
International Journal of
Reproductive Biomedicine
Mon, Jul 27, 2026
[Archive]
Volume 1, Issue 1 (1-2003)
IJRM 2003, 1(1): 16-19 |
Back to browse issues page

![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Aflatoonian A, Aflatoonian R, Khashavi Z. Comparison between Transvaginal Sonography and Cytological results for detection of ovarian cysts. IJRM 2003; 1 (1) :16-19
URL: http://ijrm.ir/article-1-2-en.html
URL: http://ijrm.ir/article-1-2-en.html


Full-Text [PDF 36 kb]
(931 Downloads)
| Abstract (HTML) (3432 Views)
Full-Text: (643 Views)
Introduction
Transvaginal aspiration of ovarian follicles under ultrasound guidance has been practiced for years, since the safety of this method has been established. Ovarian cyst aspiration remains controversial due to: malignant cells spill into the peritoneal eavity, which lead into further spread of cancer, and low sensitivity of cytopathology for malignacy (Maylenand Silverberg, 1990; Kozlowski, 1909; kapposic, 2002; Kurjak, 2002). This concern assumes importance because incidence of ovarian carcinoma in reproductive age is 1.1%. (Maylen and Silverberg, 1990). On the other hand, most common pelvic mass in reproductive age is functional cyst which may cause torsion, leakage, rapture, or anxiety for patient about pathology of mass. In addition, some endocrinologists believe that presence of simple ovarian cyst in early follicular phase may be influence the follicular maturation and quality of in IVF cycles. These persuade physicians to premature surgical therapy which results in ovarian and tubal adhesions and subefficient ovarian reserve with subsequent defects in fertility potentials (Kozlowski, 1909). Wat reported 45% By additional imaging study such as pelvic infertility development in patients who had operated on for adnexal cystic mass. According to Wat’s study, surgery for unnecessary cases would decrease fertility (Kocak,1998).
Ultrasound, CT Scan, MRI or doppler flow, it is possible to predict risk of malignancy of a tumor or being benign (Maylen and Silverberg, 1990; Jabra et al., 1993). Thus, a new scoring system with extreme sensitivity and positive predictive value for predicting benign cyst by ultrasound might be more efficient for reducing unnecessary surgery. There are some studies concerning the accuracy of aspiration cytology compare to biopsy of ovarian cyst wall, as Sevin and Nadjer who reported 94.5% diagnostic accuracy for benign ovarian cyst (Salat, 1992). According to Finkler et al. (1996) study: accuracy of transvaginal sonography for predicting the benign nature of a tumor was 96%. The most important parameter in ultrasound observation was presence of vegetation. In this study accuracy of diagnosis was documented by pathology (Diernaes, 1987). We have designed this study to evaluate accuracy of ultrasound for diagnosis of benign ovarian cysts in comparision with cytology of cyst’s fluid which was aspirated transvaginally.
Material and Methods
This cross sectional study which takes 9 months was done in Madar Hospital of Yazd. Among admitted patients with complains such as AUB, pelvic, abdominal pain, or infertility who had ovarian cyst in ultrasound, 82 cases were found with these criteria. The age was between 15-49 years with well defined border cystic lesions without septation or papillary projection or solid part, smaller than 10cm and resolution didn't occur afterHD OC pills taking for 3 months.
Informed consent was obtained from all patients after
detailed information about the procedure was given. Transvaginal probe with needle guide attachment was used after preparing of patient under general anesthesia in lithotomy position. A no. 20 needle was used for aspiration of cyst, then the aspirated fluid was delivered to the cytopathology lab for further cytological examination. All characteristics of ultrasound view of cyst and fluid was recorded in flow chart.
From 82 patients, there were with drown from our study due to missed cytology reports. A chi-square and extended fisher exact test was applied for statistical
analysis by SPSS.


Results
56.1% of the patients were in age group of 25 to 44 years. 12.2% of the cases had already ovarian surgery such as ophorectomy (3.7%) or cystectomy (8.5%). 79% of the patients had regular menstruation, and 69.5% of them had infertility: 47.5% with primary infertility and 22% with secondary infertility.
