
International Journal of
Reproductive Biomedicine
Tue, Aug 4, 2026
[Archive]
Volume 24, Issue 3 (March 2026)
IJRM 2026, 24(3): 245-256 |
Back to browse issues page


Ethics code: IR.AJUMS.REC.1402.629
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bakhshipour F, Torabizadeh M, Jalali Far M A, Moramezi F, Saki N. Altered inflammatory and coagulation markers in women with a history of recurrent pregnancy loss: A case-control study. IJRM 2026; 24 (3) :245-256
URL: http://ijrm.ir/article-1-3688-en.html
URL: http://ijrm.ir/article-1-3688-en.html
Fatemeh Bakhshipour1 

 , Mehdi Torabizadeh2 , Mohammad Ali Jalali Far1 , Farideh Moramezi3 , Najmaldin Saki *4
, Mehdi Torabizadeh2 , Mohammad Ali Jalali Far1 , Farideh Moramezi3 , Najmaldin Saki *4
, Mehdi Torabizadeh2 , Mohammad Ali Jalali Far1 , Farideh Moramezi3 , Najmaldin Saki *4
1- Thalassemia and Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
2- Golestan Hospital Clinical Research Development Unit, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
3- Fertility, Infertility and Perinatology Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
4- Thalassemia and Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. ,najmaldinsaki@gmail.com; saki-nj@ajums.ac.ir
2- Golestan Hospital Clinical Research Development Unit, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
3- Fertility, Infertility and Perinatology Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
4- Thalassemia and Hemoglobinopathy Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. ,
Full-Text [PDF 553 kb]
(288 Downloads)
| Abstract (HTML) (352 Views)
Full-Text: (61 Views)
1. Introduction
Recurrent pregnancy loss (RPL) is characterized by 2 or more recurrent spontaneous miscarriages before 20 wk of gestation (1). About 3-5% of pregnant women worldwide have RPL, a clinically difficult condition with an unknown etiology in roughly 50% of cases (2-4). The etiopathogenesis of RPL is multifactorial, involving genetic, anatomical, hormonal, immunological, and hematological determinants. In recent years, scholarly attention has increasingly focused on the intricate interplay between inflammatory and coagulation pathways in the development of RPL (5-7).
Normal pregnancy requires a finely tuned equilibrium between procoagulant activity and natural anticoagulant mechanisms to maintain placental hemostasis. Disruption of this balance, particularly through deficiencies in natural anticoagulants such as protein C and protein S, has been implicated in placental thrombosis, which may contribute to early and late miscarriages, intrauterine growth restriction, and even intrauterine fetal demise (8, 9). Several studies have reported that women with RPL are more likely to exhibit reduced protein S levels, for example, Alshammary et al. demonstrated a significant relationship between protein S deficiency and recurrent miscarriage (10). More recent investigations have confirmed that diminished levels of both protein C and protein S are associated with unexplained RPL, underscoring the role of inherited thrombophilic defects in these cases (6, 11).
Concurrently, an emerging body of evidence highlights the fact that inflammatory processes could exacerbate these coagulation abnormalities. Inflammatory cytokines, notably interleukin-6 and tumor necrosis factor-α, can downregulate the protein C pathway by impairing the expression of endothelial anticoagulant molecules such as thrombomodulin and the endothelial protein C receptor (12). Recent reviews have described how inflammatory mediators may decrease the levels of free protein S on endothelial surfaces, thereby promoting a prothrombotic state (13). Among inflammatory biomarkers, calprotectin (leukocyte L1 antigen complex), namely a calcium-binding heterodimer classified as an acute-phase protein, has garnered interest due to its sensitivity in detecting residual inflammation, which often surpasses the sensitivity of C-reactive protein (CRP) (14). Recent systematic reviews and prospective cohort studies in pregnancy-associated diseases support the potential role of calprotectin as a biomarker for monitoring inflammatory status in cases with RPL (15).
Thus, the concurrent evaluation of inflammatory markers (such as calprotectin) and natural anticoagulant proteins (proteins C and S) may offer valuable insights into the mechanisms through which inflammation interferes with placental vascular integrity. A better understanding of these interactions is critical for identifying women at risk for RPL in order to develop targeted therapeutic interventions aimed at restoring the balance between coagulation and inflammation.
