
International Journal of
Reproductive Biomedicine
Sun, Jul 13, 2025
[Archive]
Volume 20, Issue 5 (May 2022)
IJRM 2022, 20(5): 377-388 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi N, Fallahzadeh H, Dafei M, Sadeghi M, Mirzaei M. Evaluation of multiple linear regression function and generalized linear model types in estimating natural menopausal age: A cross-sectional study. IJRM 2022; 20 (5) :377-388
URL: http://ijrm.ir/article-1-2100-en.html
URL: http://ijrm.ir/article-1-2100-en.html



1- Department of Statistics and Epidemiology, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Sadeghi.stat89@ gmail.com (+98)09387786951
2- Research Center of Prevention and Epidemiology of Non-Communicable Diseases, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd-Iran. Fallahzadeh.ho@gmail.com (+98)09131529486 ,Fallahzadeh.ho@gmail.com
3- Research Center for Nursing and Midwifery Care, School of Nursing and Midwifery, Shahid Sadoughi University of Medical Sciences Yazd-Iran. maryam_dafei@yahoo.com (+98)09132588499
4- Ferdowsi University of Mashhad, Faculty of Mathematical Sciences, Mashhad, Iran. Sadeghi.maryam@mail.um.ac.ir (+98)09378099979
5- Center for Healthcare Data Modeling, Departments of Biostatistics and Epidemiology, School of public health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Masoud_mirzaei@hotmail.com (+98) 09134509917
2- Research Center of Prevention and Epidemiology of Non-Communicable Diseases, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd-Iran. Fallahzadeh.ho@gmail.com (+98)09131529486 ,
3- Research Center for Nursing and Midwifery Care, School of Nursing and Midwifery, Shahid Sadoughi University of Medical Sciences Yazd-Iran. maryam_dafei@yahoo.com (+98)09132588499
4- Ferdowsi University of Mashhad, Faculty of Mathematical Sciences, Mashhad, Iran. Sadeghi.maryam@mail.um.ac.ir (+98)09378099979
5- Center for Healthcare Data Modeling, Departments of Biostatistics and Epidemiology, School of public health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Masoud_mirzaei@hotmail.com (+98) 09134509917
Full-Text [PDF 377 kb]
(1089 Downloads)
| Abstract (HTML) (1587 Views)
1. Introduction
Natural menopause comes after a permanent cease of menstruation for 12 months with a decrease of blood estrogen levels and an increase of follicle-stimulating hormone, which results in cessation of ovarian follicular development (1-3). This natural transition occurs in almost all women without any pathological or physiological causes (2). Evidence shows that the age at natural menopause differed among different races, so the mean age of menopause was 51.4 and 49-50 yr in western and Asian women, respectively (3). According to the literature in previous studies, menopause is associated with factors such as socioeconomic status, physical activity, marital status, education level, fertility history, etc. However, various factors can affect the age of natural menopause across the world (2, 4). With the onset of menopause, biochemical and hormonal changes occur, such as decreased estrogen hormone levels that cause behavioral (5) and physical disorders (6, 7). The premature or late occurrence of these changes may bring about premature menopause or late-onset menopause increasing the risk of having certain diseases in women. According to previous studies, early menopause correlates with an increased mortality rate caused by cardiovascular diseases (8, 9) and osteoporosis (10). While late menopause increases the risk of ovarian (11, 12), uterus (13), and breast cancers (14, 15).
Since women spend about one-third of their lifespan in menopause, accurate prediction of the age of natural menopause and its effective parameters are crucial to increase women's life expectancy (3). In medical data analysis, it is not always possible to establish regression assumptions. For example, it is possible that the response variable does not have a normal distribution, and even with different transformations by the researcher, a normal distribution for the response variable is not obtained. In these cases, generalized linear models (GLM) can be used due to less sensitivity when predicting than establishing regression assumptions. To the best of our knowledge, very few studies applied GLM to determine menopause age. The GLM models formed in 3 steps. In the first step, a suitable distribution for the response variable is determined, which could be a member of the exponential family. For example, for variables with the continuous response, Gaussian, Gamma, and Gaussian inverse distributions could be included. The second step is about the formation of the systematic component. This component is created by the linear combination of the predictor variables. The third step included applying the link function to establish a relationship between the random and systematic components (16-18).
Since regression assumptions are important for the ordinary least squares (OLS) model, in the absence of these assumptions, a common method before GLM models was to use transformations to normalize the distribution of the variable y-response and the variance stability. Nonetheless, for most types of data, such as medical data, it is difficult to find a transformation that stabilizes the variance in addition to the ability to normalize the data. In such cases, the type of transformation for normalization is usually different from the best transformation for variance stability. Another advantage of the GLM model is that the selection of the link function is different from the selection of the random component in this model. In the GLM model, the link function does not need to stabilize the variance and normalize the data. The fitting process does not limit this choice to the normal distribution by increasing the probability of choosing the probability distribution for Y.
These advantages of GLM models can be important for data from medical studies because regression assumptions cannot be established by conventional methods in some cases, and prediction error increases if these assumptions are not established, and the OLS models are used (19).
This study aims to compare the performance of various GLMs and OLS methods in predicting the age of natural menopause in a large population of Iranian women. We also examined and compared GLM and OLS in estimating the natural menopausal age and its effective factors.
2. Materials and Methods
In this cross-sectional study, the data of 1706 women who were experienced menopause, registered in the Shahedieh Cohort study, Yazd, Iran from April 2015 to September 2017 were extracted.
The Shahedieh cohort study is a part of the PERSIAN cohort. The cohort study was carried out in Shahedieh, Zarch, and Ashkezar cities of Yazd due to homogeneity among people regarding a limited number of immigrants and emigrants, homogenous ethnicity, and local cooperation.
After establishing equipping the cohort center, the human resources were employed, and the research officers' team was trained to collect the required information. To collect the research data, residents of Shahedieh City who had 35-70 yr of age were required to refer to the predetermined health centers. Later, the participants' information was collected using a standardized questionnaire. Further information about the standardized questionnaire and PERSIAN Cohort can be found in related research (20). The inclusion criterion of this study was the women aged 35-70 yr who experienced menopause (21). The exclusion criteria were as follow: women with other menopausal etiology including breastfeeding, hormonal disorders, surgeries like hysterectomy or oophorectomy (22) and the individuals who had answered the question “Was your menopause a natural one?” No. After excluding the above-mentioned participants, a total of 1251 women participated in the study.
In this study, independent variables on the menopausal age were measured considering the present variables in cohort questionnaires, which included demographic characteristics (e.g., age, education level, and marital status), fertility history, body mass index (BMI), waistline, individual habits, social and economic status, physical activity, employment status, and some chronic illnesses. The participants' age was calculated when their entrance to the research. Based on the participants' last educational degree, the level of education was categorized into 5 groups: 1) illiterate, 2) elementary, 3) secondary, 4) high school, and 5) academic.
Single participants were 1 in 1251, and only 8 widows were reported. Therefore, due to a very limited number of samples, the singles, widows, and divorcees were merged into 1 group resulting in 2 main categories of 1) married and 2) widow/divorcee/single.
