
International Journal of
Reproductive Biomedicine
Mon, Jul 6, 2026
[Archive]
Volume 24, Issue 1 (January 2026)
IJRM 2026, 24(1): 71-78 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseini F, Safi F, Ahmadi F. An unrecognized non-pathologic filling defect on hysterosalpingography: A case report. IJRM 2026; 24 (1) :71-78
URL: http://ijrm.ir/article-1-3681-en.html
URL: http://ijrm.ir/article-1-3681-en.html



1- Department of Reproductive Imaging, Reproductive Biomedicine Research Center, Royan Institute for Reproductive Biomedicine, ACECR, Tehran, Iran.
2- Department of Radiology, School of Medicine, Arak University of Medical Sciences, Arak, Iran.
3- Department of Reproductive Imaging, Reproductive Biomedicine Research Center, Royan Institute for Reproductive Biomedicine, ACECR, Tehran, Iran. ,dr.ahmadi1390@gmail.com; f.ahmadi@royan-rc.ac.ir
2- Department of Radiology, School of Medicine, Arak University of Medical Sciences, Arak, Iran.
3- Department of Reproductive Imaging, Reproductive Biomedicine Research Center, Royan Institute for Reproductive Biomedicine, ACECR, Tehran, Iran. ,
Full-Text [PDF 1515 kb]
(455 Downloads)
| Abstract (HTML) (413 Views)
Full-Text: (122 Views)
1. Introduction
Hysterosalpingography (HSG) is one of the most widely used diagnostic tools for evaluating primary and secondary infertility. Despite the advent of advanced techniques, it remains the best non-surgical method for assessing the fallopian tubes. Routine evaluation of hysterosalpingograms also involves assessing the uterine cavity for any intrauterine abnormality. One of the most common abnormalities detected on HSG is a filling defect, which can represent a spectrum of intrauterine abnormalities, including submucosal fibroids, endometrial polyps, endometrial hyperplasia, synechiae, and, less frequently, nonpathological cases such as artifacts and normal variations. Uterine cavity abnormalities can cause single or multiple filling defects with regular or irregular margins (1-3). These abnormalities can significantly impact reproductive health, particularly in the context of infertility. In consequence, accurate differentiation between these entities is crucial for appropriate patient management. A definitive diagnosis requires further evaluation, such as saline infusion sonography (SIS), magnetic resonance imaging (MRI), or hysteroscopy.
However, further investigations might reveal that the uterine cavity is actually normal. This report presents a case of polypoid filling defects observed on HSG, where subsequent transvaginal sonography (TVS), SIS, and hysteroscopy revealed no underlying pathology. The broad spectrum of underlying pathologies make difficulties in diagnosis and interpretation of filling defects; therefore, further evaluation is crucial for accurate diagnosis and appropriate management.
2. Case Presentation
A 35-yr-old woman with primary infertility for 10 yr referred to Royan Institute, Tehran, Iran, and underwent HSG to evaluate tubal patency at our institution.
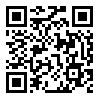
The participant denied a history of prior genital tract surgery. She did not have diabetes, hypertension, or thyroid dysfunction. She was a non-smoker with a body mass index of 28 and regular menstrual cycles. The participant’s medical record included blood test results with parameters within the normal range and a TVS report, which had been performed on day 7 of cycle, showing a normal endometrial thickness of 6 mm with a normal endometrial echo pattern and margins (Figure 1A).
The HSG performed on the participant revealed multiple filling defects throughout the uterine cavity, raising initial suspicion of polypoid hyperplasia or multiple polyps (Figure 1B). Further administration of the contrast agent induced no appreciable alteration in this HSG finding, excluding displacement of the filling defect attributed to an air bubble. The HSG showed normal findings in the fallopian tubes, with free spillage of contrast material into the peritoneal cavity. The participant was recommended for further evaluation. Next, SIS was performed, showing a normal endometrium with no evidence of polyps (Figure 1C).
Diagnostic hysteroscopy was subsequently undertaken and revealed no abnormalities. An endometrial biopsy was performed under direct hysteroscopic visualization, and the histopathology report confirmed the presence of normal endometrial tissue.
2.1. HSG protocol
A Shimadzu (Flexavision model) Dynamic Digital Radiography machine was used to perform this test. Using a cannula technique under fluoroscopic guidance, water-soluble contrast material (IODIXANOL-320) was slowly instilled into the uterus via the cervical canal in 3 stages. Each injection contained 2-3 cc of contrast material. After each injection, an image was acquired. The first image was obtained during early filling of the uterine cavity to evaluate for any filling defects or contour abnormalities; this stage is optimal for detecting small filling defects. The second image was acquired when the uterine cavity was fully distended, and the fallopian tubes were opacified. The third image was obtained to assess tubal patency. A fourth image was taken 20 min after the completion of the procedure to demonstrate the dispersion of contrast material within the peritoneal cavity.
