi.2021.04.002]
17. Wang F, Meng TG, Li J, Hou Y, Luo SM, Schatten H, et al. Mitochondrial Ca2+ Is related to mitochondrial activity and dynamic events in mouse oocytes. Front Cell Dev Biol 2020; 8: 1110. [DOI:10.3389/fcell.2020.585932] [PMID] [PMCID]
18. Alkandari MH, Zini A. Medical management of non-obstructive azoospermia: A systematic review. Arab Journal of Urology 2021; 19: 1-6. [DOI:10.1080/2090598X.2021.1956233] [PMID] [PMCID]
19. Schlegel PN, Berkeley AS, Goldstein M, Cohen J, Alikani M, Adler A, et al. Epididymal micropuncture with in vitro fertilization and oocyte micromanipulation for the treatment of unreconstructable obstructive azoospermia. Fertil Steril 1994; 61: 895-901. [DOI:10.1016/S0015-0282(16)56703-X]
20. Barroso G, Valdespin C, Vega E, Kershenovich R, Avila R, Avendaño C, et al. Developmental sperm contributions: Fertilization and beyond. Fertil Steril 2009; 92: 835-848. [DOI:10.1016/j.fertnstert.2009.06.030] [PMID]
21. Oehninger S. Clinical management of male infertility in assisted reproduction: ICSI and beyond. Int J Androl 2011; 34: e319-e329. [DOI:10.1111/j.1365-2605.2011.01143.x] [PMID]
22. Avendaño C, Oehninger S. DNA fragmentation in morphologically normal spermatozoa: How much should we be concerned in the ICSI era? Journal of Andrology 2011; 32: 356-363. [DOI:10.2164/jandrol.110.012005] [PMID]
23. Tesarik J, Greco E, Mendoza C. Late, but not early, paternal effect on human embryo development is related to sperm DNA fragmentation. Hum Reprod 2004; 19: 611-615. [DOI:10.1093/humrep/deh127] [PMID]
24. Fahmy I, Mansour R, Aboulghar M, Serour G, Kamal A, Tawab NA, et al. Intracytoplasmic sperm injection using surgically retrieved epididymal and testicular spermatozoa in cases of obstructive and non‐obstructive azoospermia. Int J Androl 1997; 20: 37-44. [DOI:10.1046/j.1365-2605.1997.00103.x] [PMID]
25. Palermo GD, Schlegel PN, Hariprashad JJ, Ergün B, Mielnik A, Zaninovic N, et al. Fertilization and pregnancy outcome with intracytoplasmic sperm injection for azoospermic men. Hum Reprod 1999; 14: 741-748. [DOI:10.1093/humrep/14.3.741] [PMID]
26. Silber Sh, Escudero T, Lenahan K, Abdelhadi I, Kilani Z, Munne S. Chromosomal abnormalities in embryos derived from testicular sperm extraction. Fertil Steril 2003; 79: 30-38. [DOI:10.1016/S0015-0282(02)04407-2]
27. Vloeberghs V, Verheyen G, Haentjens P, Goossens A, Polyzos N, Tournaye H. How successful is TESE-ICSI in couples with non-obstructive azoospermia? Hum Reprod 2015; 30: 1790-1796. [DOI:10.1093/humrep/dev139] [PMID]
28. Friedler S, Raziel A, Strassburger D, Schachter M, Soffer Y, Ron-El R. Factors influencing the outcome of ICSI in patients with obstructive and non-obstructive azoospermia: A comparative study. Hum Reprod 2002; 17: 3114-3121.
https://doi.org/10.1093/humrep/17.9.2356 [DOI:10.1093/humrep/17.12.3114]
29. Aboulghar MA, Mansour RT, Serour GI, Fahmy I, Kamal A, Tawab NA, et al. Fertilization and pregnancy rates after intracytoplasmic sperm injection using ejaculate semen and surgically retrieved sperm. Fertil Steril 1997; 68: 108-111. [DOI:10.1016/S0015-0282(97)81484-7]
30. Ubaldi F, Nagy ZP, Rienzi L, Tesarik J, Anniballo R, Franco G, et al. Reproductive capacity of spermatozoa from men with testicular failure. Hum Reprod 1999; 14: 2796-2800. [DOI:10.1093/humrep/14.11.2796] [PMID]
31. Silber SJ, Nagy Z, Devroey P, Camus M, Van Steirteghem AC. The effect of female age and ovarian reserve on pregnancy rate in male infertility: Treatment of azoospermia with sperm retrieval and intracytoplasmic sperm injection. Hum Reprod 1997; 12: 2693-2700. [DOI:10.1093/humrep/12.12.2693] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