The participants' fertility history included the natural menopause age, menarche age, age at the first pregnancy, intake of oral contraceptives, number of pregnancies, use of infertility-related medications, history of salpingectomy and infertility.
The natural menopausal age was defined as the person's age at her last menstrual period that occurred after 12 months of menstruation (without pregnancy, lactation, etc.), and the menarche age was the age at first menstruation. Other variables included the use of oral contraceptives, salpingectomy history, infertility history, and intake of infertility-related medications, which were evaluated using 2 levels of Yes/No. Unfortunately, no data was found in the cohort profile concerning the period of using oral contraceptives and the dosage of other related medications for infertility treatment. The questionnaire sufficed to only one yes/no question that asked them whether they had used the medications or not. Thus there was no opportunity to examine such data in the present study.
The participants' BMI was also obtained by dividing weight in kilograms by square meters of height in meters (kg/m2). This variable was categorized under 3 levels of 1) ≤ 24.99 kg/m2, 2) 25-29.99 kg/m2, 3) ≥ 30 kg/m2. The waistline was measured in cm individually. The socio-economic status questionnaire contained questions including the highest educational qualification, housing status, number of households, and home facilities. After gathering data, the participants were classified as weak, moderate, and strong about their socio-economic status using the clustering method. The international physical activity questionnaires were administered to assess each individual's physical activity. The validity and reliability of this questionnaire were confirmed in Iran. The multiples of the resting metabolic rate (MET) were measured according to the international questionnaire for each individual.
According to this questionnaire, the total energy gain ranging from 0-599 (MET-min/wk) shows poor physical activity, from 600-3000 (MET-min/wk) indicates moderate physical activity, and higher than 3000 (MET-min/wk) represents severe physical activity. Individual habits include 2 variables of drug use, hookah, which were investigated using Yes/No levels. Smoking cigarettes is considered improper in Iran and Islamic culture accordingly among the 1251 women, even less than 5 were reported as smokers. Since this included smoking hookah, we merged them all with hookah smokers in 1 group. The period and the amount of usage were not asked in the questionnaire.
Chronic diseases considered in this study included the history of diabetes, cardiac ischemic, thyroid, kidney stones, gallstones, rheumatism, chronic headache, and depression. Since menopause begins 3-5 yr before its occurrence, we studied individuals whose diseases were diagnosed at least 4 yr before menopausal age.
2.1. Ethical considerations
The research proposal was approved by the Ethics Committee of School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.SPH.REC.1397.066).
2.2. Statistical analysis
Statistical analyses were performed using R software, version 3.6.2 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) and SPSS software version 24 (IBM Corporation, Armonk, NY, USA).
To compare the mean age at menopause among different levels of variables which were categorized in 2-groups and multi-groups; in cases where the age at menopause was normal at each level of the variable, the parametric t test and ANOVA test were carried out respectively, however, in cases where the age wasn’t normal, the nonparametric Mann-Whitney U-test and Kruskal-Wallis test were carried out. The correlation between the quantitative variables and the menopausal age was measured using the Pearson correlation coefficient. A significance level of 5% is considered. Aiming to investigate the impact of probable influential variables on menopausal age, the multiple linear regression method was applied using OLS and GLMs.
Multiple linear regression using the OLS technique is common in predicting natural menopausal age. However, the GLM is more general than the linear model since, in GLM, the response variable can have abnormal distribution. Moreover, the mean response variable can have a non-linear relationship with the predictor variables. Linear regression is a special case of GLM. To the best of our knowledge, very few studies applied GLM to determine menopausal age. The GLM models were formed in 3 steps. In the first step, we identified a suitable distribution for the response variable, which could be a member of the exponential family. Since menopause is a positive and continuous variable, GLM models were applied in this study, such as Gaussian, Gamma, and Gaussian inverse distributions. The second step was about the formation of the systematic component. This component was formed by a linear combination of the predictor variables. The third step included applying the link function to establish a relationship between the random and systematic components. The systematic component can hold any real number, but the variable can accept specific numbers as a subset of real numbers. An appropriate link function selection allows the prediction range to be within the response variable range. The log link function is an efficient link function for non-negative data (16-18).
The classic presumptions of regression were examined to conduct the multiple linear regression method with the OLS technique. The normality of menopausal age was examined utilizing Skewness and Kurtosis measures. The variance inflation factor was applied to identify the correlation between variables. If the variance inflation factor were greater than 10, a coincidence would exist between the independent variables (23).
The performance of regression models was examined by comparing them to each other using the Akaike information criterion (AIC) and also the root-mean-square error (RMSE) and mean absolute error (MAE) for measuring the error amount.
The AIC shows the extent of data loss by applying the considered statistical model. The MAE is the MAE between the predicted and observed menopausal age, and finally. The RMSE is the root mean square error of the predicted and observed menopausal age difference (24-26).
3. Results
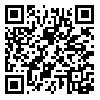
This cross-sectional cohort study investigated 1251 women who experienced natural menopause. The mean age was 58.7 ± 6.3 yr (95% CI: 59.0-58.3). Furthermore, the mean natural menopause age was 49.1 ± 4.7 yr (95% CI: 48.8-49.3) with a median of 50 yr. According to the results of univariate analysis, mean natural menopause age was significant across the educational levels, salpingectomy, infertility, diabetes, cardiovascular diseases, depression.
Illiterate people have devoted the highest mean age of menopause. Also, a history of salpingectomy, diabetes, ischemic heart disease, depression, and a history of infertility was accompanied by an increase and decrease in mean age at menopause, respectively (Table I).