2.2. SIS protocol
SIS was performed using a Samsung WS-80 ultrasound system and a 5-8 MHz transvaginal probe. Under aseptic conditions and ultrasound guidance, 5-10 cc of sterile saline solution was slowly injected into the uterine cavity through a Foley catheter (No. 8). The uterus was gradually distended, and as the uterine cavity filled with fluid, ultrasound images of the endometrium and uterine cavity were acquired and evaluated. The advantage of using saline as a negative contrast agent lies in its ability to create an echo-free background, which facilitates clear visualization of intrauterine abnormalities.
2.3. Ethical Considerations
Informed consent was obtained from the participant prior to the HSG exam. Their anonymity and confidentiality were ensured throughout the study.
3. Discussion
Imaging plays a major role in female infertility evaluation. Despite advanced imaging methods such as ultrasound, sonohysterography, and MRI, HSG remains one of the most frequently used methods to evaluate the uterine cavity and tubal patency (4, 5). In normal HSG, the uterine cavity is shown in an inverted triangular shape with no persistent filling defect and a well-defined smooth margin (1, 3, 5, 6).
Filling defects on HSG are areas where contrast dye fails to fill the uterine cavity. These defects are among the most frequently observed abnormalities on HSG and may result from either pathological or non-pathological causes. They can present as single or multiple defects, varying in shape, size, and margins (2, 3, 5, 7).
The most common pathological causes of intracavitary filling defects include endometrial polyps, intracavitary leiomyomas, endometrial hyperplasia, and synechiae (2, 3). Conversely, non-pathological causes may be artifacts such as air bubbles, mucus plugs, or normal anatomical variations that mimic filling defects, such as myometrial folds (8). Distinguishing pathological from non-pathological filling defects on HSG is often possible by assessing their shape, location, and impact on the uterine cavity contour. While these features aid in differential diagnosis, definitive confirmation often requires further evaluation through additional imaging modalities, such as ultrasound, MRI, or hysteroscopy.
Differential diagnosis relies on the characteristic features of pathological filling defects on HSG:
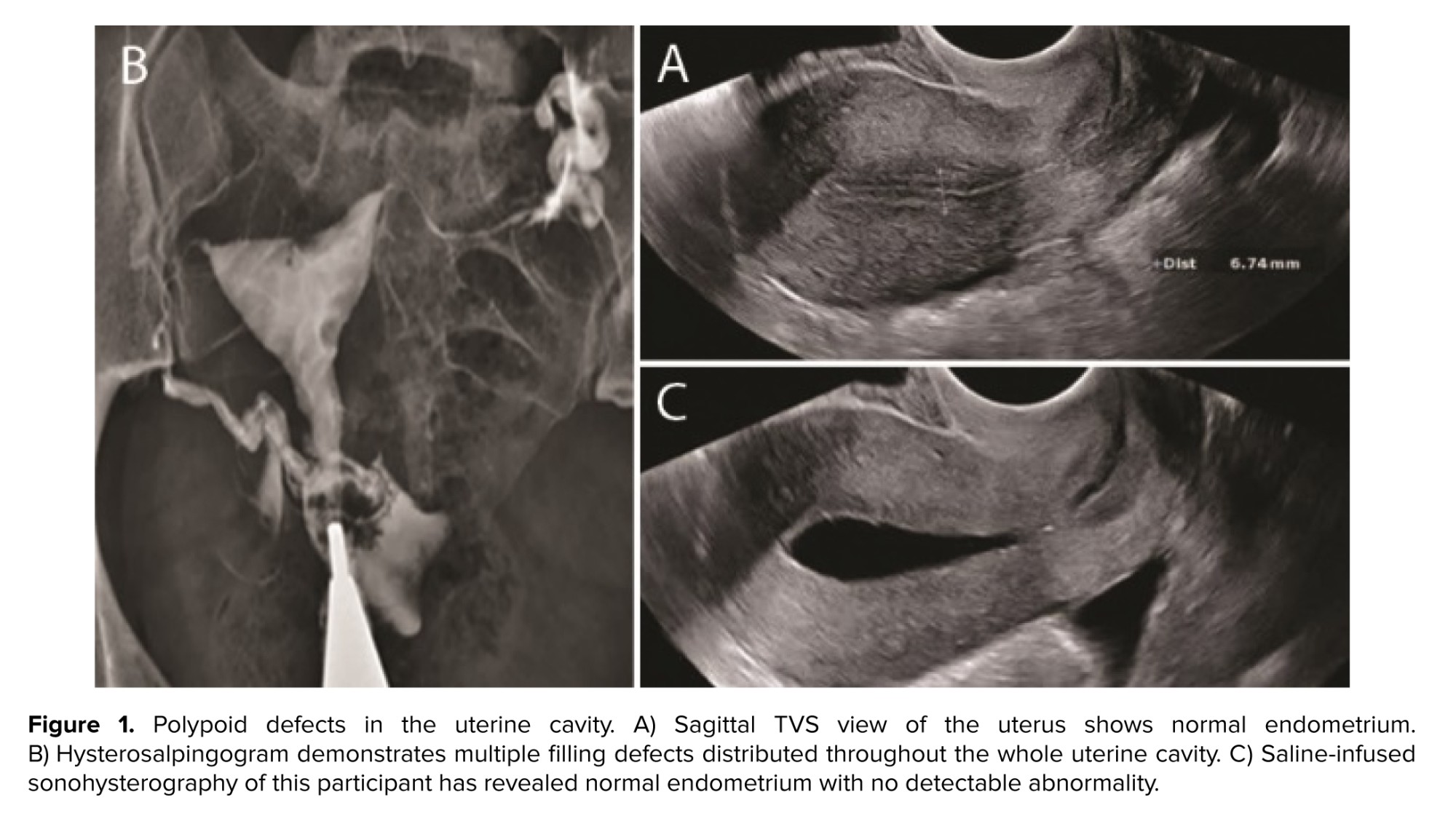
Endometrial polyps: these are usually benign and may cause abnormal uterine bleeding. On HSG, polyps appear as round filling defects, which are regular and sharply outlined. They are typically solitary but may occasionally be in multiple. Unlike fibroids, polyps do not distort the uterine outline (2, 3, 9, 10) (Figure 2).
