
International Journal of
Reproductive Biomedicine
Tue, Jun 23, 2026
[Archive]
Volume 24, Issue 4 (April 2026)
IJRM 2026, 24(4): 297-314 |
Back to browse issues page


Ethics code: IR.SSU.RSI.REC.1401.018
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Farajkhoda T, Mohammadkhani S, Sarebanhassanabadi M, Javaheri A, ZareMobini F. Design and implementation of interventions to improve sexual health of women with endometriosis: A mixed-methods study protocol with an interventional design. IJRM 2026; 24 (4) :297-314
URL: http://ijrm.ir/article-1-3551-en.html
URL: http://ijrm.ir/article-1-3551-en.html
Tahmineh Farajkhoda1 

 , Shahla Mohammadkhani2 , Mohammadtaghi Sarebanhassanabadi3 , Atiyeh Javaheri4 , Fatemeh ZareMobini *5
, Shahla Mohammadkhani2 , Mohammadtaghi Sarebanhassanabadi3 , Atiyeh Javaheri4 , Fatemeh ZareMobini *5
, Shahla Mohammadkhani2 , Mohammadtaghi Sarebanhassanabadi3 , Atiyeh Javaheri4 , Fatemeh ZareMobini *5
1- Research Center for Nursing and Midwifery Care, Comprehensive Research Institute for Maternal and Child Health, Department of Midwifery, School of Nursing and Midwifery, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2- Student Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Yazd Cardiovascular Research Center, Non-Communicable Diseases Research Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Department of Obstetrics and Gynecology, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Research Center for Nursing and Midwifery Care, Comprehensive Research Institute for Maternal and Child Health, Department of Midwifery, School of Nursing and Midwifery, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,f.zaremobini@ssu.ac.ir
2- Student Research Center, Faculty of Nursing and Midwifery, Isfahan University of Medical Sciences, Isfahan, Iran.
3- Yazd Cardiovascular Research Center, Non-Communicable Diseases Research Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
4- Department of Obstetrics and Gynecology, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5- Research Center for Nursing and Midwifery Care, Comprehensive Research Institute for Maternal and Child Health, Department of Midwifery, School of Nursing and Midwifery, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,
Full-Text [PDF 444 kb]
(139 Downloads)
| Abstract (HTML) (183 Views)
2.2.1.5. Analysis
Qualitative content analysis will be used as the conventional approach for analyzing qualitative phase data. Conventional content analysis in this research will be done according to the steps suggested by Graneheim and Lundman (24), this method has the following 5 steps:
2.2.2. Phase 2: literature review
2.2.2.1. Databases
In this phase, we will conduct a systematic review of the existing literature to determine evidence-based approaches for enhancing the sexual health of women living with endometriosis. The review process will follow the PRISMA guidelines for both conduct and reporting. To identify relevant studies, comprehensive searches will be carried out in the PubMed/MEDLINE, Scopus, and Web of Science electronic databases.
2.2.2.2. Search strategy
A comprehensive search strategy has been developed with an experienced researcher. The search combines terms related to the condition (endometriosis), outcomes/areas of interest (sexual health, sexual function, sexual quality of life, dyspareunia, sexual dysfunction, interventions, strategies, management), using controlled vocabulary (MeSH terms in PubMed) where applicable, and free-text terms.
Main keywords and synonyms (in English; Persian equivalents will be used if searching Persian databases, though currently focused on international databases):
2.2.2.5. Study selection and quality assessment
2 reviewers will independently screen the titles and abstracts of identified records based on pre-established inclusion criteria. Any studies considered potentially relevant will have their full texts obtained and evaluated separately by the same reviewers. If any disagreements arise, they will be addressed through discussion, and if necessary, by involving a third reviewer.
The evaluation of study quality and risk of bias will be adapted according to the specific study design:
2.2.4.2. Sample size
Sample size was calculated using G*Power software. We assumed a small-to-moderate effect size of Cohen's d = 0.35 for the primary outcome (total FSFI score change), based on previous intervention studies in women with endometriosis or chronic pelvic pain showing standardized mean differences in sexual function outcomes ranging from 0.3-0.6 after psycho-educational or multidisciplinary interventions. Parameters: α = 0.05, power (1-β) = 0.90, correlation among repeated measures = 0.5, no sphericity correction ε = 0.75. This yields approximately 28-30 participants per group (total n ≈ 56-60). Anticipating an attrition rate of up to 20% (based on dropout rates of 15-30% reported in similar RCTs of behavioral/educational interventions in women with endometriosis and chronic pelvic pain), we inflate the sample to 35-38 per group (total n = 70-76). The final target sample size is 70 women (35 per group) to ensure adequate power even with moderate attrition.
2.2.4.3. Randomization and allocation concealment
Eligible participants will be randomly allocated to either the intervention group or the control group in a 1:1 ratio. The randomization sequence will be generated using computer software by an independent statistician who is not involved in the participant recruitment process or in the assessment of study outcomes.
Randomization will be performed in permuted blocks of size 4 or 6 (randomly varying block sizes to prevent prediction) to balance potential prognostic factors. Allocation concealment will be maintained through the use of sequentially numbered, opaque, sealed envelopes, which will be prepared in advance by the independent statistician. Envelopes will be opened only after baseline assessment and informed consent, by a researcher not involved in data collection. Blinding: due to the nature of behavioral/educational intervention, participants and intervention deliverers cannot be blinded. Data analysts will also be blinded during primary analysis (group codes will be concealed until analysis completion).
The control group will receive routine care (standard gynecological follow-up and management in the study setting).
2.2.4.4. Eligibility criteria
Inclusion criteria:
2.2.4.5. Scales and data collection Instruments
The instruments for collecting data will be the personal-social information questionnaire and the FSFI, and the SQOL. Study questionnaires are completed by the participants before the intervention, immediately and 2 months after the intervention.
2.2.4.5.1. Personal–social information form
The personal-social information form will include details such as age, family economic status, education level of the participant, employment status, and other relevant information. This form will be completed upon the participants’ entry into the study.
2.2.4.5.2. FSFI
FSFI, is a self‑reported instrument consisting of 19 items that evaluate women’s sexual function during the previous 4 wk. The questionnaire measures 6 domains: sexual desire (2 items), arousal (4 items), lubrication (4 items), orgasm (3 items), satisfaction (3 items), and pain (3 items). Items are rated on a 5‑point Likert scale; while most items are scored from 1-5, some include a score of 0 to indicate no sexual activity. Domain scores are obtained by summing the relevant items and multiplying the result by a specific domain factor (0.6 for desire; 0.3 for arousal and lubrication; and 0.4 for orgasm, satisfaction, and pain), resulting in domain scores ranging from 0-6 (with the desire domain ranging from 1.2-6). The overall FSFI score ranges from 2-36, with higher scores reflecting better sexual function. The Persian version of this questionnaire has also been validated (26).
2.2.4.5.3. SQOL-female
The SQOL questionnaire was designed and developed to measure the sexual quality of life. An 18-item self-report measure assessing the impact of sexual function on quality of life. Items are scored on a 6-point Likert scale (1 = completely agree to 6 = completely disagree, with reverse scoring for positively worded items). Total score ranges from 18-108, with higher scores indicating better sexual quality of life. Maasoumi and Montazeri in 2013 confirmed the validity and reliability of the Farsi version of this questionnaire for the first time in Iran (27).
2.3. Ethical Considerations
Ethical approval for this protocol study has been obtained from the research ethics committees of Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.RSI.REC.1401.018). Registration of a randomized controlled clinical trial has been accomplished with the Iranian Registry of Clinical Trials (IRCT20220620055229N2).