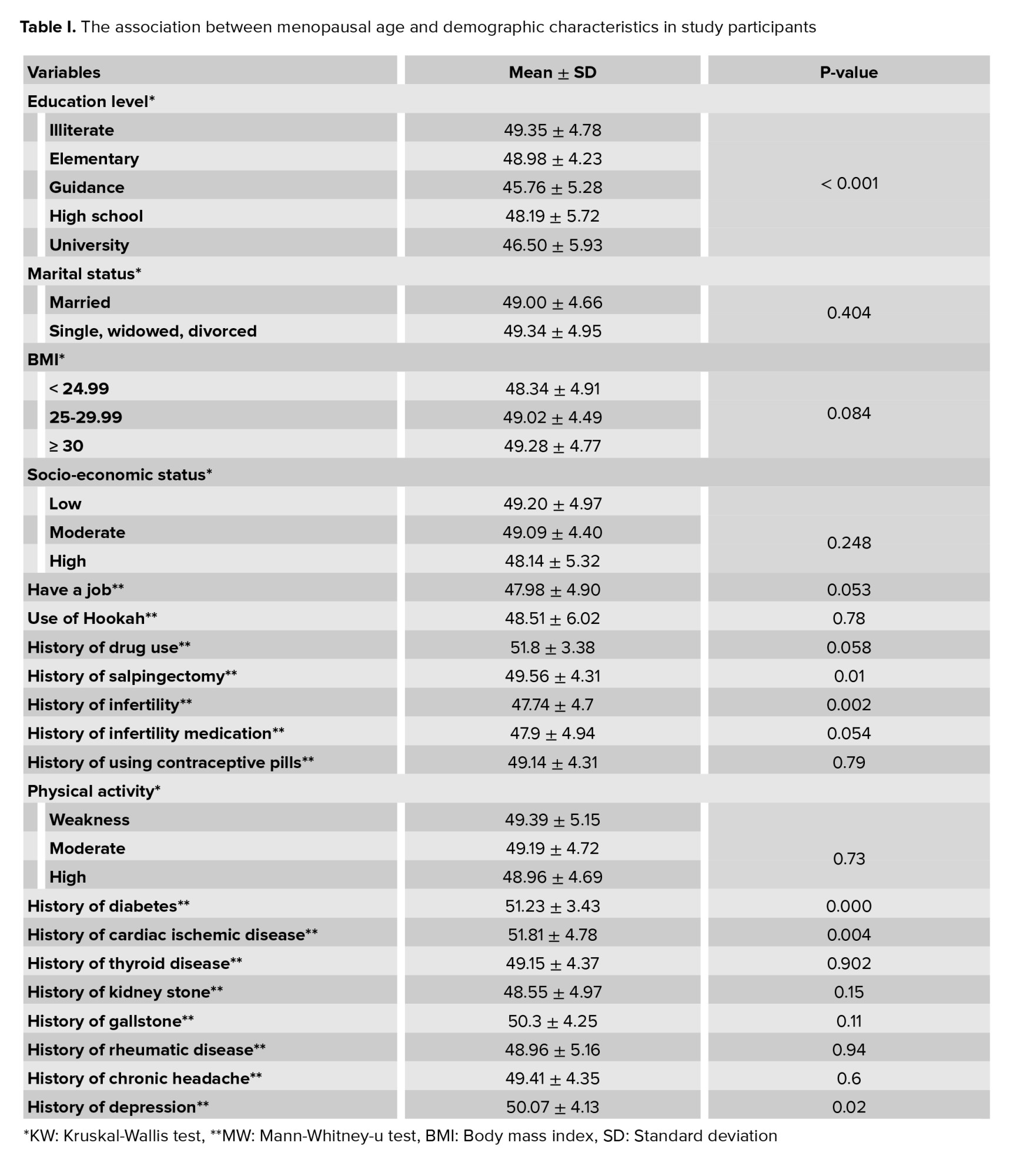
As the found results claimed, the age of menopause has a direct and significant relationship with the number of pregnancies and the waistline. To put it in other words, with an increase in the number of pregnancies or the waistline, the age of menopause increases (Table II).
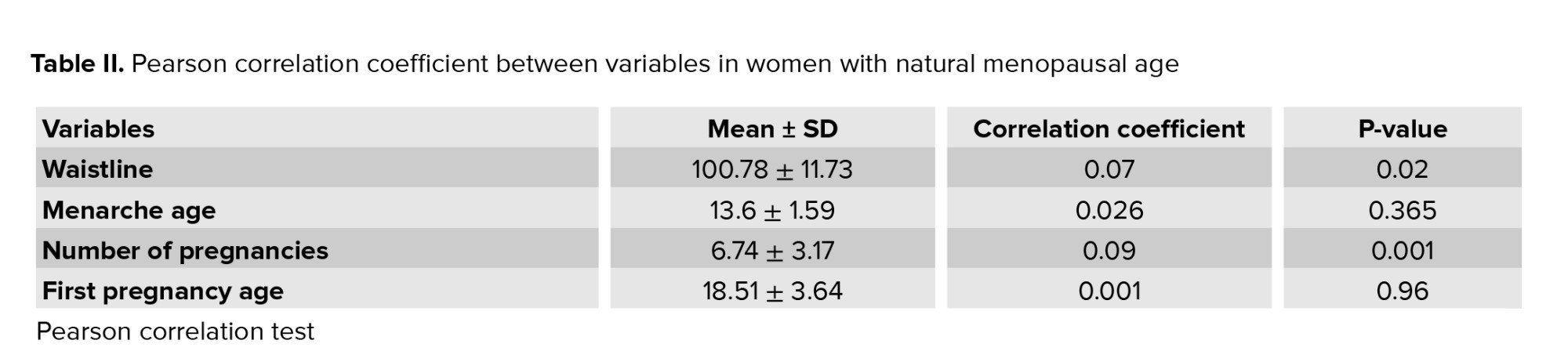
In all regression models, education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age (Table III).
In a multiple linear regression model with the OLS technique, the age at menopause for the participant with an educational level of secondary decreases by -3.58. Also, in cases where the people had a history of salpingectomy, diabetes, cardiac ischemic, and depression, the menopausal age increases by 0.65, 2.04, 2.62, and 1.03, respectively (Table III).
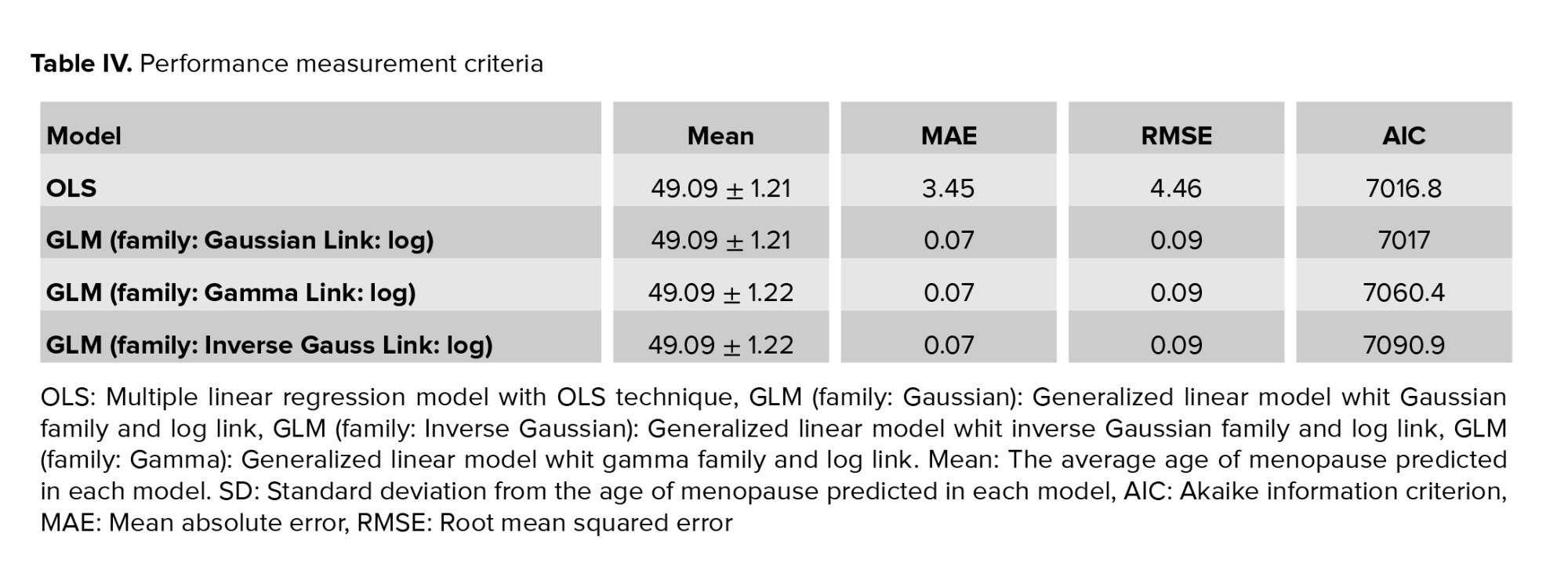
Table IV shows the performance measurement criteria of MAE, RMSE, and AIC in each model. According to table IV, the MAE and RMSE amounts were found to be remarkably higher in multiple linear models with the OLS technique compared to GLM models. The AIC of the multiple linear models was almost the same as for the GLM with the Gaussian family.