2. Materials and Methods
Normal pregnancy requires a finely tuned equilibrium between procoagulant activity and natural anticoagulant mechanisms to maintain placental hemostasis. Disruption of this balance, particularly through deficiencies in natural anticoagulants such as protein C and protein S, has been implicated in placental thrombosis, which may contribute to early and late miscarriages, intrauterine growth restriction, and even intrauterine fetal demise (8, 9). Several studies have reported that women with RPL are more likely to exhibit reduced protein S levels, for example, Alshammary et al. demonstrated a significant relationship between protein S deficiency and recurrent miscarriage (10). More recent investigations have confirmed that diminished levels of both protein C and protein S are associated with unexplained RPL, underscoring the role of inherited thrombophilic defects in these cases (6, 11).
Concurrently, an emerging body of evidence highlights the fact that inflammatory processes could exacerbate these coagulation abnormalities. Inflammatory cytokines, notably interleukin-6 and tumor necrosis factor-α, can downregulate the protein C pathway by impairing the expression of endothelial anticoagulant molecules such as thrombomodulin and the endothelial protein C receptor (12). Recent reviews have described how inflammatory mediators may decrease the levels of free protein S on endothelial surfaces, thereby promoting a prothrombotic state (13). Among inflammatory biomarkers, calprotectin (leukocyte L1 antigen complex), namely a calcium-binding heterodimer classified as an acute-phase protein, has garnered interest due to its sensitivity in detecting residual inflammation, which often surpasses the sensitivity of C-reactive protein (CRP) (14). Recent systematic reviews and prospective cohort studies in pregnancy-associated diseases support the potential role of calprotectin as a biomarker for monitoring inflammatory status in cases with RPL (15).
Thus, the concurrent evaluation of inflammatory markers (such as calprotectin) and natural anticoagulant proteins (proteins C and S) may offer valuable insights into the mechanisms through which inflammation interferes with placental vascular integrity. A better understanding of these interactions is critical for identifying women at risk for RPL in order to develop targeted therapeutic interventions aimed at restoring the balance between coagulation and inflammation.
2. Materials and Methods
2.1. Study design and participants
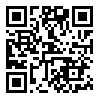
In this case-control study, a total of 100 women aged between 18 and 45 yr admitted at Golestan hospital, Ahvaz, Iran from February 2024 to January 2025 were enrolled.
Participants were divided into 2 groups based on their reproductive history: a case group of women with RPL (n = 50), which was defined as ≥ 2 spontaneous abortions without chromosomal, anatomical, or hormonal defects, and a control group of women with no history of infertility or miscarriage and at least one full-term delivery (n = 50).
2.2. Eligibility criteria
In this case-control study, a total of 100 women aged between 18 and 45 yr admitted at Golestan hospital, Ahvaz, Iran from February 2024 to January 2025 were enrolled.
Participants were divided into 2 groups based on their reproductive history: a case group of women with RPL (n = 50), which was defined as ≥ 2 spontaneous abortions without chromosomal, anatomical, or hormonal defects, and a control group of women with no history of infertility or miscarriage and at least one full-term delivery (n = 50).
2.2. Eligibility criteria
Only women aged 18-45 yr presenting with a history of ≥ 2 consecutive miscarriages with the last pregnancy loss at least 6 months previously were selected. Participants proven to be pregnant or currently receiving warfarin, oral contraceptives, other anticoagulants, or hormonal therapy were excluded from this study.
All women were clinically examined by an obstetrician and gynecologist. Uterine malformations were evaluated by transvaginal ultrasonography, and when needed, 3-dimensional ultrasonography or hysteroscopy was conducted to verify the normalcy of the uterus. Pregnant women with congenital uterine anomalies, fibroids in the uterine cavity, or intrauterine adhesions were not accepted into the study. Parental karyotyping was available for all patients, and no chromosomal abnormalities were identified.
Control subjects were matched for age and ethnicity, having at least one naturally conceived child with no miscarriage or complications in pregnancy.
Participants suffering from autoimmune disorders, thrombophilia, chronic inflammatory diseases, recent infection, or the use of immunosuppressive or anti-inflammatory drugs were excluded.
2.3. Sample collection
A blood sample (5 ml) was collected from each participant in the morning after an overnight fast. Venous blood was drawn from the brachial vein of the left arm at the respective infertility center. Samples were processed within 2 hr of collection and subsequently stored at -80°C until analysis to ensure sample integrity.
2.4. Technical information
Serum concentrations of calprotectin were determined using the CalproLab enzyme-linked immunosorbent assay (Horseradish Peroxidase™ kit from Calpro AS., Norway). Protein C and protein S levels were measured using the CHROMOGENIC PROTEIN C kit™ and the Clotting Protein S kit™, respectively, both manufactured by Sclavo Diagnostics International SpA (Italy). All assays were performed in duplicate, and standard curves were plotted for each assay using known concentrations of the respective analytes. Internal quality controls were included in each assay run, and equipment calibration was conducted in accordance with manufacturers' instructions to ensure accuracy and precision. In addition, complete blood counts (CBC) were performed using the KX-21N hematology analyzer (Sysmex). Anemia was defined as a hemoglobin (Hb) level < 12 mmol/L according to World Health Organization standards and was further categorized by mean corpuscular volume (MCV) into microcytic (MCV < 80 fL), normocytic (80 fL ≤ MCV ≤ 100 fL), and macrocytic (MCV > 100 fL) types.