2.4. Statistical Analysis
The primary analysis will be conducted on an intention-to-treat basis, including all randomized participants in their assigned group regardless of protocol adherence or dropout. A secondary per‑protocol analysis will be performed for sensitivity, including only participants who completed at least 80% of the intervention sessions and provided outcome data at all time points. For continuous outcomes (FSFI total/domain scores, SQOL total score), we will use linear mixed-effects models (repeated measures) with time, group, and time × group interaction as fixed effects, participant as random effect, and adjustment for baseline score and stratification variables (age group). This approach handles missing data under the missing-at-random assumption and is superior to last-observation-carried-forward. If substantial missingness occurs (> 15-20%), multiple imputations (e.g., 20-30 imputations) by chained equations will be used as a sensitivity analysis. Categorical outcomes (e.g., proportion achieving clinically meaningful improvement in FSFI ≥ 4 points) will be analyzed using Chi-square or logistic regression. Effect sizes (Cohen's d or partial eta-squared) will be reported. Statistical significance will be set at p < 0.05 (2-tailed). Analyses will be performed using SPSS version 25.
3. Discussion
Several studies have highlighted the profound negative impact of endometriosis on women's sexual health, including high rates of dyspareunia, reduced sexual desire, arousal difficulties, orgasmic dysfunction, and overall diminished sexual quality of life (9-11, 13, 16, 23). Despite these well-documented challenges, sexual health concerns are frequently overlooked in routine clinical care, and existing interventions often remain limited to pain management (surgical or pharmacological), with only partial success in alleviating sexual symptoms (13, 19-21, 23). Psycho-sexual and educational approaches show promise but lack comprehensive, culturally tailored programs, particularly in contexts like Iran, where socio-cultural factors, stigma around sexual discussions, and limited access to specialized sexual health services may further compound the burden (17, 18, 28, 29).
This mixed-methods study protocol addresses these gaps by systematically developing and evaluating a targeted, evidence-based intervention program. The sequential design integrates qualitative insights from affected women and healthcare providers (phase 1), evidence from a systematic review (phase 2), expert prioritization via Delphi (phase 3), and rigorous RCT evaluation (phase 4). This approach is expected to yield a holistic, contextually relevant program that goes beyond symptom relief to address emotional, relational, and socio-cultural dimensions of sexual health.
Potential contributions and expected impact, if effective, the developed intervention could offer several important contributions: provide the first comprehensive, culturally adapted sexual health promotion program specifically for Iranian women with endometriosis, filling a critical gap in localized, patient-centered care. Demonstrate the feasibility and preliminary effectiveness of a multidisciplinary, non-pharmacological approach combining education, counseling, self-management strategies, and relational support. Generate evidence to inform clinical guidelines, midwifery and gynecology practice, and policy-making regarding integration of sexual health assessment and intervention into routine endometriosis management. Contribute to broader reproductive health literature by illustrating the value of mixed-methods sequential designs in developing complex behavioral interventions for chronic gynecological conditions.
Foreseeable limitations and mitigation strategies as with any prospective interventional study, several limitations and challenges can be anticipated:
Full-Text: (18 Views)
1. Introduction
Endometriosis is a hormone-dependent chronic inflammatory disease affecting approximately 10% of women of reproductive age worldwide, making it the most common cause of chronic pelvic pain (1-4). This condition is associated with symptoms such as dyspareunia, dysmenorrhea, and dyschezia, which can lead to sexual dysfunction and negatively impact the quality of couples' sexual life and satisfaction (5-7). Studies indicate that 47-75% of women with endometriosis experience sexual dysfunction, including desire disorders, arousal issues, orgasm disorders, and deep dyspareunia, which disrupts the sexual response cycle (8-11). These sexual problems extend beyond physical pain, affecting mental activation, marital relationships, fertility, and overall well-being, encompassing psychological issues, reduced quality of life, and social challenges (12-18). Undertaking this study is essential because endometriosis profoundly affects all aspects of women's lives, yet sexual health is frequently overlooked in medical visits despite its critical role in fertility and relational stability (17, 18). Untreated sexual dysfunction can exacerbate isolation, depression, and partnership breakdowns, underscoring the need for targeted interventions to enhance sexual health and quality of life.
Previous studies have documented the multifaceted impacts of endometriosis on sexual function, highlighting strong associations with pain and reduced satisfaction, and have proposed various interventions (9-11, 16). Common treatments include surgical procedures to excise lesions and alleviate pain (19, 20), pharmacological options such as sedatives and progestins (21), couples therapy (22), use of vaginal lubricants, sexual counseling, and positional adjustments (16). However, these approaches have limitations: surgery and progesterone therapy reduce sexual pain in only 43-59% of cases, while hormonal treatments often cause vaginal dryness and exacerbate dyspareunia (13, 23). Psycho-sexual interventions remain limited, although emerging evidence suggests that, if expanded, they could effectively mitigate pain and related consequences; nevertheless, further research is required to confirm their efficacy in endometriosis patients (13).
Existing research predominantly relies on quantitative methods, inadequately exploring culture- and context-specific needs and overlooking qualitative insights from patients and service providers. This creates a knowledge gap: current interventions lack personalization, fail to address holistic sexual health strategies, and do not account for diverse socio-cultural factors, leaving many women with persistent, underserved sexual challenges. This study adds value by addressing this knowledge gap through a comprehensive, evidence-based program tailored to the unique needs of women with endometriosis. By conducting a qualitative exploration of perspectives from affected women and service providers, combined with a review of available resources, we develop targeted strategies that extend beyond symptom management to holistically promote sexual health. The present study aims to design and implement interventions to improve sexual health of women with endometriosis. To achieve this, the study will first explore the needs and strategies related to sexual health and then identify the effective strategies to improve sexual health in the literature review.
2. Materials and Methods
2.1. Study design
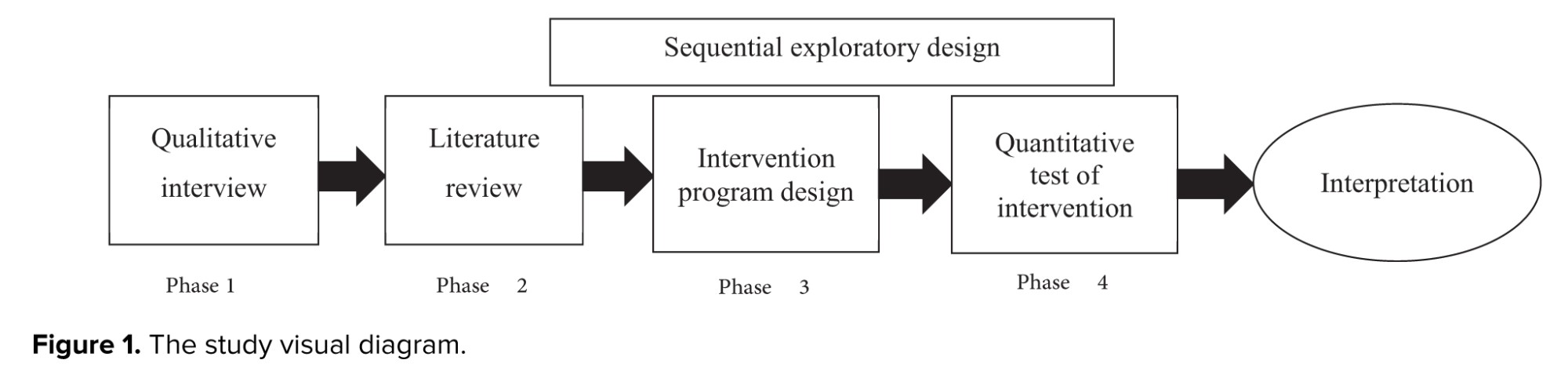
The present study protocol employs a sequential exploratory mixed-methods design consisting of 4 consecutive phases.