The distribution of menopausal age was illustrated in figure 1. The skewness and kurtosis of the natural menopausal age were from -2 to 2, which indicated the normal distribution of this variable.
4. Discussion
The mean and standard deviation of the menopausal age in our participants were 49 and 4.7 yr (95% CI: 48.8-49.3) and a median of 50 yr. The results of multivariable analysis showed that education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age.
This mean was higher than the reported menopausal age of Yazd women (47.4) in 2007 (25). The achieved mean score for this region had been within the reported menopausal age range in Iran since 2004 (46.9-49.6) (3). Menopausal age was reported as 47.4, 48.6, 46.57, 48.3, and 49.6 yr in some cities of Iran, including Yazd, Isfahan, Tehran, Shiraz, and Hamadan, respectively (3, 25, 26). In general, menopausal age in Iran is lower than in developed countries due to socio-economic status and lifestyle factors (3). The univariate analysis using parametric and nonparametric tests showed that educational level, waistline, number of previous pregnancies, and the history of salpingectomy, infertility, diabetes, cardiac ischemic, and depression had a statistically significant effect on the menopausal age (p ≤ 0.05). The multiple linear regression model using the OLS technique showed that education at the secondary school level had a significant association with menopausal age. Since high education levels affect lifestyle, pregnancy health, and self-care, some studies indicated that menopausal age was higher in women with higher levels of education (27).
However, such a result was not found in the present study (25); we found that higher education had a negative coefficient in the regression equation. This may be due to the low number of higher education levels. Some studies confirmed the relationship between BMI and menopausal age (28, 29). But in the present study, this association was not significant, consistent with some previous studies in Iran. Furthermore no relationship was found between the waistline and menopausal age (3, 25). Multiple linear regression analysis showed no association between marital status and menopausal age. This was consistent with some studies (2, 3) and contradicted some others (4). According to studies, smoking and hookah have affected the factors such as gonadotropins and steroid hormones and leading to reduce follicle storage and ovarian aging, which is one of the causes of premature menopause (30). But in the present study, no association was found between smoking and hookah use and menopausal age. However, Yang and co-workers reported that smokers were at risk for early menopause (31). Several studies in Iran indicated that smoking was not associated with menopausal age. According to a study in Isfahan, this finding can be attributed to the fact that smoking is a taboo for women in the Islamic culture of Iran; therefore, women may not report it accurately (3, 25).
Furthermore, no relationship was observed between menopausal age and occupation; whereas, Koukouliata and colleagues confirmed this relationship (2). In multiple linear regression model, no association was found between menopausal age and reproductive history factors including menarche age, age at the first pregnancy (3), number of pregnancies, use of oral contraceptives, history of infertility, and use of infertility-related medications, but a significant and direct relationship was found between the history of salpingectomy and menopausal age. However, scarce information is available on the association of salpingectomy with menopausal age.
According to some studies results, regular exercise causes fitness and creates favorable conditions for reproduction and continuation. On the other hand, intense exercises lead to menstrual cycle problems. Hence, the exercise effect in most studies related to menopausal age is noticeable (32).
We observed no significant relationship between physical activity and menopausal age, which is similar to some studies in Iran (3). However, it was found that this relationship was significant over a population in Hamadan (33), which may be due to inaccurate reports of physical activity by participants in our study. The relationship between menopausal age estimation and its related factors in Isfahan was investigated, and it has been found that low socioeconomic status was significantly associated with early menopause (3). However, no significant relationship was observed between socio-economic status and menopausal age. One study have been conducted on some diseases and their impact on menopausal age. Given that menopausal symptoms occur 3-5 yr before menopause begins (34), we included those individuals whose diseases were diagnosed at least 4 yr before menopause. The studied diseases included diabetes, heart failure and angina, thyroid, kidney stones, gallstones, rheumatism, chronic headaches, and depression.
Based on multiple linear regression results, diabetes, cardiac ischemic, and depression were associated with aging in menopause, but some previous studies reported an inverse association between diabetes and menopausal age. In these studies, people with pre-menopausal diabetes were more likely to develop early menopause (35, 36). Considering that few studies were conducted on the relationship between chronic diseases and menopausal age, further studies are needed to establish the relationship between menopausal age and conditions. Likewise, the multiple linear models with the OLS technique, the education level, history of salpingectomy, diabetes, cardiac ischemic, and depression became significant in all GLM models.
The linear model is associated with many assumptions, which sometimes it is difficult or impossible to establish all of them. For example, predictor variables might interact or have a nonlinear relationship with the response variable, and even the response variable might not follow a normal distribution. In these cases, linear models are not necessary and optimal, and GLM models can be used.
A GLM is more general than a linear model because the response variable can have an abnormal or asymmetric distribution in this model. Moreover, the mean of the response variable can have a non-linear relationship with the predictor variables (16).
According to the obtained results, the multiple linear regression model with OLS technique and GLM model with the Gaussian family and the log link function have lower AIC than other models, which indicates their better performance. However, The GLM model with the Gaussian family and the log link function has much lower RMSE and MAE compared to the OLS multiple linear models.
The RMSE is a good criterion for measuring the model's prediction accuracy. If the aim is to predict a variable, it is one of the most essential criteria for model fit. The RMSE is measured in units of similar data, not in square units. The MAE is another criterion for measuring the performance of models. Like RMSE, MAE is also measured in similar units of data. Lower values of RMSE and MAE indicate better model fit.
In the discussion about poorer performance, it can be said that in the 2 models of gamma GLM and inverse Gaussian GLM rather than the OLS and Gaussian GLM models, since the above 2 distributions have better application for the response variable whose data set is continuous, non-negative and owing a positive skew, in the prediction of normal menopausal age, the response variable data set has almost a normal distribution, showing lower performance in this study.
Therefore, considering that the Gaussian GLM model has a better performance than the OLS model, it should be noted that in this model, the Gaussian distribution is a suitable distribution for variable response data sets and is less sensitive to regression assumptions.
