
International Journal of
Reproductive Biomedicine
Thu, Apr 25, 2024
[Archive]
Volume 2, Issue 2 (7-2004)
IJRM 2004, 2(2): 74-77 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghafourzadeh M, Karimi M, Karimazadeh M A, Bokai M. Comparison between Two Methods of Ovulation Induction: Clomiphene alone and Clomiphene +Tamoxifen in PCOS Patients. IJRM 2004; 2 (2) :74-77
URL: http://ijrm.ir/article-1-19-en.html
URL: http://ijrm.ir/article-1-19-en.html


Full-Text [PDF 140 kb]
(511 Downloads)
| Abstract (HTML) (3215 Views)
Full-Text: (347 Views)
Introduction
Infertility is defined as a one-year unprotected intercourse which does not result in pregnancy (Jonathan 2002). 10 to 15 percent of couples face with this problem during their reproductive age (Hamilton et al., 1999). Half the causes of infertility are due to female infertility and infertility treatment are time consuming and expensive (Speroff 1999). Anovulation disorders cause 30 to 40 percent of infertility cases (Jonathan 2002). This problem can be seen in women as chronic anovulation (PCO) (Buckley and Goo 2000; Shoham et al., 1999). Treatments are “helping ovulation through anti-estrogenic (Borenstein et al., 2001; ESHRE 1999). Agents like clomiphene and tamoxifen”. These drugs occupy the estrogenic receptors in hypotalamus which then cause the increase in gonadotropin secretion.
Previous studies reported 80% ovulation rate and 40% pregnancy rate after the prescription of clomiphene (50 mg oral) from day 5 to 9 of the menstruation cycle (Hull 1999). One reason for the low pregnancy rate was due to the effects of clomiphen on cervical mucus (Borenstein et al., 2001). In order to decrease the antiestrogenic effect, 20 mg of tamoxifen was prescribed for 5-9
day of the menstrual cycle. Tamoxifen has a similar mechanism to clomiphene but has less negative effects on cervical mucus (Nicholas and Macklon 2000; Fox et al., 2000). Lack of response to the clomiphene treatment leads to more expensive and serious treatments like IUI and IVF (Tajima 1997; WU.C.H. 1997). The aim of the study was to investigate the effects of two drug treatment regimens: higher dose of clomiphene and a combination of lower dose of clomiphene and tamoxifen in treating infertile women with PCO.

Materials and Methods
This was a randomized clinical trial study conducted on 100 PCO infertile patients who had normal hysterosalpangography and whose husbands had normal semen analysis according to WHO criteria. Since previous treatments with clomiphene (3 courses or more) had failed, they were referred to Yazd infertility clinic between 2001-2003, Patients were randomly divided into two groups: The first group received 100 mg (Table II) clomiphen from day 5-9 of the menstrual cycle. The second group received 50 mg (Table I) of clomiphen + 20 mg tamoxifen, from day 5-9 of the menstrual cycle.
The women in this research were between 18-39 years old with amenorrhea or oligomenrrhea and who often with hirsutism; and none of them suffered from cushing and adrenal hyperplasia (Buvat et al., 2001). As
confirmed by paraclinic test, sonography and pregnancy test.
Body Mass Index (BMI), the duration of infertility and duration of drug treatment were also measured. Response to treatment was the development of at least one dominant follicle (>20 mm) and a positive pregnancy test. Data analysis was done by SPSS software. The statistical test were chi-square, fisher - exact test and T-test. P.Value was considered to be significant if < 0.05.
Results
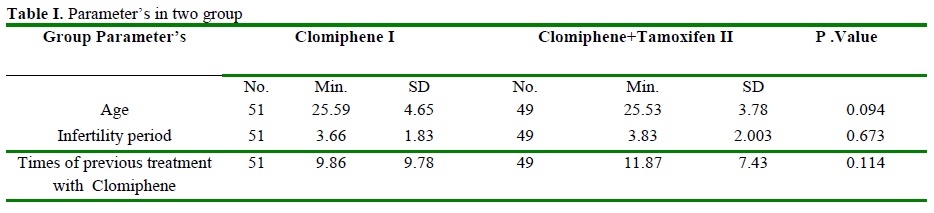
According to age parameter, the average age of both groups did not have any significant difference (P.V= 0.094). Years of infertility and duration of drug administration did not result in any significant improvement in fertility rate (table I). The presence of a dominant follicle in second group who used Clomiphene + Tamoxifen was a little more (73.5%) than the first group (Clomiphene with higher dose) (54.5%) but this difference was not significant (Table II). The rate of positive pregnancy test, in second group was higher (61.3%) than first group (39.2%) and the difference between the two groups was significant (P< 0.05).