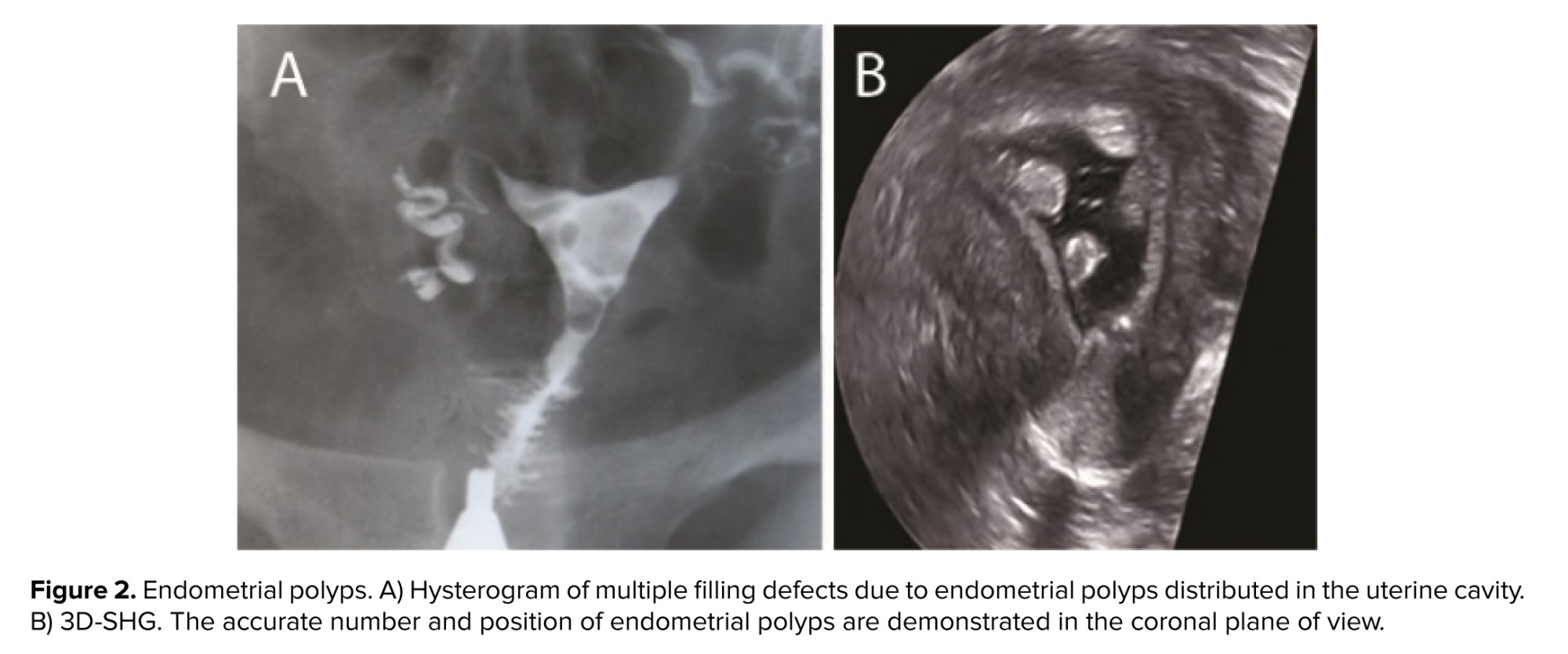
Fibroids (leiomyomas): leiomyomas are the most common benign uterine tumor. Leiomyomas are classified by location into intramural, subserosal, and submucosal. Submucosal leiomyoma is the least common but most often accounts for symptoms. This type can be seen as a smooth or irregular, single or multiple, small or large filling defect on HSG. Despite polyps, leiomyomas usually alter the uterine contour and size. Larger filling defects may be associated with enlargement and distortion of the endometrial cavity (2, 3, 9, 10) (Figure 3).