Among the difficulties faced throughout the present study, one can note the lack of sufficient data in cohort questionnaire regarding some continuous variables such as the time length of oral contraceptive intake, the time length and the amount of hookah usage, the severity of chronic disease, and the control degree of the chronic diseases. Furthermore, some variables might not have been collected by the specialists after the menopause onset, and the data had been solely what the participant could recall at that time. This could result in deviations to predict the natural menopause age.
Also, in the present study, we were faced with limitations such as low sample size in some qualitative variables and absence of the mother's menopausal age variable.
5. Conclusion
In the present study, the mean and standard deviation of the menopausal age were 49 and 4.7 yr. Then to predict the normal menopause age, the GLM model with the Gaussian family and the log link function with decreasing RMSE and MAE can be a good alternative for modeling natural menopausal age and this model showed that education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age.
Acknowledgments
This article is extracted from a master's thesis and financially supported by Shahid Sadoughi University of Medical Sciences, Yazd, Iran (grant number: 6089).
Conflict of Interest
The authors declare that there is no conflict of interest in this study.
Full-Text: (281 Views)
1. Introduction
Natural menopause comes after a permanent cease of menstruation for 12 months with a decrease of blood estrogen levels and an increase of follicle-stimulating hormone, which results in cessation of ovarian follicular development (1-3). This natural transition occurs in almost all women without any pathological or physiological causes (2). Evidence shows that the age at natural menopause differed among different races, so the mean age of menopause was 51.4 and 49-50 yr in western and Asian women, respectively (3). According to the literature in previous studies, menopause is associated with factors such as socioeconomic status, physical activity, marital status, education level, fertility history, etc. However, various factors can affect the age of natural menopause across the world (2, 4). With the onset of menopause, biochemical and hormonal changes occur, such as decreased estrogen hormone levels that cause behavioral (5) and physical disorders (6, 7). The premature or late occurrence of these changes may bring about premature menopause or late-onset menopause increasing the risk of having certain diseases in women. According to previous studies, early menopause correlates with an increased mortality rate caused by cardiovascular diseases (8, 9) and osteoporosis (10). While late menopause increases the risk of ovarian (11, 12), uterus (13), and breast cancers (14, 15).
Since women spend about one-third of their lifespan in menopause, accurate prediction of the age of natural menopause and its effective parameters are crucial to increase women's life expectancy (3). In medical data analysis, it is not always possible to establish regression assumptions. For example, it is possible that the response variable does not have a normal distribution, and even with different transformations by the researcher, a normal distribution for the response variable is not obtained. In these cases, generalized linear models (GLM) can be used due to less sensitivity when predicting than establishing regression assumptions. To the best of our knowledge, very few studies applied GLM to determine menopause age. The GLM models formed in 3 steps. In the first step, a suitable distribution for the response variable is determined, which could be a member of the exponential family. For example, for variables with the continuous response, Gaussian, Gamma, and Gaussian inverse distributions could be included. The second step is about the formation of the systematic component. This component is created by the linear combination of the predictor variables. The third step included applying the link function to establish a relationship between the random and systematic components (16-18).
Since regression assumptions are important for the ordinary least squares (OLS) model, in the absence of these assumptions, a common method before GLM models was to use transformations to normalize the distribution of the variable y-response and the variance stability. Nonetheless, for most types of data, such as medical data, it is difficult to find a transformation that stabilizes the variance in addition to the ability to normalize the data. In such cases, the type of transformation for normalization is usually different from the best transformation for variance stability. Another advantage of the GLM model is that the selection of the link function is different from the selection of the random component in this model. In the GLM model, the link function does not need to stabilize the variance and normalize the data. The fitting process does not limit this choice to the normal distribution by increasing the probability of choosing the probability distribution for Y.
These advantages of GLM models can be important for data from medical studies because regression assumptions cannot be established by conventional methods in some cases, and prediction error increases if these assumptions are not established, and the OLS models are used (19).
This study aims to compare the performance of various GLMs and OLS methods in predicting the age of natural menopause in a large population of Iranian women. We also examined and compared GLM and OLS in estimating the natural menopausal age and its effective factors.
2. Materials and Methods
In this cross-sectional study, the data of 1706 women who were experienced menopause, registered in the Shahedieh Cohort study, Yazd, Iran from April 2015 to September 2017 were extracted.
The Shahedieh cohort study is a part of the PERSIAN cohort. The cohort study was carried out in Shahedieh, Zarch, and Ashkezar cities of Yazd due to homogeneity among people regarding a limited number of immigrants and emigrants, homogenous ethnicity, and local cooperation.
After establishing equipping the cohort center, the human resources were employed, and the research officers' team was trained to collect the required information. To collect the research data, residents of Shahedieh City who had 35-70 yr of age were required to refer to the predetermined health centers. Later, the participants' information was collected using a standardized questionnaire. Further information about the standardized questionnaire and PERSIAN Cohort can be found in related research (20). The inclusion criterion of this study was the women aged 35-70 yr who experienced menopause (21). The exclusion criteria were as follow: women with other menopausal etiology including breastfeeding, hormonal disorders, surgeries like hysterectomy or oophorectomy (22) and the individuals who had answered the question “Was your menopause a natural one?” No. After excluding the above-mentioned participants, a total of 1251 women participated in the study.
In this study, independent variables on the menopausal age were measured considering the present variables in cohort questionnaires, which included demographic characteristics (e.g., age, education level, and marital status), fertility history, body mass index (BMI), waistline, individual habits, social and economic status, physical activity, employment status, and some chronic illnesses. The participants' age was calculated when their entrance to the research. Based on the participants' last educational degree, the level of education was categorized into 5 groups: 1) illiterate, 2) elementary, 3) secondary, 4) high school, and 5) academic.
Single participants were 1 in 1251, and only 8 widows were reported. Therefore, due to a very limited number of samples, the singles, widows, and divorcees were merged into 1 group resulting in 2 main categories of 1) married and 2) widow/divorcee/single.
The participants' fertility history included the natural menopause age, menarche age, age at the first pregnancy, intake of oral contraceptives, number of pregnancies, use of infertility-related medications, history of salpingectomy and infertility.
The natural menopausal age was defined as the person's age at her last menstrual period that occurred after 12 months of menstruation (without pregnancy, lactation, etc.), and the menarche age was the age at first menstruation. Other variables included the use of oral contraceptives, salpingectomy history, infertility history, and intake of infertility-related medications, which were evaluated using 2 levels of Yes/No. Unfortunately, no data was found in the cohort profile concerning the period of using oral contraceptives and the dosage of other related medications for infertility treatment. The questionnaire sufficed to only one yes/no question that asked them whether they had used the medications or not. Thus there was no opportunity to examine such data in the present study.
The participants' BMI was also obtained by dividing weight in kilograms by square meters of height in meters (kg/m2). This variable was categorized under 3 levels of 1) ≤ 24.99 kg/m2, 2) 25-29.99 kg/m2, 3) ≥ 30 kg/m2. The waistline was measured in cm individually. The socio-economic status questionnaire contained questions including the highest educational qualification, housing status, number of households, and home facilities. After gathering data, the participants were classified as weak, moderate, and strong about their socio-economic status using the clustering method. The international physical activity questionnaires were administered to assess each individual's physical activity. The validity and reliability of this questionnaire were confirmed in Iran. The multiples of the resting metabolic rate (MET) were measured according to the international questionnaire for each individual.