2.5. Sample size
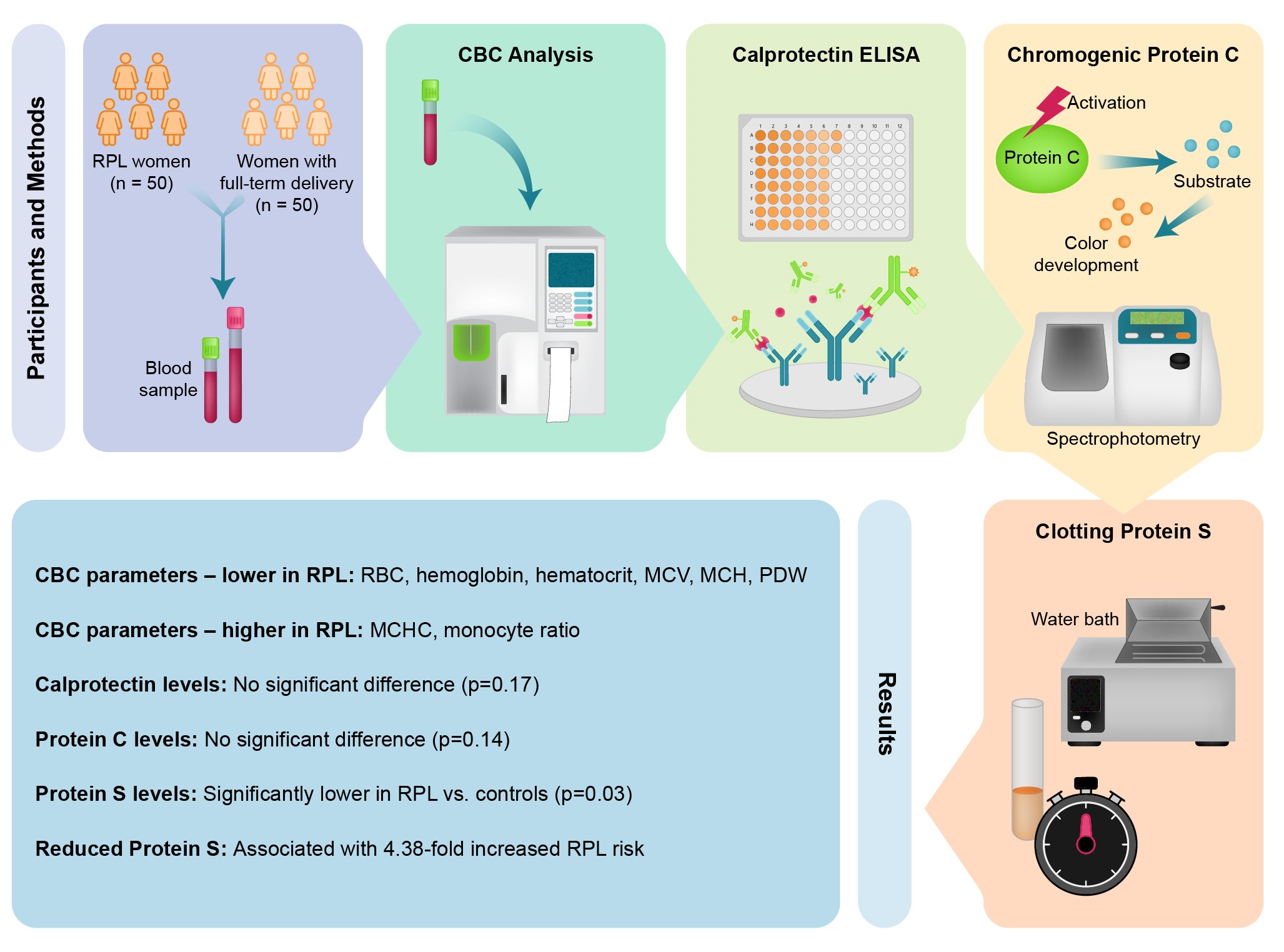
The minimum sample size per group was calculated to detect the difference in mean serum C-protein levels between cases with RPL and healthy controls with 80% test power at a significance level of α = 0.05.
Assuming that the case group has an equal standard deviation as the control group, σ = 17.57 has been reported as the standard deviation of the control group in a previous study (11).
