
International Journal of
Reproductive Biomedicine
Sun, Jun 14, 2026
[Archive]
Volume 20, Issue 1 (January 2022)
IJRM 2022, 20(1): 59-64 |
Back to browse issues page




![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mehdizadeh A, Chaichian S, Mirgaloybayat S, Rokhgireh S, Tahermanesh K, Kadivar M et al . Right-side inguinal canal endometriosis at ultrasound: A case report. IJRM 2022; 20 (1) :59-64
URL: http://ijrm.ir/article-1-2213-en.html
URL: http://ijrm.ir/article-1-2213-en.html
Abolfazl Mehdizadeh1 

 , Shahla Chaichian2 , Shahla Mirgaloybayat1 , Samaneh Rokhgireh1 , Kobra Tahermanesh1 , Maryam Kadivar3 , Farahnaz Farzaneh *4
, Shahla Chaichian2 , Shahla Mirgaloybayat1 , Samaneh Rokhgireh1 , Kobra Tahermanesh1 , Maryam Kadivar3 , Farahnaz Farzaneh *4
, Shahla Chaichian2 , Shahla Mirgaloybayat1 , Samaneh Rokhgireh1 , Kobra Tahermanesh1 , Maryam Kadivar3 , Farahnaz Farzaneh *4
1- Endometriosis Research Center, Iran University of Medical Sciences, Tehran, Iran.
2- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Tehran, Iran.
3- Department of Pathology, Hazrat-e-Rasool Akram General Hospital, Iran University of Medical Sciences, Tehran, Iran.
4- Endometriosis Research Center, Iran University of Medical Sciences, Tehran, Iran. ,Farahnaz1826@yahoo.com
2- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Tehran, Iran.
3- Department of Pathology, Hazrat-e-Rasool Akram General Hospital, Iran University of Medical Sciences, Tehran, Iran.
4- Endometriosis Research Center, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 1635 kb]
(1794 Downloads)
| Abstract (HTML) (2679 Views)
1. Introduction
Endometriosis was first described by Rokitansky in 1860 and it is a common gynecological disease. Endometriosis is characterized by proliferation of functioning endometrial glands and stroma (endometrium) outside the uterine cavity (pelvis or extra pelvic) (1-4).
The prevalence of endometriosis in women of reproductive age is 10-20%, with occurrence mainly in the pelvic peritoneum, pouch of Douglas, fallopian tubes and ovaries. There are many case reports of endometriosis in almost every organ except the spleen. Extra pelvic endometriosis is rare and refers to implants found in the urinary tract and lungs, gastrointestinal tract, bone, episiotomy scars and rarer places such as the umbilicus, surgical scars, inguinal canal, extremities, skin and central nervous system (5-7).
Inguinal endometriosis is rare and often overlooked or misdiagnosed. The most common symptoms are a change of inguinal mass size and inguinal pain during the menstrual cycle (8).
Differential diagnosis of a suspected inguinal mass is important and the causes of inguinal masses include hernia, neuroma, abscess, hydroceles, lymphadenopathy, lymphoma, lipoma and cancer (9).
2. Case presentation
A 39-yr-old virgin female gynecologist presented at Hazrat-e Rasoul Hospital, (Tehran, Iran) in December 2020 with a localized pain in the right inguinal area. The pain had started four yr previously and at this point was very tender, especially during the first to fifth days of her menstrual cycle. The participant had no specific medical or abdominal surgery history. She did not have any family history of endometriosis or hernia; she had regular menstruation at 26-day intervals without any abnormal uterine bleeding. Her menstruation period was 3-4 days. Physical examination four yr previously showed a tender mass measuring approximately 1×1 cm located on the right, superior to the pubic tubercle. The size of the mass was larger after four yr (3×1 cm). The position of the mass remained unchanged and was not related to cough or force.