Endometriosis is a hormone-dependent chronic inflammatory disease affecting approximately 10% of women of reproductive age worldwide, making it the most common cause of chronic pelvic pain (1-4). This condition is associated with symptoms such as dyspareunia, dysmenorrhea, and dyschezia, which can lead to sexual dysfunction and negatively impact the quality of couples' sexual life and satisfaction (5-7). Studies indicate that 47-75% of women with endometriosis experience sexual dysfunction, including desire disorders, arousal issues, orgasm disorders, and deep dyspareunia, which disrupts the sexual response cycle (8-11). These sexual problems extend beyond physical pain, affecting mental activation, marital relationships, fertility, and overall well-being, encompassing psychological issues, reduced quality of life, and social challenges (12-18). Undertaking this study is essential because endometriosis profoundly affects all aspects of women's lives, yet sexual health is frequently overlooked in medical visits despite its critical role in fertility and relational stability (17, 18). Untreated sexual dysfunction can exacerbate isolation, depression, and partnership breakdowns, underscoring the need for targeted interventions to enhance sexual health and quality of life.
Previous studies have documented the multifaceted impacts of endometriosis on sexual function, highlighting strong associations with pain and reduced satisfaction, and have proposed various interventions (9-11, 16). Common treatments include surgical procedures to excise lesions and alleviate pain (19, 20), pharmacological options such as sedatives and progestins (21), couples therapy (22), use of vaginal lubricants, sexual counseling, and positional adjustments (16). However, these approaches have limitations: surgery and progesterone therapy reduce sexual pain in only 43-59% of cases, while hormonal treatments often cause vaginal dryness and exacerbate dyspareunia (13, 23). Psycho-sexual interventions remain limited, although emerging evidence suggests that, if expanded, they could effectively mitigate pain and related consequences; nevertheless, further research is required to confirm their efficacy in endometriosis patients (13).
Existing research predominantly relies on quantitative methods, inadequately exploring culture- and context-specific needs and overlooking qualitative insights from patients and service providers. This creates a knowledge gap: current interventions lack personalization, fail to address holistic sexual health strategies, and do not account for diverse socio-cultural factors, leaving many women with persistent, underserved sexual challenges. This study adds value by addressing this knowledge gap through a comprehensive, evidence-based program tailored to the unique needs of women with endometriosis. By conducting a qualitative exploration of perspectives from affected women and service providers, combined with a review of available resources, we develop targeted strategies that extend beyond symptom management to holistically promote sexual health. The present study aims to design and implement interventions to improve sexual health of women with endometriosis. To achieve this, the study will first explore the needs and strategies related to sexual health and then identify the effective strategies to improve sexual health in the literature review.
2. Materials and Methods
2.1. Study design
The present study protocol employs a sequential exploratory mixed-methods design consisting of 4 consecutive phases.
- Phase 1 is a qualitative study aimed at exploring the experiences, needs, and strategies related to sexual health among women with endometriosis and healthcare providers.
- Phase 2 involves a systematic review of the literature to identify evidence-based strategies for improving sexual health in this population.
- Phase 3 integrates findings from phases 1 and 2 to develop a comprehensive care program; the proposed components are then evaluated and prioritized by a multidisciplinary expert panel using the Delphi technique.
- Phase 4 comprises a randomized controlled trial (RCT) to assess the effectiveness of the developed intervention on sexual function and sexual quality of life in women with endometriosis compared to routine care (Figure 1).
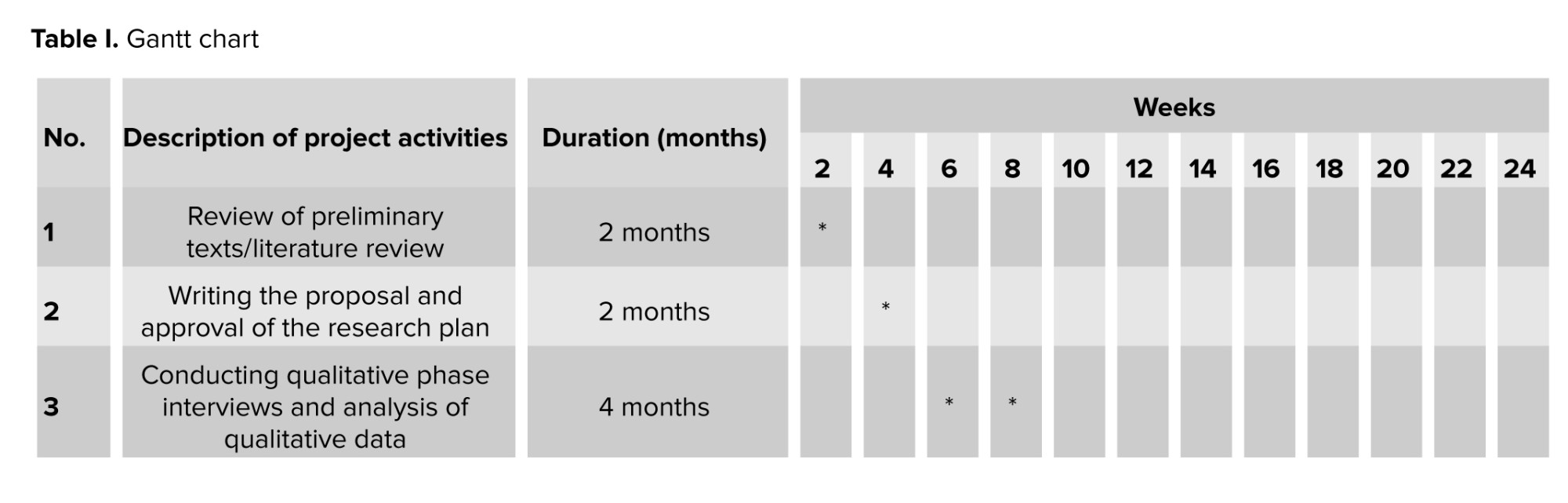
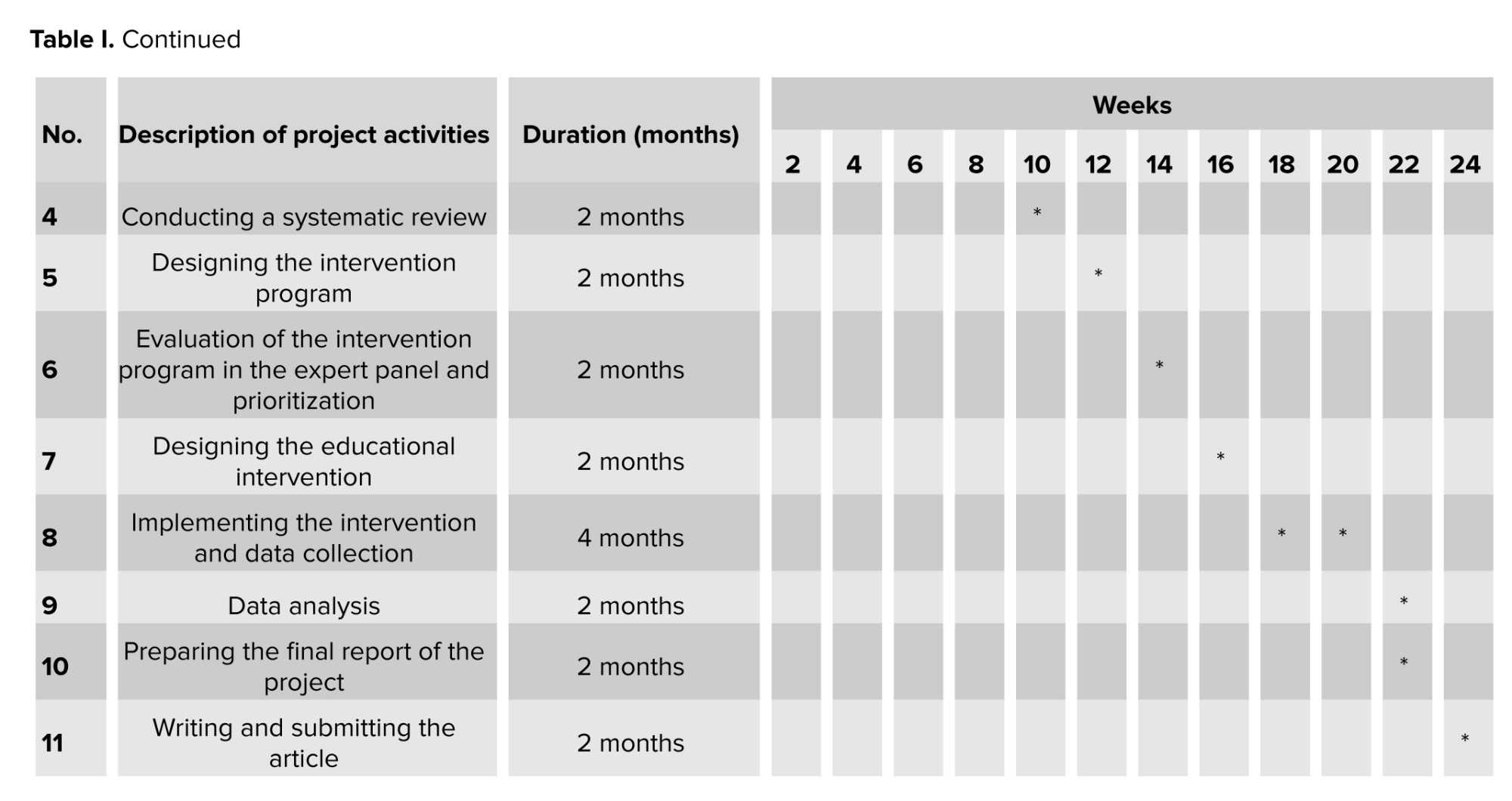
The project implementation schedule is presented in table I.