According to this questionnaire, the total energy gain ranging from 0-599 (MET-min/wk) shows poor physical activity, from 600-3000 (MET-min/wk) indicates moderate physical activity, and higher than 3000 (MET-min/wk) represents severe physical activity. Individual habits include 2 variables of drug use, hookah, which were investigated using Yes/No levels. Smoking cigarettes is considered improper in Iran and Islamic culture accordingly among the 1251 women, even less than 5 were reported as smokers. Since this included smoking hookah, we merged them all with hookah smokers in 1 group. The period and the amount of usage were not asked in the questionnaire.
Chronic diseases considered in this study included the history of diabetes, cardiac ischemic, thyroid, kidney stones, gallstones, rheumatism, chronic headache, and depression. Since menopause begins 3-5 yr before its occurrence, we studied individuals whose diseases were diagnosed at least 4 yr before menopausal age.
2.1. Ethical considerations
The research proposal was approved by the Ethics Committee of School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.SPH.REC.1397.066).
2.2. Statistical analysis
Statistical analyses were performed using R software, version 3.6.2 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) and SPSS software version 24 (IBM Corporation, Armonk, NY, USA).
To compare the mean age at menopause among different levels of variables which were categorized in 2-groups and multi-groups; in cases where the age at menopause was normal at each level of the variable, the parametric t test and ANOVA test were carried out respectively, however, in cases where the age wasn’t normal, the nonparametric Mann-Whitney U-test and Kruskal-Wallis test were carried out. The correlation between the quantitative variables and the menopausal age was measured using the Pearson correlation coefficient. A significance level of 5% is considered. Aiming to investigate the impact of probable influential variables on menopausal age, the multiple linear regression method was applied using OLS and GLMs.
Multiple linear regression using the OLS technique is common in predicting natural menopausal age. However, the GLM is more general than the linear model since, in GLM, the response variable can have abnormal distribution. Moreover, the mean response variable can have a non-linear relationship with the predictor variables. Linear regression is a special case of GLM. To the best of our knowledge, very few studies applied GLM to determine menopausal age. The GLM models were formed in 3 steps. In the first step, we identified a suitable distribution for the response variable, which could be a member of the exponential family. Since menopause is a positive and continuous variable, GLM models were applied in this study, such as Gaussian, Gamma, and Gaussian inverse distributions. The second step was about the formation of the systematic component. This component was formed by a linear combination of the predictor variables. The third step included applying the link function to establish a relationship between the random and systematic components. The systematic component can hold any real number, but the variable can accept specific numbers as a subset of real numbers. An appropriate link function selection allows the prediction range to be within the response variable range. The log link function is an efficient link function for non-negative data (16-18).
The classic presumptions of regression were examined to conduct the multiple linear regression method with the OLS technique. The normality of menopausal age was examined utilizing Skewness and Kurtosis measures. The variance inflation factor was applied to identify the correlation between variables. If the variance inflation factor were greater than 10, a coincidence would exist between the independent variables (23).
The performance of regression models was examined by comparing them to each other using the Akaike information criterion (AIC) and also the root-mean-square error (RMSE) and mean absolute error (MAE) for measuring the error amount.
The AIC shows the extent of data loss by applying the considered statistical model. The MAE is the MAE between the predicted and observed menopausal age, and finally. The RMSE is the root mean square error of the predicted and observed menopausal age difference (24-26).
3. Results
This cross-sectional cohort study investigated 1251 women who experienced natural menopause. The mean age was 58.7 ± 6.3 yr (95% CI: 59.0-58.3). Furthermore, the mean natural menopause age was 49.1 ± 4.7 yr (95% CI: 48.8-49.3) with a median of 50 yr. According to the results of univariate analysis, mean natural menopause age was significant across the educational levels, salpingectomy, infertility, diabetes, cardiovascular diseases, depression.
Illiterate people have devoted the highest mean age of menopause. Also, a history of salpingectomy, diabetes, ischemic heart disease, depression, and a history of infertility was accompanied by an increase and decrease in mean age at menopause, respectively (Table I).
As the found results claimed, the age of menopause has a direct and significant relationship with the number of pregnancies and the waistline. To put it in other words, with an increase in the number of pregnancies or the waistline, the age of menopause increases (Table II).
In all regression models, education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age (Table III).
In a multiple linear regression model with the OLS technique, the age at menopause for the participant with an educational level of secondary decreases by -3.58. Also, in cases where the people had a history of salpingectomy, diabetes, cardiac ischemic, and depression, the menopausal age increases by 0.65, 2.04, 2.62, and 1.03, respectively (Table III).
Table IV shows the performance measurement criteria of MAE, RMSE, and AIC in each model. According to table IV, the MAE and RMSE amounts were found to be remarkably higher in multiple linear models with the OLS technique compared to GLM models. The AIC of the multiple linear models was almost the same as for the GLM with the Gaussian family.
The distribution of menopausal age was illustrated in figure 1. The skewness and kurtosis of the natural menopausal age were from -2 to 2, which indicated the normal distribution of this variable.
4. Discussion
The mean and standard deviation of the menopausal age in our participants were 49 and 4.7 yr (95% CI: 48.8-49.3) and a median of 50 yr. The results of multivariable analysis showed that education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age.
This mean was higher than the reported menopausal age of Yazd women (47.4) in 2007 (25). The achieved mean score for this region had been within the reported menopausal age range in Iran since 2004 (46.9-49.6) (3). Menopausal age was reported as 47.4, 48.6, 46.57, 48.3, and 49.6 yr in some cities of Iran, including Yazd, Isfahan, Tehran, Shiraz, and Hamadan, respectively (3, 25, 26). In general, menopausal age in Iran is lower than in developed countries due to socio-economic status and lifestyle factors (3). The univariate analysis using parametric and nonparametric tests showed that educational level, waistline, number of previous pregnancies, and the history of salpingectomy, infertility, diabetes, cardiac ischemic, and depression had a statistically significant effect on the menopausal age (p ≤ 0.05). The multiple linear regression model using the OLS technique showed that education at the secondary school level had a significant association with menopausal age. Since high education levels affect lifestyle, pregnancy health, and self-care, some studies indicated that menopausal age was higher in women with higher levels of education (27).
However, such a result was not found in the present study (25); we found that higher education had a negative coefficient in the regression equation. This may be due to the low number of higher education levels. Some studies confirmed the relationship between BMI and menopausal age (28, 29). But in the present study, this association was not significant, consistent with some previous studies in Iran. Furthermore no relationship was found between the waistline and menopausal age (3, 25). Multiple linear regression analysis showed no association between marital status and menopausal age. This was consistent with some studies (2, 3) and contradicted some others (4). According to studies, smoking and hookah have affected the factors such as gonadotropins and steroid hormones and leading to reduce follicle storage and ovarian aging, which is one of the causes of premature menopause (30). But in the present study, no association was found between smoking and hookah use and menopausal age. However, Yang and co-workers reported that smokers were at risk for early menopause (31). Several studies in Iran indicated that smoking was not associated with menopausal age. According to a study in Isfahan, this finding can be attributed to the fact that smoking is a taboo for women in the Islamic culture of Iran; therefore, women may not report it accurately (3, 25).