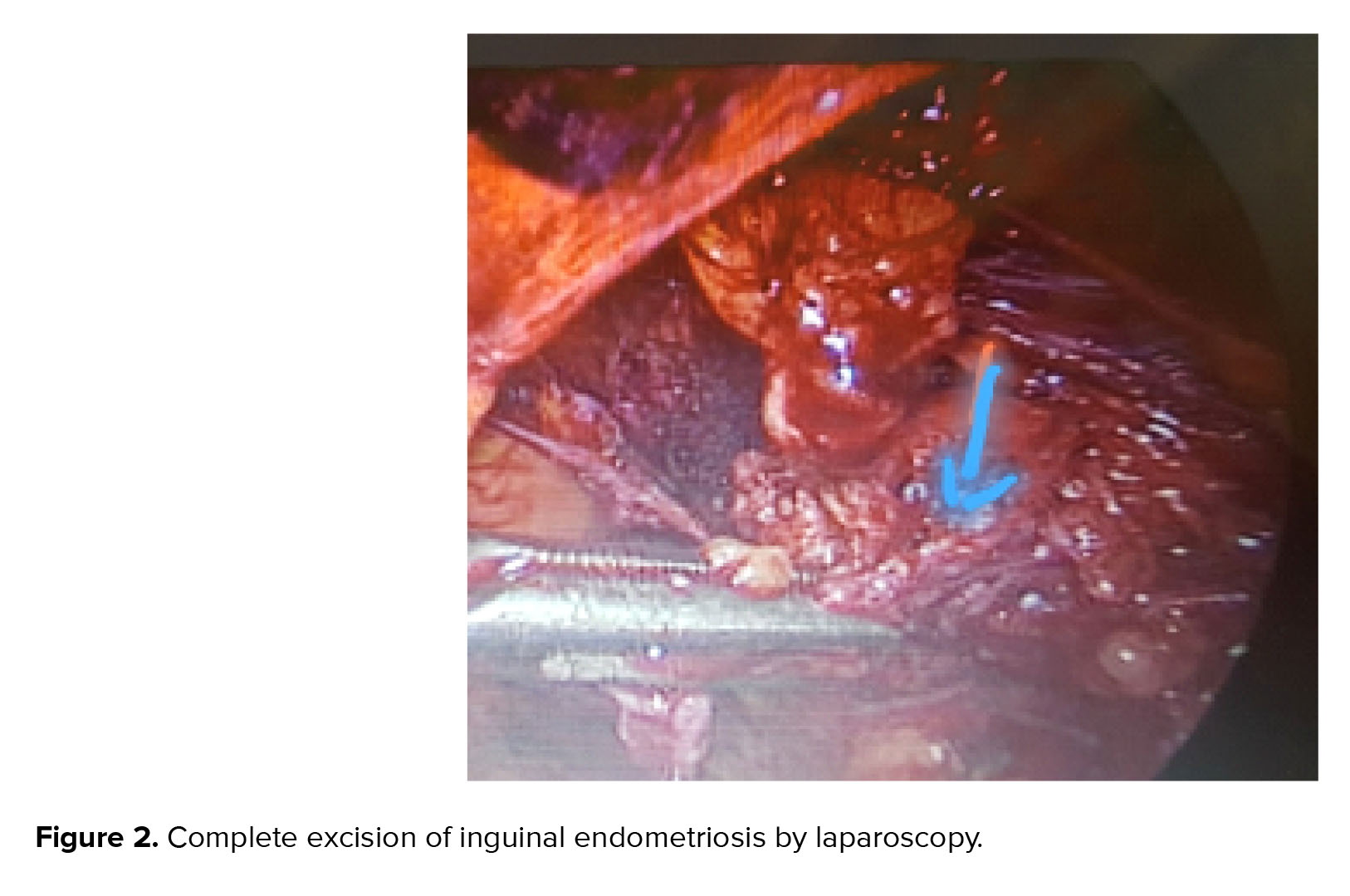
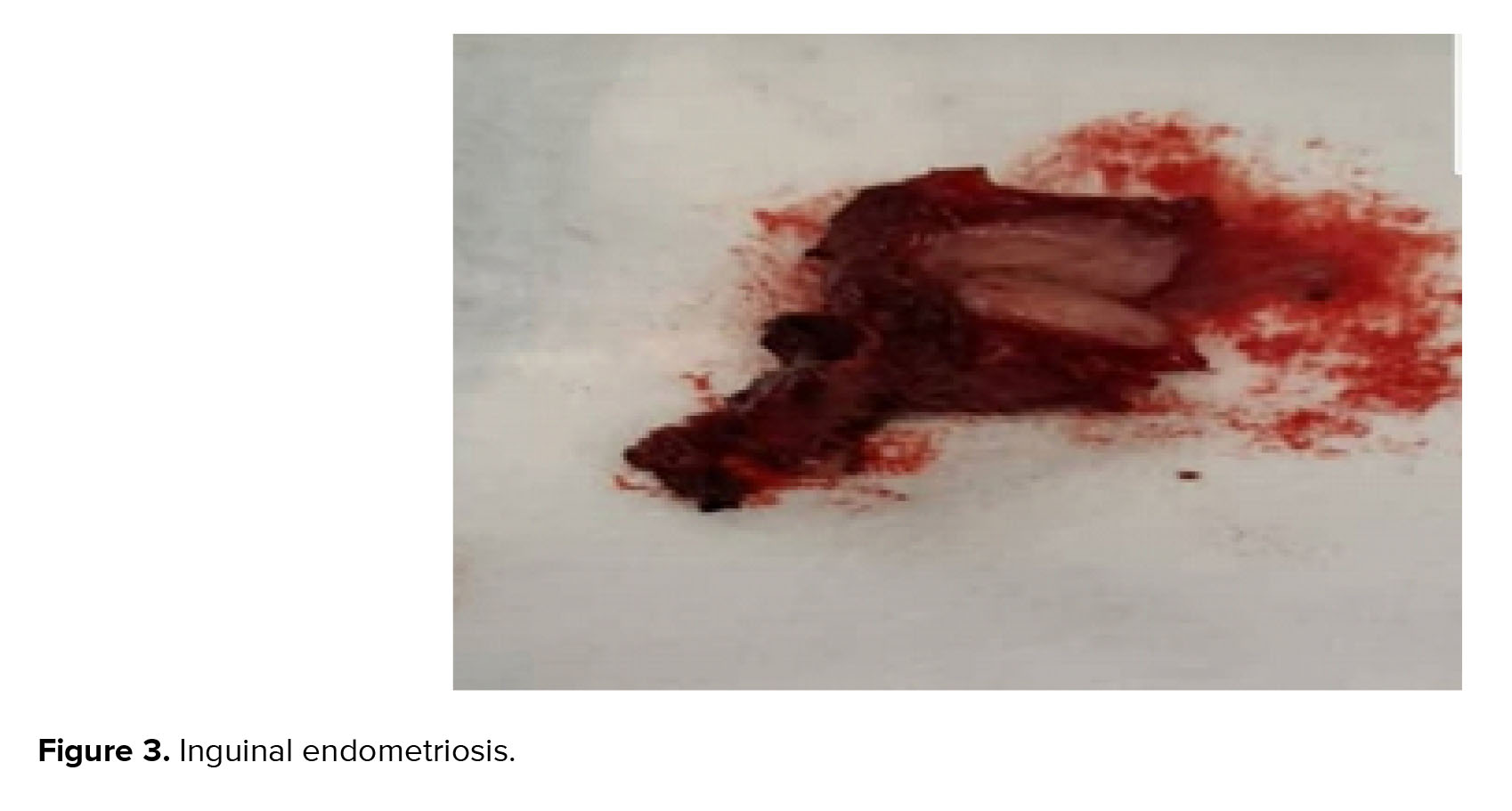
An ultrasound had been performed four yr before in Tabriz, Azerbaijan, which showed a small inguinal hernia on the right. After four yr, a transabdominal ultrasound was repeated by two expert radiologists and they reported a uterus volume of 36×42×73 mm3 with a normal myometrium; endometrial thickness of 3 mm; and a right ovary of 7 cc and left ovary of 5 cc. The two adnexa were normal. According to an ultrasound of the inguinal canal, there was one hypoechogenic mass with a size of 30×14 mm in the right inguinal; a color Doppler showed minimal vascularity and so an inguinal hernia was ruled out (Figure 1). The following tumor markers were measured: cancer antigen 125: 33.3 u/ml, cancer antigen 19-9 (: 12.3 u/ml, and human epididymis protein 4: 63.9 u/ml. The risk of ovarian malignancy algorithm index was 13.2. Transvaginal ultrasonography was not performed because of her virginity. After providing informed consent, the participant opted for surgical excision of the inguinal mass by laparoscopy (Figures 2-3). The inguinal mass was excised by an expert laparoscopist and the diagnosis of endometriosis was established through the final pathology after surgery. The participant was well and has not had any pain during her menstrual cycle since the surgery. The most important reason for reporting this case was that the individual did not have a history of abdominal surgery and was misdiagnosed for four yr (Figure 4).