2.2. Study phases
2.2.1. Phase 1: qualitative phase
2.2.1.1. Study design
This phase explains the needs and strategies for improving the sexual health of women with endometriosis. All interviews are conducted in a place where the participants feel comfortable.
2.2.1.2. Inclusion and exclusion criteria
Women with endometriosis, Iranian nationality, and current residents of Yazd, according to the diagnosis of a gynecologist or the file available in the clinic, being Iranians, married, willingness to participate in the intervention, and ability to complete questionnaires. Women aged 18-45 yr. Cause of referral to the clinic: patients referred to gynecology clinic with a confirmed diagnosis of endometriosis. Main complaints: primarily deep dyspareunia, dysmenorrhea, or chronic pelvic pain. Duration of marriage/relationship: at least 1 yr of stable sexual relationship. Women who underwent oophorectomy, patients with concurrent pelvic inflammatory disease, pelvic masses unrelated to endometriosis (e.g., fibroids and ovarian cysts), recent pelvic surgery (within the past 12 months), other diagnosed causes of chronic pelvic pain, or sexual dysfunction (e.g., vaginismus, vulvodynia, or psychiatric illnesses affecting sexual health) were excluded from the study.
The healthcare providers must have at least 2 yr of experience in providing care of women with endometriosis.
2.2.1.3. Setting and sampling method
The study will be conducted in Baghaeipour Clinic in Yazd, Iran. The sampling method for the qualitative phase of the study will be purposive sampling. Participants in the qualitative phase of the study included women with endometriosis, with maximum variation in duration of endometriosis, social class, education, age, and occupation, as well as their partners and healthcare providers, including gynecologists, reproductive health specialists, psychiatrists, health professionals, sexologists, psychologists, and midwives affiliated with Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Healthcare providers must have at least 1 yr of experience, be actively involved in endometriosis care. The first interviewer, after introducing himself/herself, explaining the objectives of the study, and obtaining participants' consent to take part in the research, coordinates the time and location of the interview with them. The sample size continues until data saturation is reached.
2.2.1.4. Data collection
Semi-structured in-depth individual interviews will be used for the qualitative phase data collection after obtaining informed consent. The interviews with women with endometriosis are conducted in a quiet and private environment by the author, so that the participants can confidently talk about their sexual needs and problems. Interviews with the spouses of women with endometriosis about their sexual concerns and needs will be conducted with the informed consent of the women and their spouses. After obtaining the spouse's phone number, the spouse will be invited for a separate individual interview using a semi-structured guide. Interviews with the spouses will be conducted by the researcher over the phone. Interviews will be conducted with health care providers in clinics, offices, healthcare centers, and universities, and at the beginning of the interview, oral and written consent will be taken to participate in the research.
Based on the opinions of the research team and then during several preliminary interviews, an interview guide is prepared.
Guiding questions from the point of view of women with endometriosis:
2.2. Study phases
2.2.1. Phase 1: qualitative phase
2.2.1.1. Study design
This phase explains the needs and strategies for improving the sexual health of women with endometriosis. All interviews are conducted in a place where the participants feel comfortable.
2.2.1.2. Inclusion and exclusion criteria
Women with endometriosis, Iranian nationality, and current residents of Yazd, according to the diagnosis of a gynecologist or the file available in the clinic, being Iranians, married, willingness to participate in the intervention, and ability to complete questionnaires. Women aged 18-45 yr. Cause of referral to the clinic: patients referred to gynecology clinic with a confirmed diagnosis of endometriosis. Main complaints: primarily deep dyspareunia, dysmenorrhea, or chronic pelvic pain. Duration of marriage/relationship: at least 1 yr of stable sexual relationship. Women who underwent oophorectomy, patients with concurrent pelvic inflammatory disease, pelvic masses unrelated to endometriosis (e.g., fibroids and ovarian cysts), recent pelvic surgery (within the past 12 months), other diagnosed causes of chronic pelvic pain, or sexual dysfunction (e.g., vaginismus, vulvodynia, or psychiatric illnesses affecting sexual health) were excluded from the study.
The healthcare providers must have at least 2 yr of experience in providing care of women with endometriosis.
2.2.1.3. Setting and sampling method
The study will be conducted in Baghaeipour Clinic in Yazd, Iran. The sampling method for the qualitative phase of the study will be purposive sampling. Participants in the qualitative phase of the study included women with endometriosis, with maximum variation in duration of endometriosis, social class, education, age, and occupation, as well as their partners and healthcare providers, including gynecologists, reproductive health specialists, psychiatrists, health professionals, sexologists, psychologists, and midwives affiliated with Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Healthcare providers must have at least 1 yr of experience, be actively involved in endometriosis care. The first interviewer, after introducing himself/herself, explaining the objectives of the study, and obtaining participants' consent to take part in the research, coordinates the time and location of the interview with them. The sample size continues until data saturation is reached.
2.2.1.4. Data collection
Semi-structured in-depth individual interviews will be used for the qualitative phase data collection after obtaining informed consent. The interviews with women with endometriosis are conducted in a quiet and private environment by the author, so that the participants can confidently talk about their sexual needs and problems. Interviews with the spouses of women with endometriosis about their sexual concerns and needs will be conducted with the informed consent of the women and their spouses. After obtaining the spouse's phone number, the spouse will be invited for a separate individual interview using a semi-structured guide. Interviews with the spouses will be conducted by the researcher over the phone. Interviews will be conducted with health care providers in clinics, offices, healthcare centers, and universities, and at the beginning of the interview, oral and written consent will be taken to participate in the research.
Based on the opinions of the research team and then during several preliminary interviews, an interview guide is prepared.
Guiding questions from the point of view of women with endometriosis:
- Describe your experiences with sexual health.
- What sexual problems did endometriosis cause?
- What needs do you feel to improve your sexual health?
- In terms of sex, what services did you need and to whom or which centers did you go to receive them?
Guide questions from the perspective of healthcare providers:
- What concerns do women with endometriosis have regarding sexual issues?
- During the care of these women, what services did they need in terms of sexual health?
- What solutions do you suggest to improve the situation of providing sexual health services to these women?
2.2.1.5. Analysis
Qualitative content analysis will be used as the conventional approach for analyzing qualitative phase data. Conventional content analysis in this research will be done according to the steps suggested by Graneheim and Lundman (24), this method has the following 5 steps:
- Immediately after each interview, the interviews are transcribed.
- The whole transcribed text is read several times to get a general understanding of the content of the interview.