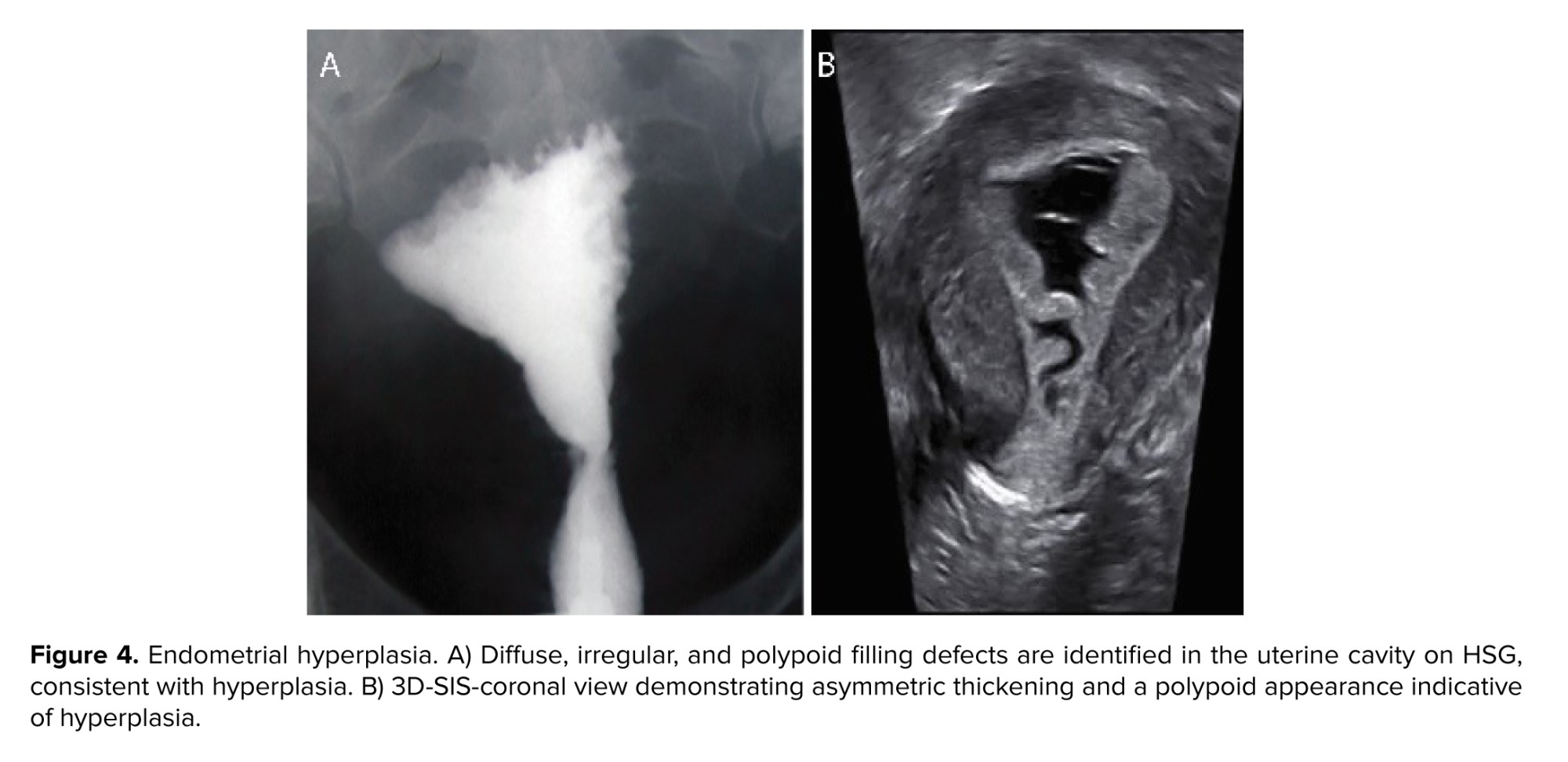
Endometrial hyperplasia: depending on the gross appearance of endometrial hyperplasia, the uterographic picture may show wide variations. With moderate thickening of the hyperplastic endometrium, some irregularity in the outline of the inner uterine surface is seen. When the endometrium is frankly polypoid, the uterine shadow shows variations in density, of which less dense areas correspond to polypoid projections (10) (Figure 4).