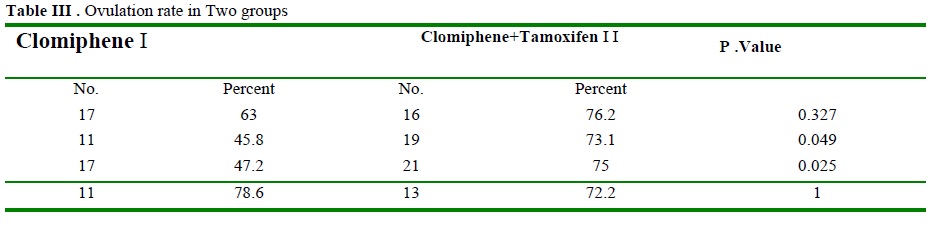
The presence of a dominant follicle in the two treatment groups among women aged between 18-24 was not significant, but in women aged between 25-39 was significant (PV= 0.049) (Table III). BMI affected the results of treatment with 20-
26.99 in second group than the first group. The patients with lower BMI had a better development of dominant follicle (P.Value < 0.05). In women with BMI ³ 27 in both groups, no significant difference in dominant follicle was seen (P.Value @ 1).
Rate of positive pregnancy test was studied based on age and BMI parameters (Table IV).

Discussion
This study show that there was no significant difference in development of dominant follicle in both groups. The result of this study was similar to .Janicke and Estofans (Jonicke et al., 2000). They had reported 62.9% ovulation with clomiphen and 56.2% with Clomiphene + Tamoxifen But there were no significant differences. Researchers believe that Tamoxifen is as effective as Clomiphen in the development of a single dominant follicle. The results also support Robert and Jain’s study who did not find any significant differences in the administration of the two drug regimens.
In Axelrod and Goldzieheve’s study the results was different, so that, the ovulation rate with Clomiphene was higher than with Tamoxifen + Clomiphene (Goldziehev and Axelrod 1998).
In Clomiphene + Tamoxifen group positive pregnancy cases were more than the Clomiphene only group. Robert and Wach’s (1999) study had the same result. In their study there was no significant difference on ovulation rate between
two treatment groups. However Borestein and Shohan’s study showed that the pregnancy rate increased by Tamoxifen significantly (Shoham 1999).
According to the results of this study, Tamoxifen + clomiphene increase the ovulation rate only in age group of 25 to 39 years old with 20£BMI£26.99 women. Thus age assumes to play a significant role in ovulation rate. In overweight women, adding tamoxifen to clomiphen did not increase ovulation, did not produce a single dominant follicle and did not yield a positive pregnancy test rate.
Thus the treatment choice is to administer a combination of Tamoxifen and Clomiphene for 35-39 year old women with 20£BMI£26.99 before administering gonadotropins treatment in PCOS with or without IUI.
Infertility is defined as a one-year unprotected intercourse which does not result in pregnancy (Jonathan 2002). 10 to 15 percent of couples face with this problem during their reproductive age (Hamilton et al., 1999). Half the causes of infertility are due to female infertility and infertility treatment are time consuming and expensive (Speroff 1999). Anovulation disorders cause 30 to 40 percent of infertility cases (Jonathan 2002). This problem can be seen in women as chronic anovulation (PCO) (Buckley and Goo 2000; Shoham et al., 1999). Treatments are “helping ovulation through anti-estrogenic (Borenstein et al., 2001; ESHRE 1999). Agents like clomiphene and tamoxifen”. These drugs occupy the estrogenic receptors in hypotalamus which then cause the increase in gonadotropin secretion.
Previous studies reported 80% ovulation rate and 40% pregnancy rate after the prescription of clomiphene (50 mg oral) from day 5 to 9 of the menstruation cycle (Hull 1999). One reason for the low pregnancy rate was due to the effects of clomiphen on cervical mucus (Borenstein et al., 2001). In order to decrease the antiestrogenic effect, 20 mg of tamoxifen was prescribed for 5-9
day of the menstrual cycle. Tamoxifen has a similar mechanism to clomiphene but has less negative effects on cervical mucus (Nicholas and Macklon 2000; Fox et al., 2000). Lack of response to the clomiphene treatment leads to more expensive and serious treatments like IUI and IVF (Tajima 1997; WU.C.H. 1997). The aim of the study was to investigate the effects of two drug treatment regimens: higher dose of clomiphene and a combination of lower dose of clomiphene and tamoxifen in treating infertile women with PCO.