This study showed in functional cysts: unilocular in sonographic view was: 90.2% - Bilocular view was 6.1% and 3.7% had multiluculer view. All endometrioma (100%) were
unilocular, and epithelial cysts showed unilocular (66.6%) and Bilocular (33.3%) in sonography.
Accuracy
These results showed: ultrasound has 96.8% sensitivity of and 86.6% of specifity on functional cyst diagnosis. 100% specifity and 97% sensitivity on diagnosis endometrioma.33.3% sensitivity and 100% specifity on Benign epithelial cyst. diagnosis. Overall: 95% sensitivity and 77% specifity on discriminating type of Benign ocyst (Table I).
Echolucency
95.4% of sonolucent cysts were functional, and 4.6% of sonolucent cysts were bnign epithelial cyst. Homogen echogen view was seen in endometrioma (85.7%) and benign epithelial cysts (14.3%) (Table II).
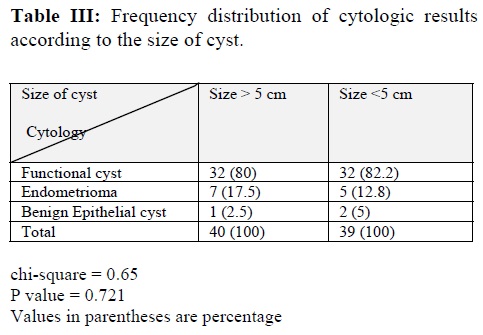
Size
size of cyst less than 10 cm didn't affect on quality of cyst. 50% of cysts were greater than 5cm and 50% of them were lesser than 5cm (Table III).
Color
Color of functional cyst was light yellow and clear white. Also, color of benign epithelial cyst was yellow and clear white. While, the Color of endometrioma was chocolate like color (Table IV).

Discussion
Transvagianal ultrasound–guided aspiration of benign ovarian cyst, proposed as an alternative method for laparoscopy and surgical excision (Kozlowski, 1909). Wat et al. (1970) reported that infertility developed in 45% of the 36 patients he had operated on for adnexal cystic masses. Threy further claimed that surgery should not be the first step in the treatment of ovarian cysts with benign criteria on ultrasound. Due to advantage of this method, which does not require hospitalization and general anesthesia compared to laparoscopy or laparatomy in some cases (Kocak, 1998). Ultrasound are generally used for discriminating the benign from malignant lesions, also to determine the histological type of tumors (Kapposic, 2002). Criteria for this distinguish includes: Size of the tumor number of loculi, presence of septation, inward papillary excrescence from outer rim of the mass, overall echodensity, and Doppler pulsatility index (Kapposic, 2002). If all the other ultrasound parameters are reassuring; however, a unilocular lesion without internal echo or papillary excrecences is highly unlikely to be malignant regardless of the size or age of patient (Kapposic, 2002).
Presence of septations creating a multilocular pattern increases the liklihood of cancer up to 8%. And presence of solid components increases to 70%, thickness of septation more than 0.3mm proving to be malignant (87.5) but this parameter is less useful criteria than papillary projection in the cystic masses, particulaly in postmenopausal subjects, are highly suggestive of malignancy up to 93%. This criterion is more relevant to the malignant than internal solid echo which could be seen dermoid cyst, the most with all echodensity (Geatije and Poop, 1994).
Diemases et al (1987) reported on the use of preoparation ultrasound and cytology in evaluating of ovarian cyst of 89 cysts evaluated. They showed that ultrasound alone had a positive predictive value of 40% and negative predictive value of 98%, cytology alone had a negative predictive value of 91% and positive predictive value of 67%. when ultrasound and cytology were used together all malignant lesions were identified preoperatively (Salat, 1992).These findings were confirmed by De Crosping et al. and Hermann et al. Therefore, ultrasound appears to be more accurate in identifying benign cysts than malignant ones . However, if a malignant cyst is aspirated, the risk of complications is as low as (0.55%) (Diernaes, 1987). Although, there may be some theoretical complication related to the transvaginal aspiration, such as peritonitis due to microbial contamination, spillage of the malignant cells, perforation of blood vessels or intestine, or spillage of endometrial content which may cause in Pelvic Inflammatory Disease (PID). Our results support the finding which was observed by Kocak et al which no complication happened in these studies. Hurwitz et al (1988) have offered transvaginal- ultrasound guided aspiration of benign ovarian cyst. De Crespingny et al (1985) suggested this method for managing these cysts. Ultrasound by itself is a valuable tool in ruling out of
malignancy and has a negative predictive value of 94 to 96%. However, adding doppler flow mapping and blood flow velocimetry make further improvement upon the positive predictive value (Hansmann,1985).