2.1. Ethical considerations
Written consent was obtained from the participant for reporting the case.


3. Discussion
Endometriosis has been shown to be estrogen-dependent but its etiology is multifactorial (1, 2). Retrograde menstruation explained the theory that endometrial cells protrude from the end of the fallopian tubes and the menstrual blood remains on the peritoneal surfaces of the pelvis and abdomen.
Inguinal endometriosis is an uncommon problem that occurs in 0.6% of women (4). Women with inguinal endometriosis have mild to severe dysmenorrhea and a mass in this area (2, 4).
Overall, all the proposed hypotheses for the cell origin can be categorized into two main theories: the in-situ theory and the transplantation theory However, the exact origin and mechanism of endometriosis development remain theoretical (4, 5). The growing body of evidence confirms the multifactorial nature of endometriosis that is the result of the combined contribution of anatomical, hormonal, immunological, reactive, estrogenic, genetic, epigenetic, and environmental factors in affected women (8, 10), and two different theories were showed 1) the sigmoid colon support the left inguinal canal, and 2) endometrial cells remain on the right side because of the clockwise movement of intraperitoneal fluid (10), our case had right inguinal endometriosis also. Differential diagnosis (DD) is necessary in cases of suspected inguinal mass (9). Abdominal sonography, trans vaginal sonography, trans rectal sonography, magnetic resonance imaging (MRI), Computed tomography (CT), are useful diagnostic instruments. However, if the ultrasound is performed by expert radiologist, it will be valuable. The appearance of inguinal endometriosis in CT is often not specific (9), it appears as solid, cystic or complex. MRI is more accurate than CT. Two MRI patterns are showed for inguinal endometriosis. Type I pattern includes cystic hyper-intense lesions and type 2 lesions with solid components (10). Ultrasound findings of inguinal endometriosis are variable, cystic masses, represent intra-cystic bleeding with menstruation, and are found in most cases which in our participant is an oval lesion. Differential diagnosis in. cystic inguinal masses include inguinal hernia and hydrocele, and solid masses is sarcoma, lymphoma, hematoma, and abscess. In inguinal endometriosis, differential diagnosis based on imaging results should be accompanied by a history of dysmenorrhea because of not being of specific diagnostic modality. Needle aspiration cytology provides accurate provides diagnosis before removal of malignancy and could be useful in selected cases (9). Women with inguinal endometriosis usually have a history of previous surgery. If inguinal endometriosis is correctly diagnosed before the operation, the woman can undergo laparoscopic surgery to remove the pathology of inguinal point as ultrasound was done for our participant and inguinal endometriosis was reported and she was performed laparoscopy surgery. The participant of our study had no problems except the brief pain at the site of the trocars, and was discharged in well general condition the day after the operation. The pathologic diagnosis was inguinal endometriosis. Therefore, attention to inguinal endometriosis in women with inguinal mass is important even if there is no history of gynecological or abdominal surgery. Treatment of inguinal endometriosis is surgical removal of the mass (10).
4. Conclusion
Considering of inguinal endometriosis in the differential diagnosis of women with inguinal mass is important, even if there is not history of gynecologic or abdominal surgery.
Acknowledgements
The authors wish to thank the participant who allowed us to report the process of her surgery and declare that the current research has been done without supports from Iran University of Medical Science.
Conflict of Interest
The authors declare no conflict of interest.
Full-Text: (702 Views)
1. Introduction
Endometriosis was first described by Rokitansky in 1860 and it is a common gynecological disease. Endometriosis is characterized by proliferation of functioning endometrial glands and stroma (endometrium) outside the uterine cavity (pelvis or extra pelvic) (1-4).
The prevalence of endometriosis in women of reproductive age is 10-20%, with occurrence mainly in the pelvic peritoneum, pouch of Douglas, fallopian tubes and ovaries. There are many case reports of endometriosis in almost every organ except the spleen. Extra pelvic endometriosis is rare and refers to implants found in the urinary tract and lungs, gastrointestinal tract, bone, episiotomy scars and rarer places such as the umbilicus, surgical scars, inguinal canal, extremities, skin and central nervous system (5-7).