Furthermore, no relationship was observed between menopausal age and occupation; whereas, Koukouliata and colleagues confirmed this relationship (2). In multiple linear regression model, no association was found between menopausal age and reproductive history factors including menarche age, age at the first pregnancy (3), number of pregnancies, use of oral contraceptives, history of infertility, and use of infertility-related medications, but a significant and direct relationship was found between the history of salpingectomy and menopausal age. However, scarce information is available on the association of salpingectomy with menopausal age.
According to some studies results, regular exercise causes fitness and creates favorable conditions for reproduction and continuation. On the other hand, intense exercises lead to menstrual cycle problems. Hence, the exercise effect in most studies related to menopausal age is noticeable (32).
We observed no significant relationship between physical activity and menopausal age, which is similar to some studies in Iran (3). However, it was found that this relationship was significant over a population in Hamadan (33), which may be due to inaccurate reports of physical activity by participants in our study. The relationship between menopausal age estimation and its related factors in Isfahan was investigated, and it has been found that low socioeconomic status was significantly associated with early menopause (3). However, no significant relationship was observed between socio-economic status and menopausal age. One study have been conducted on some diseases and their impact on menopausal age. Given that menopausal symptoms occur 3-5 yr before menopause begins (34), we included those individuals whose diseases were diagnosed at least 4 yr before menopause. The studied diseases included diabetes, heart failure and angina, thyroid, kidney stones, gallstones, rheumatism, chronic headaches, and depression.
Based on multiple linear regression results, diabetes, cardiac ischemic, and depression were associated with aging in menopause, but some previous studies reported an inverse association between diabetes and menopausal age. In these studies, people with pre-menopausal diabetes were more likely to develop early menopause (35, 36). Considering that few studies were conducted on the relationship between chronic diseases and menopausal age, further studies are needed to establish the relationship between menopausal age and conditions. Likewise, the multiple linear models with the OLS technique, the education level, history of salpingectomy, diabetes, cardiac ischemic, and depression became significant in all GLM models.
The linear model is associated with many assumptions, which sometimes it is difficult or impossible to establish all of them. For example, predictor variables might interact or have a nonlinear relationship with the response variable, and even the response variable might not follow a normal distribution. In these cases, linear models are not necessary and optimal, and GLM models can be used.
A GLM is more general than a linear model because the response variable can have an abnormal or asymmetric distribution in this model. Moreover, the mean of the response variable can have a non-linear relationship with the predictor variables (16).
According to the obtained results, the multiple linear regression model with OLS technique and GLM model with the Gaussian family and the log link function have lower AIC than other models, which indicates their better performance. However, The GLM model with the Gaussian family and the log link function has much lower RMSE and MAE compared to the OLS multiple linear models.
The RMSE is a good criterion for measuring the model's prediction accuracy. If the aim is to predict a variable, it is one of the most essential criteria for model fit. The RMSE is measured in units of similar data, not in square units. The MAE is another criterion for measuring the performance of models. Like RMSE, MAE is also measured in similar units of data. Lower values of RMSE and MAE indicate better model fit.
In the discussion about poorer performance, it can be said that in the 2 models of gamma GLM and inverse Gaussian GLM rather than the OLS and Gaussian GLM models, since the above 2 distributions have better application for the response variable whose data set is continuous, non-negative and owing a positive skew, in the prediction of normal menopausal age, the response variable data set has almost a normal distribution, showing lower performance in this study.
Therefore, considering that the Gaussian GLM model has a better performance than the OLS model, it should be noted that in this model, the Gaussian distribution is a suitable distribution for variable response data sets and is less sensitive to regression assumptions.
Among the difficulties faced throughout the present study, one can note the lack of sufficient data in cohort questionnaire regarding some continuous variables such as the time length of oral contraceptive intake, the time length and the amount of hookah usage, the severity of chronic disease, and the control degree of the chronic diseases. Furthermore, some variables might not have been collected by the specialists after the menopause onset, and the data had been solely what the participant could recall at that time. This could result in deviations to predict the natural menopause age.
Also, in the present study, we were faced with limitations such as low sample size in some qualitative variables and absence of the mother's menopausal age variable.
5. Conclusion
In the present study, the mean and standard deviation of the menopausal age were 49 and 4.7 yr. Then to predict the normal menopause age, the GLM model with the Gaussian family and the log link function with decreasing RMSE and MAE can be a good alternative for modeling natural menopausal age and this model showed that education, history of salpingectomy, diabetes, cardiac ischemic, and depression were significantly associated with menopausal age.
Acknowledgments
This article is extracted from a master's thesis and financially supported by Shahid Sadoughi University of Medical Sciences, Yazd, Iran (grant number: 6089).
Conflict of Interest
The authors declare that there is no conflict of interest in this study.
Type of Study: Original Article |
Subject:
Fertility & Infertility
References
1. Muka T, Asllanaj E, Avazverdi N, Jaspers L, Stringa N, Milic J, et al. Age at natural menopause and risk of type 2 diabetes: A prospective cohort study. Diabetologia 2017; 60: 1951-1960. [DOI:10.1007/s00125-017-4346-8] [PMID] [PMCID]
2. Koukouliata A, Nena E, Koutlaki N, Liberis V, Constantinidis TC. Correlation of age at natural menopause with occupational status and other epidemiologic factors in women from Prefecture of Kavala, Greece. Hippokratia 2017; 21: 32-37.