Taking all the above criteria together, it seems that if a mass appears benign by ultrasound morphology criteria and doppler PI, probability of it being malignant is very close to zero and can be aspirated by transvaginal route without any fear from missing of malignacy (Maylen, 1990; Kocak, 1998).
In contrast to our suggestion, recurrence of cysts after aspiration, either transvaginal or with laparoscopy, may be as high as 50%. This must be considered for long term effect on endocrine function and future fertility. This finding needs more investigation and data to be confirmed (Zanetta and Gerards, 1996; Novak, 2002). Spillage of endometrial content in peritoneal cavity may cause in PID, but this assumption was rejected in regard to our study as well as others (Kocak, 1998). In conclusion, the results of this study showed the accuracy of sonography as an accurate diagnostic tool for ovarian cyst.
Transvaginal aspiration of ovarian follicles under ultrasound guidance has been practiced for years, since the safety of this method has been established. Ovarian cyst aspiration remains controversial due to: malignant cells spill into the peritoneal eavity, which lead into further spread of cancer, and low sensitivity of cytopathology for malignacy (Maylenand Silverberg, 1990; Kozlowski, 1909; kapposic, 2002; Kurjak, 2002). This concern assumes importance because incidence of ovarian carcinoma in reproductive age is 1.1%. (Maylen and Silverberg, 1990). On the other hand, most common pelvic mass in reproductive age is functional cyst which may cause torsion, leakage, rapture, or anxiety for patient about pathology of mass. In addition, some endocrinologists believe that presence of simple ovarian cyst in early follicular phase may be influence the follicular maturation and quality of in IVF cycles. These persuade physicians to premature surgical therapy which results in ovarian and tubal adhesions and subefficient ovarian reserve with subsequent defects in fertility potentials (Kozlowski, 1909). Wat reported 45% By additional imaging study such as pelvic infertility development in patients who had operated on for adnexal cystic mass. According to Wat’s study, surgery for unnecessary cases would decrease fertility (Kocak,1998).
Ultrasound, CT Scan, MRI or doppler flow, it is possible to predict risk of malignancy of a tumor or being benign (Maylen and Silverberg, 1990; Jabra et al., 1993). Thus, a new scoring system with extreme sensitivity and positive predictive value for predicting benign cyst by ultrasound might be more efficient for reducing unnecessary surgery. There are some studies concerning the accuracy of aspiration cytology compare to biopsy of ovarian cyst wall, as Sevin and Nadjer who reported 94.5% diagnostic accuracy for benign ovarian cyst (Salat, 1992). According to Finkler et al. (1996) study: accuracy of transvaginal sonography for predicting the benign nature of a tumor was 96%. The most important parameter in ultrasound observation was presence of vegetation. In this study accuracy of diagnosis was documented by pathology (Diernaes, 1987). We have designed this study to evaluate accuracy of ultrasound for diagnosis of benign ovarian cysts in comparision with cytology of cyst’s fluid which was aspirated transvaginally.
Material and Methods
This cross sectional study which takes 9 months was done in Madar Hospital of Yazd. Among admitted patients with complains such as AUB, pelvic, abdominal pain, or infertility who had ovarian cyst in ultrasound, 82 cases were found with these criteria. The age was between 15-49 years with well defined border cystic lesions without septation or papillary projection or solid part, smaller than 10cm and resolution didn't occur afterHD OC pills taking for 3 months.