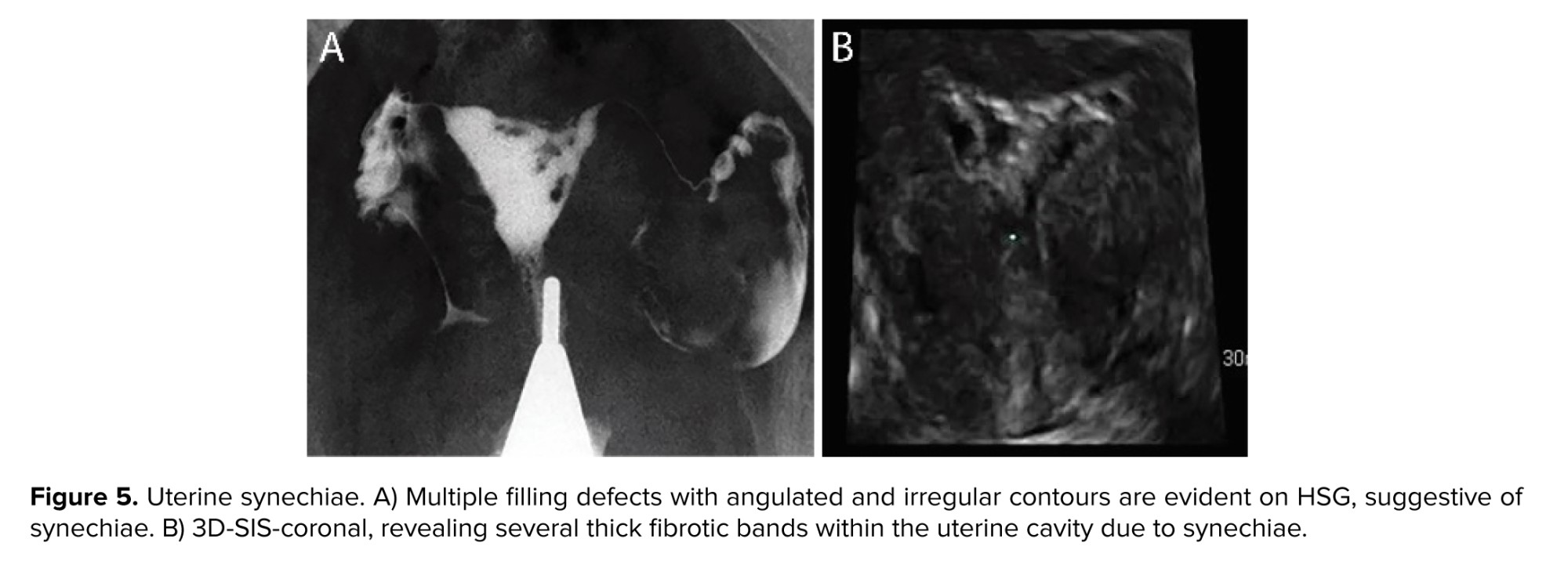
Synechiae (intrauterine adhesions): destruction of the endometrium may result in scarring and development of fibrotic bands within the uterine cavity, which appear as filling defects that distort the contour of the uterine cavity. They can make various appearances according to their location and the severity of scarring. They typically have an irregular, angulated shape and are immobile (2, 3, 9-11) (Figure 5).
Nonpathological filling defects are typically transient and well-defined and do not cause significant changes to the uterine structure. Common causes include:
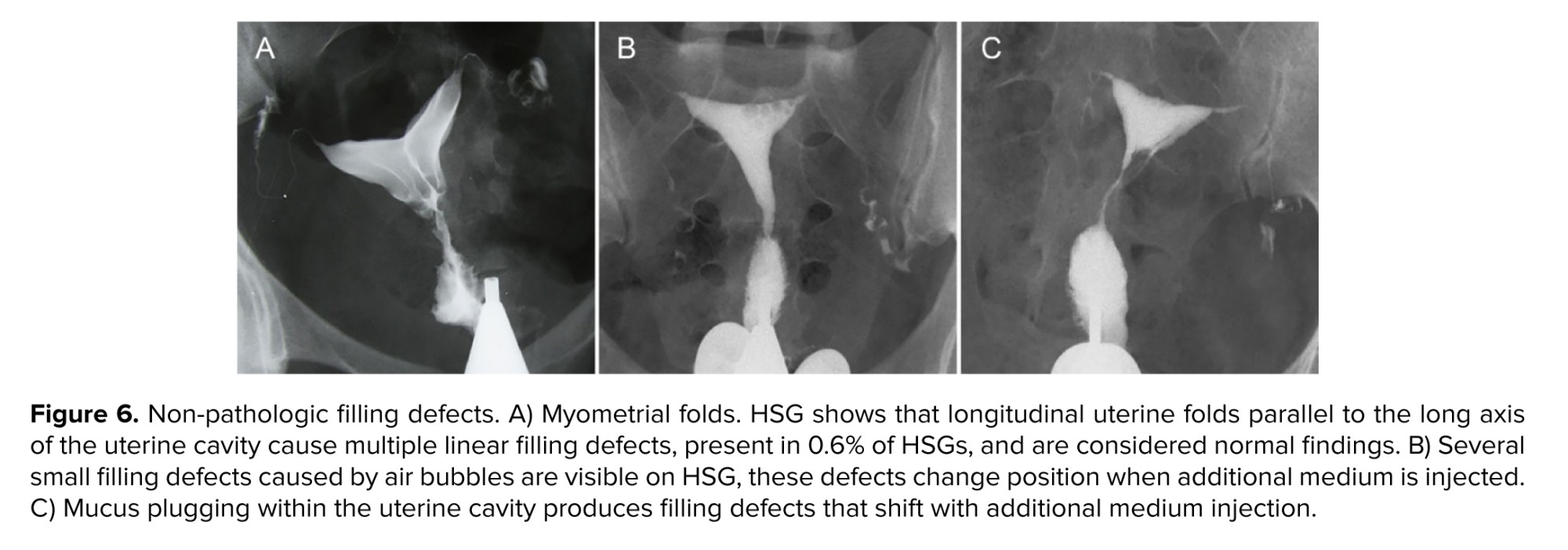
Myometrial folds: once myometrial folds are prominent, they may create linear filling defects and are considered normal anatomical variations. They can appear as broad, longitudinal ridges parallel to the uterine cavity, especially in early underfilled views of the uterus (3, 8, 10) (Figure 6).