Materials and Methods
This was a randomized clinical trial study conducted on 100 PCO infertile patients who had normal hysterosalpangography and whose husbands had normal semen analysis according to WHO criteria. Since previous treatments with clomiphene (3 courses or more) had failed, they were referred to Yazd infertility clinic between 2001-2003, Patients were randomly divided into two groups: The first group received 100 mg (Table II) clomiphen from day 5-9 of the menstrual cycle. The second group received 50 mg (Table I) of clomiphen + 20 mg tamoxifen, from day 5-9 of the menstrual cycle.
The women in this research were between 18-39 years old with amenorrhea or oligomenrrhea and who often with hirsutism; and none of them suffered from cushing and adrenal hyperplasia (Buvat et al., 2001). As
confirmed by paraclinic test, sonography and pregnancy test.
Body Mass Index (BMI), the duration of infertility and duration of drug treatment were also measured. Response to treatment was the development of at least one dominant follicle (>20 mm) and a positive pregnancy test. Data analysis was done by SPSS software. The statistical test were chi-square, fisher - exact test and T-test. P.Value was considered to be significant if < 0.05.
Results
According to age parameter, the average age of both groups did not have any significant difference (P.V= 0.094). Years of infertility and duration of drug administration did not result in any significant improvement in fertility rate (table I). The presence of a dominant follicle in second group who used Clomiphene + Tamoxifen was a little more (73.5%) than the first group (Clomiphene with higher dose) (54.5%) but this difference was not significant (Table II). The rate of positive pregnancy test, in second group was higher (61.3%) than first group (39.2%) and the difference between the two groups was significant (P< 0.05).
The presence of a dominant follicle in the two treatment groups among women aged between 18-24 was not significant, but in women aged between 25-39 was significant (PV= 0.049) (Table III). BMI affected the results of treatment with 20-
26.99 in second group than the first group. The patients with lower BMI had a better development of dominant follicle (P.Value < 0.05). In women with BMI ³ 27 in both groups, no significant difference in dominant follicle was seen (P.Value @ 1).
Rate of positive pregnancy test was studied based on age and BMI parameters (Table IV).
Discussion
This study show that there was no significant difference in development of dominant follicle in both groups. The result of this study was similar to .Janicke and Estofans (Jonicke et al., 2000). They had reported 62.9% ovulation with clomiphen and 56.2% with Clomiphene + Tamoxifen But there were no significant differences. Researchers believe that Tamoxifen is as effective as Clomiphen in the development of a single dominant follicle. The results also support Robert and Jain’s study who did not find any significant differences in the administration of the two drug regimens.
In Axelrod and Goldzieheve’s study the results was different, so that, the ovulation rate with Clomiphene was higher than with Tamoxifen + Clomiphene (Goldziehev and Axelrod 1998).
In Clomiphene + Tamoxifen group positive pregnancy cases were more than the Clomiphene only group. Robert and Wach’s (1999) study had the same result. In their study there was no significant difference on ovulation rate between
two treatment groups. However Borestein and Shohan’s study showed that the pregnancy rate increased by Tamoxifen significantly (Shoham 1999).
According to the results of this study, Tamoxifen + clomiphene increase the ovulation rate only in age group of 25 to 39 years old with 20£BMI£26.99 women. Thus age assumes to play a significant role in ovulation rate. In overweight women, adding tamoxifen to clomiphen did not increase ovulation, did not produce a single dominant follicle and did not yield a positive pregnancy test rate.
Thus the treatment choice is to administer a combination of Tamoxifen and Clomiphene for 35-39 year old women with 20£BMI£26.99 before administering gonadotropins treatment in PCOS with or without IUI.