Informed consent was obtained from all patients after
detailed information about the procedure was given. Transvaginal probe with needle guide attachment was used after preparing of patient under general anesthesia in lithotomy position. A no. 20 needle was used for aspiration of cyst, then the aspirated fluid was delivered to the cytopathology lab for further cytological examination. All characteristics of ultrasound view of cyst and fluid was recorded in flow chart.
From 82 patients, there were with drown from our study due to missed cytology reports. A chi-square and extended fisher exact test was applied for statistical
analysis by SPSS.
Results
56.1% of the patients were in age group of 25 to 44 years. 12.2% of the cases had already ovarian surgery such as ophorectomy (3.7%) or cystectomy (8.5%). 79% of the patients had regular menstruation, and 69.5% of them had infertility: 47.5% with primary infertility and 22% with secondary infertility.
This study showed in functional cysts: unilocular in sonographic view was: 90.2% - Bilocular view was 6.1% and 3.7% had multiluculer view. All endometrioma (100%) were
unilocular, and epithelial cysts showed unilocular (66.6%) and Bilocular (33.3%) in sonography.
Accuracy
These results showed: ultrasound has 96.8% sensitivity of and 86.6% of specifity on functional cyst diagnosis. 100% specifity and 97% sensitivity on diagnosis endometrioma.33.3% sensitivity and 100% specifity on Benign epithelial cyst. diagnosis. Overall: 95% sensitivity and 77% specifity on discriminating type of Benign ocyst (Table I).
Echolucency
95.4% of sonolucent cysts were functional, and 4.6% of sonolucent cysts were bnign epithelial cyst. Homogen echogen view was seen in endometrioma (85.7%) and benign epithelial cysts (14.3%) (Table II).
Size
size of cyst less than 10 cm didn't affect on quality of cyst. 50% of cysts were greater than 5cm and 50% of them were lesser than 5cm (Table III).
Color
Color of functional cyst was light yellow and clear white. Also, color of benign epithelial cyst was yellow and clear white. While, the Color of endometrioma was chocolate like color (Table IV).
Discussion
Transvagianal ultrasound–guided aspiration of benign ovarian cyst, proposed as an alternative method for laparoscopy and surgical excision (Kozlowski, 1909). Wat et al. (1970) reported that infertility developed in 45% of the 36 patients he had operated on for adnexal cystic masses. Threy further claimed that surgery should not be the first step in the treatment of ovarian cysts with benign criteria on ultrasound. Due to advantage of this method, which does not require hospitalization and general anesthesia compared to laparoscopy or laparatomy in some cases (Kocak, 1998). Ultrasound are generally used for discriminating the benign from malignant lesions, also to determine the histological type of tumors (Kapposic, 2002). Criteria for this distinguish includes: Size of the tumor number of loculi, presence of septation, inward papillary excrescence from outer rim of the mass, overall echodensity, and Doppler pulsatility index (Kapposic, 2002). If all the other ultrasound parameters are reassuring; however, a unilocular lesion without internal echo or papillary excrecences is highly unlikely to be malignant regardless of the size or age of patient (Kapposic, 2002).
Presence of septations creating a multilocular pattern increases the liklihood of cancer up to 8%. And presence of solid components increases to 70%, thickness of septation more than 0.3mm proving to be malignant (87.5) but this parameter is less useful criteria than papillary projection in the cystic masses, particulaly in postmenopausal subjects, are highly suggestive of malignancy up to 93%. This criterion is more relevant to the malignant than internal solid echo which could be seen dermoid cyst, the most with all echodensity (Geatije and Poop, 1994).
Diemases et al (1987) reported on the use of preoparation ultrasound and cytology in evaluating of ovarian cyst of 89 cysts evaluated. They showed that ultrasound alone had a positive predictive value of 40% and negative predictive value of 98%, cytology alone had a negative predictive value of 91% and positive predictive value of 67%. when ultrasound and cytology were used together all malignant lesions were identified preoperatively (Salat, 1992).These findings were confirmed by De Crosping et al. and Hermann et al. Therefore, ultrasound appears to be more accurate in identifying benign cysts than malignant ones . However, if a malignant cyst is aspirated, the risk of complications is as low as (0.55%) (Diernaes, 1987). Although, there may be some theoretical complication related to the transvaginal aspiration, such as peritonitis due to microbial contamination, spillage of the malignant cells, perforation of blood vessels or intestine, or spillage of endometrial content which may cause in Pelvic Inflammatory Disease (PID). Our results support the finding which was observed by Kocak et al which no complication happened in these studies. Hurwitz et al (1988) have offered transvaginal- ultrasound guided aspiration of benign ovarian cyst. De Crespingny et al (1985) suggested this method for managing these cysts. Ultrasound by itself is a valuable tool in ruling out of
malignancy and has a negative predictive value of 94 to 96%. However, adding doppler flow mapping and blood flow velocimetry make further improvement upon the positive predictive value (Hansmann,1985).