3. Golshiri P, Akbari M, Abdollahzadeh MR. Age at natural menopause and related factors in Isfahan, Iran. J Menopausal Med 2016; 22: 87-93. [DOI:10.6118/jmm.2016.22.2.87] [PMID] [PMCID]
4. Costanian Ch, McCague H, Tamim H. Age at natural menopause and its associated factors in Canada: Cross-sectional analyses from the Canadian longitudinal study on aging. Menopause 2018; 25: 265-272. [DOI:10.1097/GME.0000000000000990] [PMID]
5. Gordon JL, Eisenlohr-Moul TA, Rubinow DR, Schrubbe L, Girdler SS. Naturally occurring changes in estradiol concentrations in the menopause transition predict morning cortisol and negative mood in perimenopausal depression. Clin Psychol Sci 2016; 4: 919-935. [DOI:10.1177/2167702616647924] [PMID] [PMCID]
6. Ali AM, Ahmed AH, Smail L. Psychological climacteric symptoms and attitudes toward menopause among Emirati women. Int J Environ Res Public Health 2020; 17: 5028. [DOI:10.3390/ijerph17145028] [PMID] [PMCID]
7. Kozakowski J, Gietka-Czernel M, Leszczyńska D, Majos A. Obesity in menopause: Our negligence or an unfortunate inevitability? Prz Menopauzalny 2017; 16: 61-65. [DOI:10.5114/pm.2017.68594] [PMID] [PMCID]
8. Muka T, Oliver-Williams C, Kunutsor S, Laven JSE, Fauser BCJ, Chowdhury R, et al. Association of age at onset of menopause and time since onset of menopause with cardiovascular outcomes, intermediate vascular traits, and all-cause mortality: A systematic review and meta-analysis. JAMA Cardiol 2016; 1: 767-776. [DOI:10.1001/jamacardio.2016.2415] [PMID]
9. Rahman I, Åkesson A, Wolk A. Relationship between age at natural menopause and risk of heart failure. Menopause 2015; 22: 12-16. [DOI:10.1097/GME.0000000000000261] [PMID]
10. de Sá MFS. Premature ovarian insufficiency and bone health care: A concern of the gynecologist. Rev Bras Ginecol Obstet 2018; 40: 305-308. [DOI:10.1055/s-0038-1667112] [PMID]
11. Dunneram Y, Greenwood DC, Cade JE. Diet, menopause and the risk of ovarian, endometrial and breast cancer. Proc Nutr Soc 2019; 78: 438-448. [DOI:10.1017/S0029665118002884] [PMID]
12. La Vecchia C. Ovarian cancer: Epidemiology and risk factors. Eur J Cancer Prev 2017; 26: 55-62. [DOI:10.1097/CEJ.0000000000000217] [PMID]
13. Roett MA. Genital cancers in women: Uterine cancer. FP Essent 2015; 438: 11-17.
14. Hansen J. Environmental noise and breast cancer risk? Scand J Work Environ Health 2017; 43: 505-508. [DOI:10.5271/sjweh.3681] [PMID]
15. Dall GV, Britt KL. Estrogen effects on the mammary gland in early and late life and breast cancer risk. Front Oncol 2017; 7: 110. [DOI:10.3389/fonc.2017.00110] [PMID] [PMCID]
16. Anderson CJ, Verkuilen J, Johnson T. Applied generalized linear mixed models: Continuous and discrete data. New York: Springer; 2012.
17. McCullagh P, Nelder JA. Generalized linear models. 2nd Ed. New York: Routledge; 2019. [DOI:10.1201/9780203753736]
18. Moran JL, Solomon PJ, Peisach AR, Martin J. New models for old questions: Generalized linear models for cost prediction. J Eval Clin Pract 2007; 13: 381-389. [DOI:10.1111/j.1365-2753.2006.00711.x] [PMID]
19. Agresti A. Foundations of linear and generalized linear models. New York: John Wiley & Sons; 2015.
20. Eghtesad S, Mohammadi Z, Shayanrad A, Faramarzi E, Joukar F, Hamzeh B, et al. The Persian cohort: Providing the evidence needed for healthcare reform. Arch Iran Med 2017; 20: 691-695.
21. Salmerón R, García CB, García J. Variance inflation factor and condition number in multiple linear regression. J Stat Comput Simulat 2018; 88: 2365-2384. [DOI:10.1080/00949655.2018.1463376]
22. Delignette-Muller ML, Dutang Ch. Fitdistrplus: An R package for fitting distributions. J Statist Software 2015; 64: 1-34. [DOI:10.18637/jss.v064.i04]
23. Chai T, Draxler RR. Root mean square error (RMSE) or mean absolute error (MAE)? Arguments against avoiding RMSE in the literature. Geosci Model Dev 2014; 7: 1247-1250. [DOI:10.5194/gmd-7-1247-2014]
24. Willmott CJ, Matsuura K. Advantages of the mean absolute error (MAE) over the root mean square error (RMSE) in assessing average model performance. Climate Res 2005; 30: 79-82. [DOI:10.3354/cr030079]
25. Fallahzadeh H. Age at natural menopause in Yazd, Islamic Republic of Iran. Menopause 2007; 14: 900-904. [DOI:10.1097/gme.0b013e318032b2e6] [PMID]
26. Saei Ghare Naz M, Sayehmiri F, Kiani F, Ozgoli G. A systematic review and meta-analysis on the average age of menopause among iranian women. Evidence Based Care J 2019; 8: 26-34.
27. Wang M, Gong WW, Hu RY, Wang H, Guo Y, Bian Z, et al. Age at natural menopause and associated factors in adult women: Findings from the China Kadoorie Biobank study in Zhejiang rural area. PloS One 2018; 13: e0195658. [DOI:10.1371/journal.pone.0195658] [PMID] [PMCID]
28. Zhu D, Chung HF, Pandeya N, Dobson AJ, Kuh D, Crawford SL, et al. Body mass index and age at natural menopause: An international pooled analysis of 11 prospective studies. Eur J Epidemiol 2018; 33: 699-710. [DOI:10.1007/s10654-018-0367-y] [PMID]
29. Tao X, Jiang A, Yin L, Li Y, Tao F, Hu H. Body mass index and age at natural menopause: A meta-analysis. Menopause 2015; 22: 469-474. [DOI:10.1097/GME.0000000000000324] [PMID]
30. Whitcomb BW, Purdue-Smithe AC, Szegda KL, Boutot ME, Hankinson SE, Manson JE, et al. Cigarette smoking and risk of early natural menopause. Am J Epidemiol 2018; 187: 696-704. [DOI:10.1093/aje/kwx292] [PMID] [PMCID]
31. Yang HJ, Suh PS, Kim SJ, Lee SY. Effects of smoking on menopausal age: Results from the Korea national health and nutrition examination survey, 2007 to 2012. J Prev Med Public Health 2015; 48: 216-224. [DOI:10.3961/jpmph.15.021] [PMID] [PMCID]
32. Morris DH, Jones ME, Schoemaker MJ, McFadden E, Ashworth A, Swerdlow AJ. Body mass index, exercise, and other lifestyle factors in relation to age at natural menopause: Analyses from the breakthrough generations study. Am J Epidemiol 2012; 175: 998-1005. [DOI:10.1093/aje/kwr447] [PMID]
33. Omidi A, Bakht R, Moghimbeigi A, Balali Z. A study of age at menopause and related factors. Life Sci J 2013; 10: 1295-1299.
34. Santoro N. Perimenopause: From research to practice. J Womens Health 2016; 25: 332-339. [DOI:10.1089/jwh.2015.5556] [PMID] [PMCID]
35. Sasi Sekhar TVD, Medarametla S, Rahman A, Adapa SS. Early menopause in type 2 diabetes: A study from a south Indian tertiary care centre. J Clin Diagn Res 2015; 9: OC08-OC10. [DOI:10.7860/JCDR/2015/14181.6628] [PMID] [PMCID]
36. Monterrosa-Castro A, Blümel J, Portela-Buelvas K, Mezones-Holguín E, Barón G, Bencosme A, et al. Type II diabetes mellitus and menopause: A multinational study. Climacteric 2013; 16: 663-672. [DOI:10.3109/13697137.2013.798272] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