- Meaningful units are extracted, and coding is done.
- Primary codes are classified into subcategories, and categories are created based on the comparison of differences and similarities.
- Main themes are extracted from data concepts.
In this research, MAXQDA 2020 software is used for analysis.
2.2.1.6. Trustworthiness and validation strategies
4 criteria to ensure the reliability of the findings are: validity, confirmability, transferability, and reliability (25).
To ensure rigor and trustworthiness:
2.2.1.6. Trustworthiness and validation strategies
4 criteria to ensure the reliability of the findings are: validity, confirmability, transferability, and reliability (25).
To ensure rigor and trustworthiness:
- Member checking: summaries of key findings or transcripts will be returned to selected participants for verification and feedback on accuracy.
- Peer debriefing: regular discussions with an external qualitative researcher (not part of the core team) to review coding, categories, and emerging themes.
- Triangulation: data triangulation through multiple sources (women, healthcare providers, and potentially partners) and method triangulation (interviews + field notes).
- Audit trail: detailed documentation of all methodological decisions, interview transcripts, coding processes, and analytical memos will be maintained for transparency and confirmability.
2.2.2. Phase 2: literature review
2.2.2.1. Databases
In this phase, we will conduct a systematic review of the existing literature to determine evidence-based approaches for enhancing the sexual health of women living with endometriosis. The review process will follow the PRISMA guidelines for both conduct and reporting. To identify relevant studies, comprehensive searches will be carried out in the PubMed/MEDLINE, Scopus, and Web of Science electronic databases.
2.2.2.2. Search strategy
A comprehensive search strategy has been developed with an experienced researcher. The search combines terms related to the condition (endometriosis), outcomes/areas of interest (sexual health, sexual function, sexual quality of life, dyspareunia, sexual dysfunction, interventions, strategies, management), using controlled vocabulary (MeSH terms in PubMed) where applicable, and free-text terms.
Main keywords and synonyms (in English; Persian equivalents will be used if searching Persian databases, though currently focused on international databases):
- Endometriosis OR endometriosis OR endometriotic
- Sexual health OR sexual function OR sexual dysfunction OR sexual quality of life OR sexual wellbeing OR dyspareunia OR sexual pain OR libido OR arousal OR orgasm OR satisfaction
- Intervention* OR strategy/strategies OR management OR treatment* OR program* OR therapy* OR counsel* OR education OR psychosocial OR psychosexual OR multidisciplinary
Boolean operators and example complete search strings (adapted for each database):
PubMed example (using MeSH and free text): ("Endometriosis"[Mesh] OR endometri) AND ("Sexual Dysfunction, Physiological"[Mesh] OR "Sexuality"[Mesh] OR sexual OR sex* function* OR sex* health OR dyspareunia OR "quality of sexual life" OR "sexual quality of life" OR FSFI OR SQoL) AND (intervention* OR strateg* OR manage* OR treat* OR therap* OR counsel* OR educat* OR psychosocial OR psychosexual OR multidisciplin*).
Scopus example: TITLE-ABS-KEY (endometri) AND TITLE-ABS-KEY ("sexual function" OR "sexual health" OR "sexual dysfunction" OR dyspareunia OR "sexual quality of life" OR "sexual wellbeing") AND TITLE-ABS-KEY (intervention* OR strateg* OR program* OR therap* OR counsel* OR educat* OR psychosocial).
Web of Science example: TS = (endometri AND (sexual NEAR/5 (function OR health OR dysfunction OR quality OR pain OR dyspareunia)) AND (intervention* OR strateg* OR manage* OR therap* OR counsel* OR educat*)).
The search will be conducted without language restrictions (though full-text review will prioritize English and Persian articles).
2.2.2.3. Time frame
No lower date limit; searches from database inception until October 2024. The field of sexual health in endometriosis is relatively young and evolving, with important foundational qualitative, observational, and early interventional studies published before 2000 still providing valuable insights into needs, experiences, and initial management approaches.
2.2.2.4. Inclusion and exclusion criteria
This review will include original research articles, full-length studies, and articles that focus on the impact of endometriosis on women's sexual health, in both Farsi and English. Inclusion criteria (using PICOS framework):
PubMed example (using MeSH and free text): ("Endometriosis"[Mesh] OR endometri) AND ("Sexual Dysfunction, Physiological"[Mesh] OR "Sexuality"[Mesh] OR sexual OR sex* function* OR sex* health OR dyspareunia OR "quality of sexual life" OR "sexual quality of life" OR FSFI OR SQoL) AND (intervention* OR strateg* OR manage* OR treat* OR therap* OR counsel* OR educat* OR psychosocial OR psychosexual OR multidisciplin*).
Scopus example: TITLE-ABS-KEY (endometri) AND TITLE-ABS-KEY ("sexual function" OR "sexual health" OR "sexual dysfunction" OR dyspareunia OR "sexual quality of life" OR "sexual wellbeing") AND TITLE-ABS-KEY (intervention* OR strateg* OR program* OR therap* OR counsel* OR educat* OR psychosocial).
Web of Science example: TS = (endometri AND (sexual NEAR/5 (function OR health OR dysfunction OR quality OR pain OR dyspareunia)) AND (intervention* OR strateg* OR manage* OR therap* OR counsel* OR educat*)).
The search will be conducted without language restrictions (though full-text review will prioritize English and Persian articles).
2.2.2.3. Time frame
No lower date limit; searches from database inception until October 2024. The field of sexual health in endometriosis is relatively young and evolving, with important foundational qualitative, observational, and early interventional studies published before 2000 still providing valuable insights into needs, experiences, and initial management approaches.
2.2.2.4. Inclusion and exclusion criteria
This review will include original research articles, full-length studies, and articles that focus on the impact of endometriosis on women's sexual health, in both Farsi and English. Inclusion criteria (using PICOS framework):
- Population: women diagnosed with endometriosis
- Intervention/exposure: any type of intervention, strategy, management approach, or treatment aimed at improving sexual health, sexual function, sexual quality of life, reducing dyspareunia, or addressing related sexual problems (including medical, surgical, psychological, educational, counseling, multidisciplinary, self-management, etc.)
- Comparator: may include usual care, no intervention, placebo, or another active treatment
- Outcomes: primary focus on sexual function (e.g., FSFI score/domains), sexual quality of life (e.g., SQOL), dyspareunia severity, sexual satisfaction, desire/arousal/orgasm, or related qualitative themes
- Study designs: all original research designs will be included to capture the broadest evidence base for intervention development: RCTs, non-RCTs, quasi-experimental studies, observational studies (cohort, case-control, cross-sectional), qualitative studies, mixed-methods studies, case series/reports (if providing novel strategies), and systematic reviews/meta-analyses (for reference mining).
Exclusion criteria:
- Articles without accessible full text
- Short communications, letters, editorials, conference abstracts, protocols (unless they describe unique interventions not yet published in full), narrative reviews (though used for background and reference checking)
- Studies focused solely on pain, fertility, or general quality of life without any specific sexual health outcome/component.
2.2.2.5. Study selection and quality assessment
2 reviewers will independently screen the titles and abstracts of identified records based on pre-established inclusion criteria. Any studies considered potentially relevant will have their full texts obtained and evaluated separately by the same reviewers. If any disagreements arise, they will be addressed through discussion, and if necessary, by involving a third reviewer.
The evaluation of study quality and risk of bias will be adapted according to the specific study design:
- For RCTs, the Cochrane Risk of Bias 2 (RoB 2) tool will be utilized.
- For non-randomized interventional or observational studies, Risk of Bias in Non-randomized Studies of Interventions. For descriptive/observational studies without intervention comparison: Modified versions of relevant tools (e.g., Newcastle-Ottawa scale where appropriate)
- For qualitative studies: Consolidated Criteria for Reporting Qualitative Research (COREQ)
- For reporting observational studies (if relevant): STROBE checklist
The minimum acceptable quality threshold will be applied flexibly depending on study type (e.g., STROBE ≥ 15/22 for observational; Consolidated Criteria for Reporting Qualitative Research ≥ most items reported); however, no studies will be excluded solely based on quality, poor-quality studies will be noted, and their findings interpreted cautiously.