Type of Study: Original Article |
References
1. Borenstein R., Shoham Z., Yemini M., Barosh A., Fienstein M., Rozenman D. (2001) Tamoxifen treatment in women with failure of clomiphene citrate therapy. Aus N Z J Obstet Gynecol, 29(2): 173-5. [DOI:10.1111/j.1479-828X.1989.tb01711.x] [PMID]
2. Buckley M.M., and Goo K.L. (2000) Tamoxifen, Areappraisel of its Pharmacodynamic and pharmacokinetic propertics, and therapeutic use. Drugs 37(4): 451-9. [DOI:10.2165/00003495-198937040-00004] [PMID]
3. Buvat J., Buvat - Herbout M., Marcolin G. (2001) Ardaens Boulierk. Antiestrogens as treatment of female and male infertilities. Horm Res 28(2-4) : 219-29. [DOI:10.1159/000180947] [PMID]
4. ESHRE. (1999) Female infertility: Treatment options for complicated cases. The ESHRE capri workshop. Hum Reprod 12: 1191-6. [DOI:10.1093/humrep/12.6.1191] [PMID]
5. Fox R., Corrigan E., Thomas P.A., Hull M.G.R. (2000) the diagnosis of polycystic ovarian in women with menstrual disorder. Fertil Steril 66: 761-4.
6. Franks S. (2001) Medical progress article: Polycytic ovary syndrome. N Eng J Med 333: 853-61. [DOI:10.1056/NEJM199509283331307] [PMID]
7. Fukushima J., Tajimue C., Fuknma K., Maejama M. (2001) Tamoxifen in the treatment of infertility associated with luteal phase deficiency. Fertile Steril 37(6) 755-61. [DOI:10.1016/S0015-0282(16)46334-X]
8. Goldziehev J.W., Axelrod L.R. (1998) Clinical and biochemical features of polycystic ovarian disease. Fertil Steril 14: 631-53. [DOI:10.1016/S0015-0282(16)35047-6]
9. Hamilton - Fairley D., Kiddy D., Watson H., Paterson C., Franks S. (1999) Association of moderate obesity with poor pregnancy outcome in women with polycystic ovary syndrome. Br J Obstet Gynaecol 99 : 128 -31. [DOI:10.1111/j.1471-0528.1992.tb14470.x] [PMID]
10. Hull M.G.R. (1999) Epidemiology of infertility and polycystic ovarian disease: Endocrinological and demographic studies. Gynecol Endocrinol 235: 45.
11. Hull M.G.R. (1999) Epidemiology of infertility and polycystic ovarian disease: Endocrinological and demographic studies. Gynecol Endocrinol 1: 235: 45. [DOI:10.3109/09513598709023610] [PMID]
12. Jonathan S. (2002) Berek. Novak's textbook of gynecology. Williams & Wilkins 25: 840-852.
13. Jonicke F., Estofen D., Boos H., Bottger I. (2000) Endocrine fertility - restricting factors in clomiphene therapy. Ceburtshilf franenhalked 46(4) : 228-33.
14. Leon Speroff. (1999) Clinical Gyneacologic Endocrinology and Infertility. Lippinicon Williams & Wilkins12: 490.
15. Messini I.E., Nillius S.J. (1998) Compersion between tamoxifen and clomiphene for induction ovulation . Acta obstet Gynecol Scand 61(4): 377-9.
16. Nicholas S., Macklon. (2000) Optimizing protocols for ovulation induction.Female infertility therapy. MARTIN DUNITZ 7:76.
17. Robert Boostnfar M.D., John K. Jain M.D. (2001) A prospective randomized trial comparing clomiphen citrate with Tamoxifen Citrate for ovulation induction. Fertility and Sterility 75:(5) 1024-1026. [DOI:10.1016/S0015-0282(01)01749-6]
18. Shoham Z., Borenstein R., Lunenfeld B., Pariente C. (1999) Hormonal profiles following clomiphene citrate therapy in conception and nonconception cycles. Clin Endocrinol 33: 271-8. [DOI:10.1111/j.1365-2265.1990.tb00491.x] [PMID]
19. Tajima C. (1996) Endocrine profile in tamoxifen , Induced conception cycle. Fertil Steril 42(4): 548-53. [DOI:10.1016/S0015-0282(16)48137-9]
20. Tajima C. (1997) Tamoxifen in the treatment of infertile patiants associated with in adequate luteal phase. Fertile Steril 41(3): 470-72. [DOI:10.1016/S0015-0282(16)47730-7]
21. Tsuiki A., Uchara S., Kyono K., Satio A., Hoshi K. (1998) Induction of ovulation with an estrogen antagonist Tamoxifen. Tohoku J Exp Med 144(1): 21-23. [DOI:10.1620/tjem.144.21] [PMID]
22. WU.C.H. (1997) Less Miscarriage in pregnancy following tamoxifen treatment of infertile patients with luteal phase dysfunction as compared to clomiphene treatment. Early pregnancy 3(4): 301-5.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