Inguinal endometriosis is rare and often overlooked or misdiagnosed. The most common symptoms are a change of inguinal mass size and inguinal pain during the menstrual cycle (8).
Differential diagnosis of a suspected inguinal mass is important and the causes of inguinal masses include hernia, neuroma, abscess, hydroceles, lymphadenopathy, lymphoma, lipoma and cancer (9).
2. Case presentation
A 39-yr-old virgin female gynecologist presented at Hazrat-e Rasoul Hospital, (Tehran, Iran) in December 2020 with a localized pain in the right inguinal area. The pain had started four yr previously and at this point was very tender, especially during the first to fifth days of her menstrual cycle. The participant had no specific medical or abdominal surgery history. She did not have any family history of endometriosis or hernia; she had regular menstruation at 26-day intervals without any abnormal uterine bleeding. Her menstruation period was 3-4 days. Physical examination four yr previously showed a tender mass measuring approximately 1×1 cm located on the right, superior to the pubic tubercle. The size of the mass was larger after four yr (3×1 cm). The position of the mass remained unchanged and was not related to cough or force.
An ultrasound had been performed four yr before in Tabriz, Azerbaijan, which showed a small inguinal hernia on the right. After four yr, a transabdominal ultrasound was repeated by two expert radiologists and they reported a uterus volume of 36×42×73 mm3 with a normal myometrium; endometrial thickness of 3 mm; and a right ovary of 7 cc and left ovary of 5 cc. The two adnexa were normal. According to an ultrasound of the inguinal canal, there was one hypoechogenic mass with a size of 30×14 mm in the right inguinal; a color Doppler showed minimal vascularity and so an inguinal hernia was ruled out (Figure 1). The following tumor markers were measured: cancer antigen 125: 33.3 u/ml, cancer antigen 19-9 (: 12.3 u/ml, and human epididymis protein 4: 63.9 u/ml. The risk of ovarian malignancy algorithm index was 13.2. Transvaginal ultrasonography was not performed because of her virginity. After providing informed consent, the participant opted for surgical excision of the inguinal mass by laparoscopy (Figures 2-3). The inguinal mass was excised by an expert laparoscopist and the diagnosis of endometriosis was established through the final pathology after surgery. The participant was well and has not had any pain during her menstrual cycle since the surgery. The most important reason for reporting this case was that the individual did not have a history of abdominal surgery and was misdiagnosed for four yr (Figure 4).
2.1. Ethical considerations
Written consent was obtained from the participant for reporting the case.
3. Discussion
Endometriosis has been shown to be estrogen-dependent but its etiology is multifactorial (1, 2). Retrograde menstruation explained the theory that endometrial cells protrude from the end of the fallopian tubes and the menstrual blood remains on the peritoneal surfaces of the pelvis and abdomen.
Inguinal endometriosis is an uncommon problem that occurs in 0.6% of women (4). Women with inguinal endometriosis have mild to severe dysmenorrhea and a mass in this area (2, 4).
Overall, all the proposed hypotheses for the cell origin can be categorized into two main theories: the in-situ theory and the transplantation theory However, the exact origin and mechanism of endometriosis development remain theoretical (4, 5). The growing body of evidence confirms the multifactorial nature of endometriosis that is the result of the combined contribution of anatomical, hormonal, immunological, reactive, estrogenic, genetic, epigenetic, and environmental factors in affected women (8, 10), and two different theories were showed 1) the sigmoid colon support the left inguinal canal, and 2) endometrial cells remain on the right side because of the clockwise movement of intraperitoneal fluid (10), our case had right inguinal endometriosis also. Differential diagnosis (DD) is necessary in cases of suspected inguinal mass (9). Abdominal sonography, trans vaginal sonography, trans rectal sonography, magnetic resonance imaging (MRI), Computed tomography (CT), are useful diagnostic instruments. However, if the ultrasound is performed by expert radiologist, it will be valuable. The appearance of inguinal endometriosis in CT is often not specific (9), it appears as solid, cystic or complex. MRI is more accurate than CT. Two MRI patterns are showed for inguinal endometriosis. Type I pattern includes cystic hyper-intense lesions and type 2 lesions with solid components (10). Ultrasound findings of inguinal endometriosis are variable, cystic masses, represent intra-cystic bleeding with menstruation, and are found in most cases which in our participant is an oval lesion. Differential diagnosis in. cystic inguinal masses include inguinal hernia and hydrocele, and solid masses is sarcoma, lymphoma, hematoma, and abscess. In inguinal endometriosis, differential diagnosis based on imaging results should be accompanied by a history of dysmenorrhea because of not being of specific diagnostic modality. Needle aspiration cytology provides accurate provides diagnosis before removal of malignancy and could be useful in selected cases (9). Women with inguinal endometriosis usually have a history of previous surgery. If inguinal endometriosis is correctly diagnosed before the operation, the woman can undergo laparoscopic surgery to remove the pathology of inguinal point as ultrasound was done for our participant and inguinal endometriosis was reported and she was performed laparoscopy surgery. The participant of our study had no problems except the brief pain at the site of the trocars, and was discharged in well general condition the day after the operation. The pathologic diagnosis was inguinal endometriosis. Therefore, attention to inguinal endometriosis in women with inguinal mass is important even if there is no history of gynecological or abdominal surgery. Treatment of inguinal endometriosis is surgical removal of the mass (10).