Air bubbles: the incidental introduction of air during HSG can produce round or oval-shaped, well-defined filling defects. These are often mobile and may be single or multiple, sometimes mistaken for pathological lesions. Repositioning the participant or aspiration and refilling the uterine cavity resolves problems with air bubbles (2, 3, 8, 10) (Figure 6).
Cervical mucus: thick cervical mucus may appear as an irregularly bordered filling defect on HSG. Unlike true pathological defects, these artifacts tend to resolve upon further imaging (8, 10) (Figure 6).
Familiarity with nonpathological filling defects is crucial for radiologists to avoid misdiagnoses and unnecessary additional investigations.
Herein, we present a rare normal variation case in which normal endometrium can mimic multiple filling defects on HSG. These filling defects resemble the defects caused by multiple small submucous leiomyomas or polyps. Further endometrial investigation using diagnostic methods such as sonohysterography and hysteroscopy reveals no specific abnormality for this type. The cause of this phenomenon remains unclear, but it is thought to represent physiological changes during the menstrual cycle. No difference was found in the prevalence of these polypoid defects between the secretory and proliferative phases, and no correlation with the presence of uterine bleeding or other clinical symptoms (12). Subclinical scarring and transient myometrial contractions have also been suggested as potential contributors. Some minor intrauterine scars may not be detectable on ultrasound or hysteroscopy but can still be present as fine filling defects on HSG (11, 13). Uterine peristalsis or transient spasms during the procedure may momentarily alter the shape of the cavity, creating an apparent defect that disappears upon repeat imaging (14). To the best of our knowledge, this type of filling defect is not common and has been mentioned in a few studies (12). Only 4 similar cases of this type of normal variation were observed at our institute over the past 15 yr.
Upon identification of similar findings, precise documentation of participant’s clinical data and technical parameters related to this examination, combined with further investigation, application of transvaginal ultrasound or SIS (as accessible and non-invasive modalities) within a short interval following HSG, may effectively help to find the ambiguous etiologies underlying this imaging appearance and reduce the incidence of false-positive findings. Additionally, longitudinal follow-up of these patients to assess potential endometrial involvement may prove beneficial.
4. Conclusion
The radiologist's familiarity with pathological and nonpathological filling defects and their differential diagnosis reduces the risk of misdiagnosis and unnecessary interventions. Recognition of the distinguishing features of filling defects, such as shape, location, and the effects on the uterine cavity, allows for better differentiation between abnormalities and normal variations or artifacts. This recognition does not eliminate the need for further investigation but rather highlights the importance of complementary investigations with less invasive methods, such as SIS, to avoid misdiagnosis and unnecessary interventions.
Author Contributions
All authors meet the ICMJE authorship criteria. Study conception and design: F. Hosseini, F. Safi, and F. Ahmadi. Data collection: F. Hosseini, F. Safi, and F. Ahmadi. Data analysis and interpretation: F. Ahmadi and F. Safi. Drafting of the manuscript: F. Hosseini. Critical revision of the article: F. Ahmadi and F. Safi. Study supervision: F. Ahmadi. Final approval of the manuscript: F. Hosseini, F. Safi, and F. Ahmadi.
Acknowledgments
We appreciate the able assistance of our radiology technologists, Akram Pouyan, Leila Abedi, and Farahnaz Ghaderi. The study needed no financial support. The authors acknowledge the use of Google’s Gemini 1.5 Flash, an AI-assisted editing tool, to improve spelling, grammar, clarity, and readability during manuscript preparation. After using this tool, the authors carefully reviewed and edited the text and take full responsibility for the final content.
Conflict of Interest
The authors declare that there is no conflict of interest.
Hysterosalpingography (HSG) is one of the most widely used diagnostic tools for evaluating primary and secondary infertility. Despite the advent of advanced techniques, it remains the best non-surgical method for assessing the fallopian tubes. Routine evaluation of hysterosalpingograms also involves assessing the uterine cavity for any intrauterine abnormality. One of the most common abnormalities detected on HSG is a filling defect, which can represent a spectrum of intrauterine abnormalities, including submucosal fibroids, endometrial polyps, endometrial hyperplasia, synechiae, and, less frequently, nonpathological cases such as artifacts and normal variations. Uterine cavity abnormalities can cause single or multiple filling defects with regular or irregular margins (1-3). These abnormalities can significantly impact reproductive health, particularly in the context of infertility. In consequence, accurate differentiation between these entities is crucial for appropriate patient management. A definitive diagnosis requires further evaluation, such as saline infusion sonography (SIS), magnetic resonance imaging (MRI), or hysteroscopy.