Taking all the above criteria together, it seems that if a mass appears benign by ultrasound morphology criteria and doppler PI, probability of it being malignant is very close to zero and can be aspirated by transvaginal route without any fear from missing of malignacy (Maylen, 1990; Kocak, 1998).
In contrast to our suggestion, recurrence of cysts after aspiration, either transvaginal or with laparoscopy, may be as high as 50%. This must be considered for long term effect on endocrine function and future fertility. This finding needs more investigation and data to be confirmed (Zanetta and Gerards, 1996; Novak, 2002). Spillage of endometrial content in peritoneal cavity may cause in PID, but this assumption was rejected in regard to our study as well as others (Kocak, 1998). In conclusion, the results of this study showed the accuracy of sonography as an accurate diagnostic tool for ovarian cyst.
Type of Study: Original Article |
References
1. Brown DL, Doublet PM. (1998) Benign and malignant ovarian masses. Radiology 208: 103-110. [DOI:10.1148/radiology.208.1.9646799] [PMID]
2. De crespingy L. CH. (1998) Ultrasound guided puncture for gynecology and pelvic lesion. Australian and newzealand J of OBGy; 25-227. [DOI:10.1111/j.1479-828X.1985.tb00650.x] [PMID]
3. Diernaes E Rassmussen. (1987) Ovarian cyst management by puncture . Lancet 168-173. [DOI:10.1016/S0140-6736(87)90503-4]
4. Finkler et al. (1996) Management of ovarian cyst: BMJ 313-1103. [DOI:10.1136/bmj.313.7065.1103a] [PMID]
5. Geatije R, Poop L.W. (1994) Is differention of benign and mailgnant cystic adnexal masses . Acta OBGy scandinavica 73: 502-507. [DOI:10.3109/00016349409013440] [PMID]
6. Hansmann M. (1985) Ultrasound diagnosis in Gyncology. Radiology J 132: 1186-1190.
7. Kocak I, Auzel (1998) An evaluation of transvaginal ultrasound. guided aspiration of simple adnexal mass. Journal of OBGY 18: 103-108. [DOI:10.1080/01443619866822] [PMID]
8. Jabra AA, Fishman Ek, Taylor G.A. (1993) Primary ovarian tumors evaluation clin Imaging 17: 199-203. [DOI:10.1016/0899-7071(93)90110-9]
9. Kozlowski KJ. (1999) Ovarian Masses. Adoles Med 10: 335-37.
10. Kurjak A, Kupesic, (2002) Color dopller of malignant adnexal mass 21,22: 191-203.
11. Maylen M. silverberg M. (1990) Ovarian cyst aspiration. J of IVF-ET 7: 1536-1543.
12. Novak, S. (2002) Ovarian cancer, Jonatan. S.Br Gynecology Textbook. Lippincont Williams and Wilkins 32: 376.
13. Prasap kumar. (2001) Transvaginal ultra sonography in ovarian pathology, Rajan R, philadelphia W.B. textbook of ultrasound in OBGyn sandes company 30: 229.
14. Rajan R. (1993) Changing concept in gyncologycal diagnosis J. OBGYN 43: 1130-38.
15. Salat, Baroux. (1992) Manage of ovarian cysts. Biritish medical J l 313: 6031-37.
16. Zanetta, Gerards. (1996) Role of puncture and aspiration in expectant management- British Medical J 313: 7065-7069. [DOI:10.1136/bmj.313.7065.1110] [PMID] [PMCID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