4. Conclusion
Considering of inguinal endometriosis in the differential diagnosis of women with inguinal mass is important, even if there is not history of gynecologic or abdominal surgery.
Acknowledgements
The authors wish to thank the participant who allowed us to report the process of her surgery and declare that the current research has been done without supports from Iran University of Medical Science.
Conflict of Interest
The authors declare no conflict of interest.
Type of Study: Case Report |
Subject:
Reproductive Surgery
References
1. Arakawa T, Hirata T, Koga K, Neriishi K, Fukuda Sh, Ma S, et al. Clinical aspects and management of inguinal endometriosis: A case series of 20 patients. J Obstet Gynaecol Res 2019; 45: 2029-2036. [DOI:10.1111/jog.14059] [PMID]
2. Niitsu H, Tsumura H, Kanehiro T, Yamaoka H, Taogoshi H, Murao N. Clinical characteristics and surgical treatment for inguinal endometriosis in young women of reproductive age. Dig Surg 2019; 36: 166-172. [DOI:10.1159/000489827] [PMID]
3. Wolfhagen N, Simons NE, de Jong KH, van Kesteren PJM, Simons MP. Inguinal endometriosis, a rare entity of which surgeons should be aware: Clinical aspects and long-term follow-up of nine cases. Hernia 2018; 22: 881-886. [DOI:10.1007/s10029-018-1797-x] [PMID]
4. Fujikawa H, Uehara Y. Inguinal endometriosis: An unusual cause of groin pain. Balkan Med J 2020; 37: 291-292. [DOI:10.4274/balkanmedj.galenos.2020.2020.2.105] [PMID] [PMCID]
5. Andres MP, Arcoverde FVL, Souza CCC, Fernandes LFC, Simões Abrão M, Kho RM. Extrapelvic endometriosis: A systematic review. J Minim Invasive Gynecol 2020; 27: 373-389. [DOI:10.1016/j.jmig.2019.10.004] [PMID]
6. Nagama T, Kakudo N, Fukui M, Yamauchi T, Mitsui T, Kusumoto K. Heterotopic endometriosis in the inguinal region: A case report and literature review. Eplasty 2019; 19: ic19.
7. HerniaSurge Group. International guidelines for groin hernia management. Hernia 2018; 22: 1-165. [DOI:10.1007/s10029-017-1668-x] [PMID] [PMCID]
8. Lim MCh, Choi JY, Lee DO, Yoo JW, Park SY, Seo SS. Inguinal endometriosis connected to intraperitoneal round ligament: Complete excision with extraperitoneal wide dissection. Korean J Obstet Gynecol 2008; 51: 1533-1538.
9. Behnoud N, Rezaei R, Esform E, Farzaneh F. The relationship between endometrial thickness and endometrial pattern with pregnancy rate based on positive serum beta-human chorionic gonadotropin. International Journal of Women's Health and Reproduction Sciences 2019; 7: 400-403. [DOI:10.15296/ijwhr.2019.65]
10. Sun ZhJ, Zhu L, Lang JH. A rare extrapelvic endometriosis: Inguinal endometriosis. J Reprod Med 2010; 55: 62-66.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