However, further investigations might reveal that the uterine cavity is actually normal. This report presents a case of polypoid filling defects observed on HSG, where subsequent transvaginal sonography (TVS), SIS, and hysteroscopy revealed no underlying pathology. The broad spectrum of underlying pathologies make difficulties in diagnosis and interpretation of filling defects; therefore, further evaluation is crucial for accurate diagnosis and appropriate management.
2. Case Presentation
A 35-yr-old woman with primary infertility for 10 yr referred to Royan Institute, Tehran, Iran, and underwent HSG to evaluate tubal patency at our institution.
The participant denied a history of prior genital tract surgery. She did not have diabetes, hypertension, or thyroid dysfunction. She was a non-smoker with a body mass index of 28 and regular menstrual cycles. The participant’s medical record included blood test results with parameters within the normal range and a TVS report, which had been performed on day 7 of cycle, showing a normal endometrial thickness of 6 mm with a normal endometrial echo pattern and margins (Figure 1A).
The HSG performed on the participant revealed multiple filling defects throughout the uterine cavity, raising initial suspicion of polypoid hyperplasia or multiple polyps (Figure 1B). Further administration of the contrast agent induced no appreciable alteration in this HSG finding, excluding displacement of the filling defect attributed to an air bubble. The HSG showed normal findings in the fallopian tubes, with free spillage of contrast material into the peritoneal cavity. The participant was recommended for further evaluation. Next, SIS was performed, showing a normal endometrium with no evidence of polyps (Figure 1C).
Diagnostic hysteroscopy was subsequently undertaken and revealed no abnormalities. An endometrial biopsy was performed under direct hysteroscopic visualization, and the histopathology report confirmed the presence of normal endometrial tissue.
2.1. HSG protocol
A Shimadzu (Flexavision model) Dynamic Digital Radiography machine was used to perform this test. Using a cannula technique under fluoroscopic guidance, water-soluble contrast material (IODIXANOL-320) was slowly instilled into the uterus via the cervical canal in 3 stages. Each injection contained 2-3 cc of contrast material. After each injection, an image was acquired. The first image was obtained during early filling of the uterine cavity to evaluate for any filling defects or contour abnormalities; this stage is optimal for detecting small filling defects. The second image was acquired when the uterine cavity was fully distended, and the fallopian tubes were opacified. The third image was obtained to assess tubal patency. A fourth image was taken 20 min after the completion of the procedure to demonstrate the dispersion of contrast material within the peritoneal cavity.
2.2. SIS protocol
SIS was performed using a Samsung WS-80 ultrasound system and a 5-8 MHz transvaginal probe. Under aseptic conditions and ultrasound guidance, 5-10 cc of sterile saline solution was slowly injected into the uterine cavity through a Foley catheter (No. 8). The uterus was gradually distended, and as the uterine cavity filled with fluid, ultrasound images of the endometrium and uterine cavity were acquired and evaluated. The advantage of using saline as a negative contrast agent lies in its ability to create an echo-free background, which facilitates clear visualization of intrauterine abnormalities.
2.3. Ethical Considerations
Informed consent was obtained from the participant prior to the HSG exam. Their anonymity and confidentiality were ensured throughout the study.
3. Discussion
Imaging plays a major role in female infertility evaluation. Despite advanced imaging methods such as ultrasound, sonohysterography, and MRI, HSG remains one of the most frequently used methods to evaluate the uterine cavity and tubal patency (4, 5). In normal HSG, the uterine cavity is shown in an inverted triangular shape with no persistent filling defect and a well-defined smooth margin (1, 3, 5, 6).
Filling defects on HSG are areas where contrast dye fails to fill the uterine cavity. These defects are among the most frequently observed abnormalities on HSG and may result from either pathological or non-pathological causes. They can present as single or multiple defects, varying in shape, size, and margins (2, 3, 5, 7).
The most common pathological causes of intracavitary filling defects include endometrial polyps, intracavitary leiomyomas, endometrial hyperplasia, and synechiae (2, 3). Conversely, non-pathological causes may be artifacts such as air bubbles, mucus plugs, or normal anatomical variations that mimic filling defects, such as myometrial folds (8). Distinguishing pathological from non-pathological filling defects on HSG is often possible by assessing their shape, location, and impact on the uterine cavity contour. While these features aid in differential diagnosis, definitive confirmation often requires further evaluation through additional imaging modalities, such as ultrasound, MRI, or hysteroscopy.
Differential diagnosis relies on the characteristic features of pathological filling defects on HSG:
Endometrial polyps: these are usually benign and may cause abnormal uterine bleeding. On HSG, polyps appear as round filling defects, which are regular and sharply outlined. They are typically solitary but may occasionally be in multiple. Unlike fibroids, polyps do not distort the uterine outline (2, 3, 9, 10) (Figure 2).