2.2.2.6. Data extraction
A standardized form will be used to extract: study characteristics, population, intervention details/strategies, outcomes related to sexual health, key qualitative findings/themes, and limitations.
Combining data from qualitative research with a literature review: after extracting the main codes from the interviews of the qualitative phase and reviewing the literature, the findings of the first and second phases of the study will be integrated. Then, the initial draft of the needs and strategies to improve the sexual health of women with endometriosis is prepared.
2.2.3. Phase 3: intervention program design
Scoping the solutions priorities to facilitate an effective intervention program for improving the sexual health of women with endometriosis.
The sampling frame and selection of experts will involve purposive recruitment of Delphi panel members who are specialists or experts with recognized experience in endometriosis care and/or sexual and reproductive health.
The sampling frame includes professionals from the following groups (with representation aimed across all categories to ensure multidisciplinary input):
2.2.2.6. Data extraction
A standardized form will be used to extract: study characteristics, population, intervention details/strategies, outcomes related to sexual health, key qualitative findings/themes, and limitations.
Combining data from qualitative research with a literature review: after extracting the main codes from the interviews of the qualitative phase and reviewing the literature, the findings of the first and second phases of the study will be integrated. Then, the initial draft of the needs and strategies to improve the sexual health of women with endometriosis is prepared.
2.2.3. Phase 3: intervention program design
Scoping the solutions priorities to facilitate an effective intervention program for improving the sexual health of women with endometriosis.
The sampling frame and selection of experts will involve purposive recruitment of Delphi panel members who are specialists or experts with recognized experience in endometriosis care and/or sexual and reproductive health.
The sampling frame includes professionals from the following groups (with representation aimed across all categories to ensure multidisciplinary input):
- Midwives and reproductive health specialists (with experience in sexual health counseling or endometriosis management)
- Gynecologists and obstetricians (subspecialty in endometriosis, pelvic pain)
- Psychiatrists and clinical psychologists (with expertise in psychosexual issues or women's mental health)
- Sexologists/sexual health specialists/counselors (certified or with documented clinical practice in sexual dysfunction or couple therapy)
Experts will be recruited from academic centers (universities and research institutes), teaching hospitals, specialized gynecology/endometriosis clinics, sexual health clinics, and private practices affiliated with Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Inclusion criteria for experts:
Inclusion criteria for experts:
- At least 1 yr of clinical and/or academic experience directly related to endometriosis care, sexual health of women, or psychosexual counseling
- Current or recent active involvement in patient care, teaching, or research in the above fields
- Willingness and availability to participate in 2 rounds of Delphi (via email/online platform)
We aim to recruit 20 experts. This sample size is justified based on published recommendations in health sciences and Delphi methodology literature, which commonly suggest panel sizes of 10-30 experts for achieving reliable consensus. 20 experts allow sufficient diversity across professions while remaining manageable for response tracking, data analysis, and maintaining high response rates across rounds.
2.2.3.1. Implementation of Delphi phase 1
The Delphi panel will be used in 2 rounds to evaluate and prioritize the sexual health promotion program components for women with endometriosis.
In round 1, the initial version of the program (developed by integrating findings from phases 1 and 2) will be sent to experts via email or a secure online survey platform. Each proposed component/solution/strategy will be rated independently on a 4-point Likert-type scale of priority:
1 = least priority
2 = low priority
3 = high priority
4 = highest priority
Experts will also be invited to provide qualitative comments, suggest modifications, or propose additional items.
After receiving responses, the mean score and standard deviation for each item will be calculated using SPSS version 25. Items will also be ranked by mean score.
2.2.3.2. Implementation of Delphi phase 2
In round 2, experts will receive anonymized aggregated results from round 1 (means, standard deviation, rankings, and summarized qualitative comments). They will then re-rate the items and evaluate the most promising solutions using a decision matrix based on 4 practical criteria:
2.2.3.1. Implementation of Delphi phase 1
The Delphi panel will be used in 2 rounds to evaluate and prioritize the sexual health promotion program components for women with endometriosis.
In round 1, the initial version of the program (developed by integrating findings from phases 1 and 2) will be sent to experts via email or a secure online survey platform. Each proposed component/solution/strategy will be rated independently on a 4-point Likert-type scale of priority:
1 = least priority
2 = low priority
3 = high priority
4 = highest priority
Experts will also be invited to provide qualitative comments, suggest modifications, or propose additional items.
After receiving responses, the mean score and standard deviation for each item will be calculated using SPSS version 25. Items will also be ranked by mean score.
2.2.3.2. Implementation of Delphi phase 2
In round 2, experts will receive anonymized aggregated results from round 1 (means, standard deviation, rankings, and summarized qualitative comments). They will then re-rate the items and evaluate the most promising solutions using a decision matrix based on 4 practical criteria:
- Ease of implementation (1 = very difficult → 3 = very easy)
- Time required for implementation (1 = high time demand → 3 = low time demand)
- Cost of implementation (1 = high cost → 3 = low cost)
- Expected effectiveness/potential impact (1 = low → 3 = high)
For each remaining/program component, experts assign a score of 1-3 on each of the 4 criteria. A total weighted decision matrix score will be calculated for each component as follows: decision matrix score = (ease score × 0.25) + (time score × 0.25) + (cost score × 0.25) + (effectiveness score × 0.25) (equal weighting of 25% for each criterion; weights can be adjusted post-hoc if consensus emerges on differential importance)
Thresholds for acceptance/rejection/prioritization:
Thresholds for acceptance/rejection/prioritization:
- Components with a final mean decision matrix score ≥ 2.4 (out of 3.0) will be considered high priority and retained for inclusion in the final intervention program.
- Components with mean score of 2.0-2.39 will be classified as moderate priority (may be included with modifications or as optional elements).
- Components below 2.0 will be rejected or substantially revised unless strong qualitative justification is provided by multiple experts.
Consensus will be defined as ≥ 75% of experts rating an item/component in the top 2 categories (high/highest priority in round 1; or matrix score ≥ 2.4 in round 2), supplemented by stability of ratings between rounds and qualitative convergence.
The final prioritized program components will form the basis for the intervention to be tested in phase 4.
2.2.4. Phase 4: quantitative phase
2.2.4.1. Specific objectives
The primary objective is to evaluate the effectiveness of the developed intervention program compared to routine care on sexual function in women with endometriosis.
Primary outcome: change in total Female Sexual Function Index (FSFI) score from baseline to immediately post-intervention and to 2-month follow-up.
Secondary outcomes:
The final prioritized program components will form the basis for the intervention to be tested in phase 4.
2.2.4. Phase 4: quantitative phase
2.2.4.1. Specific objectives
The primary objective is to evaluate the effectiveness of the developed intervention program compared to routine care on sexual function in women with endometriosis.
Primary outcome: change in total Female Sexual Function Index (FSFI) score from baseline to immediately post-intervention and to 2-month follow-up.
Secondary outcomes:
- Changes in the 6 domain scores of the FSFI (desire, arousal, lubrication, orgasm, satisfaction, pain)
- Change in total Sexual Quality of Life Questionnaire (SQOL) score.
2.2.4.2. Sample size
Sample size was calculated using G*Power software. We assumed a small-to-moderate effect size of Cohen's d = 0.35 for the primary outcome (total FSFI score change), based on previous intervention studies in women with endometriosis or chronic pelvic pain showing standardized mean differences in sexual function outcomes ranging from 0.3-0.6 after psycho-educational or multidisciplinary interventions. Parameters: α = 0.05, power (1-β) = 0.90, correlation among repeated measures = 0.5, no sphericity correction ε = 0.75. This yields approximately 28-30 participants per group (total n ≈ 56-60). Anticipating an attrition rate of up to 20% (based on dropout rates of 15-30% reported in similar RCTs of behavioral/educational interventions in women with endometriosis and chronic pelvic pain), we inflate the sample to 35-38 per group (total n = 70-76). The final target sample size is 70 women (35 per group) to ensure adequate power even with moderate attrition.
2.2.4.3. Randomization and allocation concealment
Eligible participants will be randomly allocated to either the intervention group or the control group in a 1:1 ratio. The randomization sequence will be generated using computer software by an independent statistician who is not involved in the participant recruitment process or in the assessment of study outcomes.
Randomization will be performed in permuted blocks of size 4 or 6 (randomly varying block sizes to prevent prediction) to balance potential prognostic factors. Allocation concealment will be maintained through the use of sequentially numbered, opaque, sealed envelopes, which will be prepared in advance by the independent statistician. Envelopes will be opened only after baseline assessment and informed consent, by a researcher not involved in data collection. Blinding: due to the nature of behavioral/educational intervention, participants and intervention deliverers cannot be blinded. Data analysts will also be blinded during primary analysis (group codes will be concealed until analysis completion).
The control group will receive routine care (standard gynecological follow-up and management in the study setting).
2.2.4.4. Eligibility criteria
Inclusion criteria:
- Confirmed diagnosis of endometriosis by a gynecologist (clinical, imaging, or surgical evidence documented in medical records)
- Iranian nationality and resident of Yazd
- Aged 18-45 yr
- Married and sexually active, operationally defined as having engaged in vaginal sexual intercourse at least once in the past 4 wk and reporting a stable marital/sexual relationship of at least 1 yr
- Willing and able to provide informed consent and complete study procedures/questionnaires
- Referred to gynecology clinic primarily for deep dyspareunia, dysmenorrhea, or chronic pelvic pain.
Exclusion criteria:
- History of bilateral oophorectomy
- Concurrent pelvic inflammatory disease diagnosed clinically or by imaging
- Pelvic masses unrelated to endometriosis (e.g., large symptomatic fibroids > 5 cm, complex ovarian cysts)
- Pelvic surgery within the past 12 months
- Other primary causes of chronic pelvic pain (e.g., interstitial cystitis, irritable bowel syndrome with predominant pelvic symptoms)
- Primary sexual dysfunction unrelated to endometriosis (e.g., diagnosed vaginismus, vulvodynia)
- Severe psychiatric disorders (e.g., psychosis, schizophrenia requiring active treatment, documented in medical records or self-report)
- Pregnancy at enrollment
- Participation in another sexual health or psychological intervention study concurrently
- Cancer (any active malignancy)
- Other severe chronic diseases significantly affecting sexual function (e.g., uncontrolled diabetes with neuropathy, severe cardiovascular disease, advanced multiple sclerosis, assessed via self-report, medical history review, and clinician confirmation if needed)
- Drug or alcohol dependence (self-report or medical record)
- Use of medications/hormones known to significantly affect sexual function within 60 days prior to enrollment (e.g., certain antidepressants, antipsychotics, high-dose opioids)
- Major stressful life events in the past 6 months (e.g., recent bereavement, divorce, immigration, severe financial crisis, assessed by self-report)
2.2.4.5. Scales and data collection Instruments
The instruments for collecting data will be the personal-social information questionnaire and the FSFI, and the SQOL. Study questionnaires are completed by the participants before the intervention, immediately and 2 months after the intervention.
2.2.4.5.1. Personal–social information form
The personal-social information form will include details such as age, family economic status, education level of the participant, employment status, and other relevant information. This form will be completed upon the participants’ entry into the study.
2.2.4.5.2. FSFI
FSFI, is a self‑reported instrument consisting of 19 items that evaluate women’s sexual function during the previous 4 wk. The questionnaire measures 6 domains: sexual desire (2 items), arousal (4 items), lubrication (4 items), orgasm (3 items), satisfaction (3 items), and pain (3 items). Items are rated on a 5‑point Likert scale; while most items are scored from 1-5, some include a score of 0 to indicate no sexual activity. Domain scores are obtained by summing the relevant items and multiplying the result by a specific domain factor (0.6 for desire; 0.3 for arousal and lubrication; and 0.4 for orgasm, satisfaction, and pain), resulting in domain scores ranging from 0-6 (with the desire domain ranging from 1.2-6). The overall FSFI score ranges from 2-36, with higher scores reflecting better sexual function. The Persian version of this questionnaire has also been validated (26).
2.2.4.5.3. SQOL-female
The SQOL questionnaire was designed and developed to measure the sexual quality of life. An 18-item self-report measure assessing the impact of sexual function on quality of life. Items are scored on a 6-point Likert scale (1 = completely agree to 6 = completely disagree, with reverse scoring for positively worded items). Total score ranges from 18-108, with higher scores indicating better sexual quality of life. Maasoumi and Montazeri in 2013 confirmed the validity and reliability of the Farsi version of this questionnaire for the first time in Iran (27).
2.3. Ethical Considerations
Ethical approval for this protocol study has been obtained from the research ethics committees of Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.RSI.REC.1401.018). Registration of a randomized controlled clinical trial has been accomplished with the Iranian Registry of Clinical Trials (IRCT20220620055229N2).
2.4. Statistical Analysis
The primary analysis will be conducted on an intention-to-treat basis, including all randomized participants in their assigned group regardless of protocol adherence or dropout. A secondary per‑protocol analysis will be performed for sensitivity, including only participants who completed at least 80% of the intervention sessions and provided outcome data at all time points. For continuous outcomes (FSFI total/domain scores, SQOL total score), we will use linear mixed-effects models (repeated measures) with time, group, and time × group interaction as fixed effects, participant as random effect, and adjustment for baseline score and stratification variables (age group). This approach handles missing data under the missing-at-random assumption and is superior to last-observation-carried-forward. If substantial missingness occurs (> 15-20%), multiple imputations (e.g., 20-30 imputations) by chained equations will be used as a sensitivity analysis. Categorical outcomes (e.g., proportion achieving clinically meaningful improvement in FSFI ≥ 4 points) will be analyzed using Chi-square or logistic regression. Effect sizes (Cohen's d or partial eta-squared) will be reported. Statistical significance will be set at p < 0.05 (2-tailed). Analyses will be performed using SPSS version 25.
3. Discussion
Several studies have highlighted the profound negative impact of endometriosis on women's sexual health, including high rates of dyspareunia, reduced sexual desire, arousal difficulties, orgasmic dysfunction, and overall diminished sexual quality of life (9-11, 13, 16, 23). Despite these well-documented challenges, sexual health concerns are frequently overlooked in routine clinical care, and existing interventions often remain limited to pain management (surgical or pharmacological), with only partial success in alleviating sexual symptoms (13, 19-21, 23). Psycho-sexual and educational approaches show promise but lack comprehensive, culturally tailored programs, particularly in contexts like Iran, where socio-cultural factors, stigma around sexual discussions, and limited access to specialized sexual health services may further compound the burden (17, 18, 28, 29).
This mixed-methods study protocol addresses these gaps by systematically developing and evaluating a targeted, evidence-based intervention program. The sequential design integrates qualitative insights from affected women and healthcare providers (phase 1), evidence from a systematic review (phase 2), expert prioritization via Delphi (phase 3), and rigorous RCT evaluation (phase 4). This approach is expected to yield a holistic, contextually relevant program that goes beyond symptom relief to address emotional, relational, and socio-cultural dimensions of sexual health.
Potential contributions and expected impact, if effective, the developed intervention could offer several important contributions: provide the first comprehensive, culturally adapted sexual health promotion program specifically for Iranian women with endometriosis, filling a critical gap in localized, patient-centered care. Demonstrate the feasibility and preliminary effectiveness of a multidisciplinary, non-pharmacological approach combining education, counseling, self-management strategies, and relational support. Generate evidence to inform clinical guidelines, midwifery and gynecology practice, and policy-making regarding integration of sexual health assessment and intervention into routine endometriosis management. Contribute to broader reproductive health literature by illustrating the value of mixed-methods sequential designs in developing complex behavioral interventions for chronic gynecological conditions.