Fibroids (leiomyomas): leiomyomas are the most common benign uterine tumor. Leiomyomas are classified by location into intramural, subserosal, and submucosal. Submucosal leiomyoma is the least common but most often accounts for symptoms. This type can be seen as a smooth or irregular, single or multiple, small or large filling defect on HSG. Despite polyps, leiomyomas usually alter the uterine contour and size. Larger filling defects may be associated with enlargement and distortion of the endometrial cavity (2, 3, 9, 10) (Figure 3).
Endometrial hyperplasia: depending on the gross appearance of endometrial hyperplasia, the uterographic picture may show wide variations. With moderate thickening of the hyperplastic endometrium, some irregularity in the outline of the inner uterine surface is seen. When the endometrium is frankly polypoid, the uterine shadow shows variations in density, of which less dense areas correspond to polypoid projections (10) (Figure 4).
Synechiae (intrauterine adhesions): destruction of the endometrium may result in scarring and development of fibrotic bands within the uterine cavity, which appear as filling defects that distort the contour of the uterine cavity. They can make various appearances according to their location and the severity of scarring. They typically have an irregular, angulated shape and are immobile (2, 3, 9-11) (Figure 5).
Nonpathological filling defects are typically transient and well-defined and do not cause significant changes to the uterine structure. Common causes include:
Myometrial folds: once myometrial folds are prominent, they may create linear filling defects and are considered normal anatomical variations. They can appear as broad, longitudinal ridges parallel to the uterine cavity, especially in early underfilled views of the uterus (3, 8, 10) (Figure 6).
Air bubbles: the incidental introduction of air during HSG can produce round or oval-shaped, well-defined filling defects. These are often mobile and may be single or multiple, sometimes mistaken for pathological lesions. Repositioning the participant or aspiration and refilling the uterine cavity resolves problems with air bubbles (2, 3, 8, 10) (Figure 6).
Cervical mucus: thick cervical mucus may appear as an irregularly bordered filling defect on HSG. Unlike true pathological defects, these artifacts tend to resolve upon further imaging (8, 10) (Figure 6).
Familiarity with nonpathological filling defects is crucial for radiologists to avoid misdiagnoses and unnecessary additional investigations.
Herein, we present a rare normal variation case in which normal endometrium can mimic multiple filling defects on HSG. These filling defects resemble the defects caused by multiple small submucous leiomyomas or polyps. Further endometrial investigation using diagnostic methods such as sonohysterography and hysteroscopy reveals no specific abnormality for this type. The cause of this phenomenon remains unclear, but it is thought to represent physiological changes during the menstrual cycle. No difference was found in the prevalence of these polypoid defects between the secretory and proliferative phases, and no correlation with the presence of uterine bleeding or other clinical symptoms (12). Subclinical scarring and transient myometrial contractions have also been suggested as potential contributors. Some minor intrauterine scars may not be detectable on ultrasound or hysteroscopy but can still be present as fine filling defects on HSG (11, 13). Uterine peristalsis or transient spasms during the procedure may momentarily alter the shape of the cavity, creating an apparent defect that disappears upon repeat imaging (14). To the best of our knowledge, this type of filling defect is not common and has been mentioned in a few studies (12). Only 4 similar cases of this type of normal variation were observed at our institute over the past 15 yr.
Upon identification of similar findings, precise documentation of participant’s clinical data and technical parameters related to this examination, combined with further investigation, application of transvaginal ultrasound or SIS (as accessible and non-invasive modalities) within a short interval following HSG, may effectively help to find the ambiguous etiologies underlying this imaging appearance and reduce the incidence of false-positive findings. Additionally, longitudinal follow-up of these patients to assess potential endometrial involvement may prove beneficial.
4. Conclusion
The radiologist's familiarity with pathological and nonpathological filling defects and their differential diagnosis reduces the risk of misdiagnosis and unnecessary interventions. Recognition of the distinguishing features of filling defects, such as shape, location, and the effects on the uterine cavity, allows for better differentiation between abnormalities and normal variations or artifacts. This recognition does not eliminate the need for further investigation but rather highlights the importance of complementary investigations with less invasive methods, such as SIS, to avoid misdiagnosis and unnecessary interventions.
Author Contributions
All authors meet the ICMJE authorship criteria. Study conception and design: F. Hosseini, F. Safi, and F. Ahmadi. Data collection: F. Hosseini, F. Safi, and F. Ahmadi. Data analysis and interpretation: F. Ahmadi and F. Safi. Drafting of the manuscript: F. Hosseini. Critical revision of the article: F. Ahmadi and F. Safi. Study supervision: F. Ahmadi. Final approval of the manuscript: F. Hosseini, F. Safi, and F. Ahmadi.
Acknowledgments
We appreciate the able assistance of our radiology technologists, Akram Pouyan, Leila Abedi, and Farahnaz Ghaderi. The study needed no financial support. The authors acknowledge the use of Google’s Gemini 1.5 Flash, an AI-assisted editing tool, to improve spelling, grammar, clarity, and readability during manuscript preparation. After using this tool, the authors carefully reviewed and edited the text and take full responsibility for the final content.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Case Report |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