Foreseeable limitations and mitigation strategies as with any prospective interventional study, several limitations and challenges can be anticipated:
- Self-report bias: primary outcomes rely on validated self-report questionnaires (FSFI and SQOL), which may be influenced by social desirability, recall bias, or cultural reluctance to disclose sensitive sexual information. Using validated Persian instruments with proven psychometric properties in Iranian populations, ensuring complete anonymity and confidentiality, administering by a trained, blinded female rater in private settings, and integrating quantitative findings with qualitative insights from phase 1 mitigate this limitation.
- Attrition and loss to follow-up: behavioral interventions requiring participant engagement may experience dropout, particularly over the 2-month follow-up period. Sample size inflation for up to 20% attrition; use of multiple reminders (phone, SMS); flexible scheduling of sessions; and intention-to-treat analysis with mixed-effects models to handle missing data appropriately mitigate this limitation.
- Cultural and contextual constraints in Iran, stigma surrounding sexual health discussions, gender norms, and limited partner involvement may affect recruitment, intervention uptake, and outcome reporting. Culturally sensitive recruitment and data collection (female interviewers, private settings); optional partner involvement only with explicit consent; integration of cultural considerations throughout program design via phase 1 qualitative data and Delphi expert panel; and monitoring of recruitment feasibility and acceptability during the trial mitigate this limitation.
- Generalizability: the single-center design and focus on Yazd may limit applicability to other regions or socio-economic groups. Purposive maximum variation sampling in qualitative phase; recruitment from multiple clinic types; a clear description of context for future multicenter adaptation mitigates this limitation.
- Blinding challenges: participants and intervention deliverers cannot be blinded to group allocation in a behavioral trial. Blinding of outcome assessors and data analysts, use of objective validated scales, and transparent reporting of potential performance/detection bias mitigate this limitation.
Overall, this protocol represents a rigorous step toward addressing an underserved aspect of endometriosis care. The findings, once available, are expected to inform future larger-scale trials, guideline development, and improved multidisciplinary sexual health support for women living with endometriosis in Iran and similar settings.
3.1. Recommendations
This study anticipates several challenges, including participant recruitment and retention due to the sensitive nature of the topic and disease-related fatigue, intervention fidelity in delivering a multi-component program, cultural constraints surrounding open discussion of sexual issues, and limited generalizability resulting from the single-center design. The mixed-methods sequential design addresses these issues through purposive maximum variation sampling and cultural tailoring in phases 1 and 3, flexible scheduling, a 20% attrition buffer in sample size calculation, development of a detailed intervention manual, facilitator training, and ongoing process evaluation (attendance, engagement, and acceptability).
The results of this study will be shared through publications in peer‑reviewed scientific journals and by delivering presentations at both national and international conferences, and preparation of summary reports for participating clinics, professional associations, and reproductive health policy units within the Ministry of Health. If the intervention proves effective, future research will include multicenter randomized trials across major Iranian cities, longer-term follow-up (6-12 months or more), development of digital or hybrid delivery formats for wider accessibility, couple-inclusive designs, and cost-effectiveness analyses to support broader implementation and scaling of the program.
4. Conclusion
Endometriosis significantly impairs sexual function and quality of life in affected women, yet targeted, culturally appropriate interventions addressing these aspects remain limited, particularly in contexts where sexual health is under-discussed in routine care. This mixed-methods protocol was developed to systematically address this gap by integrating qualitative exploration of needs and barriers (phase 1), evidence synthesis from a systematic review (phase 2), expert consensus prioritization (phase 3), and rigorous evaluation through a RCT (phase 4). The resulting program is expected to offer a holistic, evidence-based, and contextually tailored approach to improving sexual health outcomes beyond conventional pain-focused management.
Methodologically, this study contributes to the growing use of sequential mixed-method designs for developing and testing complex behavioral interventions in reproductive health, providing a replicable framework that combines stakeholder perspectives, systematic evidence, and Delphi prioritization before definitive RCT evaluation. The RCT component is particularly significant as it will generate preliminary evidence on the feasibility, acceptability, and effectiveness of the intervention in a real-world clinical setting, addressing a key limitation in the current literature where most existing approaches lack controlled empirical testing. Ultimately, successful implementation of this protocol may support the integration of sexual health assessment and targeted support into multidisciplinary endometriosis care pathways.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
F. ZareMobini and T. Farajkhoda contributed to the study design and conducted the research. F. ZareMobini, T. Farajkhoda, A. Javaheri, Sh. Mohamadkhani, and M. Sarebanhassanabadi participated in manuscript revision. All authors read and approved the final manuscript and take responsibility for the integrity and accuracy of the data.
Acknowledgements
The authors would like to thank Shahid Sadoughi University of Medical Sciences, Yazd, Iran for supporting this research. This research protocol was funded by the Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Grant no. 15083). ChatGPT (OpenAI, GPT‑5.2 model) was used for grammar checking.
Conflict of Interest
The authors declare that there is no conflict of interest.
3.1. Recommendations
This study anticipates several challenges, including participant recruitment and retention due to the sensitive nature of the topic and disease-related fatigue, intervention fidelity in delivering a multi-component program, cultural constraints surrounding open discussion of sexual issues, and limited generalizability resulting from the single-center design. The mixed-methods sequential design addresses these issues through purposive maximum variation sampling and cultural tailoring in phases 1 and 3, flexible scheduling, a 20% attrition buffer in sample size calculation, development of a detailed intervention manual, facilitator training, and ongoing process evaluation (attendance, engagement, and acceptability).
The results of this study will be shared through publications in peer‑reviewed scientific journals and by delivering presentations at both national and international conferences, and preparation of summary reports for participating clinics, professional associations, and reproductive health policy units within the Ministry of Health. If the intervention proves effective, future research will include multicenter randomized trials across major Iranian cities, longer-term follow-up (6-12 months or more), development of digital or hybrid delivery formats for wider accessibility, couple-inclusive designs, and cost-effectiveness analyses to support broader implementation and scaling of the program.
4. Conclusion
Endometriosis significantly impairs sexual function and quality of life in affected women, yet targeted, culturally appropriate interventions addressing these aspects remain limited, particularly in contexts where sexual health is under-discussed in routine care. This mixed-methods protocol was developed to systematically address this gap by integrating qualitative exploration of needs and barriers (phase 1), evidence synthesis from a systematic review (phase 2), expert consensus prioritization (phase 3), and rigorous evaluation through a RCT (phase 4). The resulting program is expected to offer a holistic, evidence-based, and contextually tailored approach to improving sexual health outcomes beyond conventional pain-focused management.
Methodologically, this study contributes to the growing use of sequential mixed-method designs for developing and testing complex behavioral interventions in reproductive health, providing a replicable framework that combines stakeholder perspectives, systematic evidence, and Delphi prioritization before definitive RCT evaluation. The RCT component is particularly significant as it will generate preliminary evidence on the feasibility, acceptability, and effectiveness of the intervention in a real-world clinical setting, addressing a key limitation in the current literature where most existing approaches lack controlled empirical testing. Ultimately, successful implementation of this protocol may support the integration of sexual health assessment and targeted support into multidisciplinary endometriosis care pathways.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
F. ZareMobini and T. Farajkhoda contributed to the study design and conducted the research. F. ZareMobini, T. Farajkhoda, A. Javaheri, Sh. Mohamadkhani, and M. Sarebanhassanabadi participated in manuscript revision. All authors read and approved the final manuscript and take responsibility for the integrity and accuracy of the data.
Acknowledgements
The authors would like to thank Shahid Sadoughi University of Medical Sciences, Yazd, Iran for supporting this research. This research protocol was funded by the Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Grant no. 15083). ChatGPT (OpenAI, GPT‑5.2 model) was used for grammar checking.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Psycology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