We managed to detect a mean difference of 10.4 using the following formula for comparing 2 independent groups:
Anticipating up to 10% loss of follow-up, we inflated the per group size to 50, leading to a total of 100 participants (50 RPL and 50 control).
2.6. Ethical Considerations
This study was approved by the ethics committee of Jundishapur University of Medical Sciences, Ahvaz, Iran (Code: IR.AJUMS.REC.1402.629). All procedures adhered to the principles of the 1964 Helsinki Declaration. Prior to participation, the objectives and protocols of the study were thoroughly explained, and written informed consent was obtained from all participants.
2.7. Statistical Analysis
Quantitative variables (including protein C, protein S, calprotectin, etc.) were reported as mean ± standard deviation, as well as median and interquartile range. The normality of these variables was assessed using the Shapiro-Wilk test. To compare quantitative variables between the case and control groups, an independent t test or Mann-Whitney U test was applied, depending on the distribution of the data. In addition, a logistic regression model was performed.
A p < 0.05 was considered statistically significant. All statistical analyses were conducted using Statistical Package for the Social Sciences software, version 20.
3. Results
All women were clinically examined by an obstetrician and gynecologist. Uterine malformations were evaluated by transvaginal ultrasonography, and when needed, 3-dimensional ultrasonography or hysteroscopy was conducted to verify the normalcy of the uterus. Pregnant women with congenital uterine anomalies, fibroids in the uterine cavity, or intrauterine adhesions were not accepted into the study. Parental karyotyping was available for all patients, and no chromosomal abnormalities were identified.
Control subjects were matched for age and ethnicity, having at least one naturally conceived child with no miscarriage or complications in pregnancy.
Participants suffering from autoimmune disorders, thrombophilia, chronic inflammatory diseases, recent infection, or the use of immunosuppressive or anti-inflammatory drugs were excluded.
2.3. Sample collection
A blood sample (5 ml) was collected from each participant in the morning after an overnight fast. Venous blood was drawn from the brachial vein of the left arm at the respective infertility center. Samples were processed within 2 hr of collection and subsequently stored at -80°C until analysis to ensure sample integrity.
2.4. Technical information
Serum concentrations of calprotectin were determined using the CalproLab enzyme-linked immunosorbent assay (Horseradish Peroxidase™ kit from Calpro AS., Norway). Protein C and protein S levels were measured using the CHROMOGENIC PROTEIN C kit™ and the Clotting Protein S kit™, respectively, both manufactured by Sclavo Diagnostics International SpA (Italy). All assays were performed in duplicate, and standard curves were plotted for each assay using known concentrations of the respective analytes. Internal quality controls were included in each assay run, and equipment calibration was conducted in accordance with manufacturers' instructions to ensure accuracy and precision. In addition, complete blood counts (CBC) were performed using the KX-21N hematology analyzer (Sysmex). Anemia was defined as a hemoglobin (Hb) level < 12 mmol/L according to World Health Organization standards and was further categorized by mean corpuscular volume (MCV) into microcytic (MCV < 80 fL), normocytic (80 fL ≤ MCV ≤ 100 fL), and macrocytic (MCV > 100 fL) types.
2.5. Sample size
The minimum sample size per group was calculated to detect the difference in mean serum C-protein levels between cases with RPL and healthy controls with 80% test power at a significance level of α = 0.05.
Assuming that the case group has an equal standard deviation as the control group, σ = 17.57 has been reported as the standard deviation of the control group in a previous study (11).
We managed to detect a mean difference of 10.4 using the following formula for comparing 2 independent groups:
Anticipating up to 10% loss of follow-up, we inflated the per group size to 50, leading to a total of 100 participants (50 RPL and 50 control).
2.6. Ethical Considerations
This study was approved by the ethics committee of Jundishapur University of Medical Sciences, Ahvaz, Iran (Code: IR.AJUMS.REC.1402.629). All procedures adhered to the principles of the 1964 Helsinki Declaration. Prior to participation, the objectives and protocols of the study were thoroughly explained, and written informed consent was obtained from all participants.
2.7. Statistical Analysis
Quantitative variables (including protein C, protein S, calprotectin, etc.) were reported as mean ± standard deviation, as well as median and interquartile range. The normality of these variables was assessed using the Shapiro-Wilk test. To compare quantitative variables between the case and control groups, an independent t test or Mann-Whitney U test was applied, depending on the distribution of the data. In addition, a logistic regression model was performed.
A p < 0.05 was considered statistically significant. All statistical analyses were conducted using Statistical Package for the Social Sciences software, version 20.
3. Results
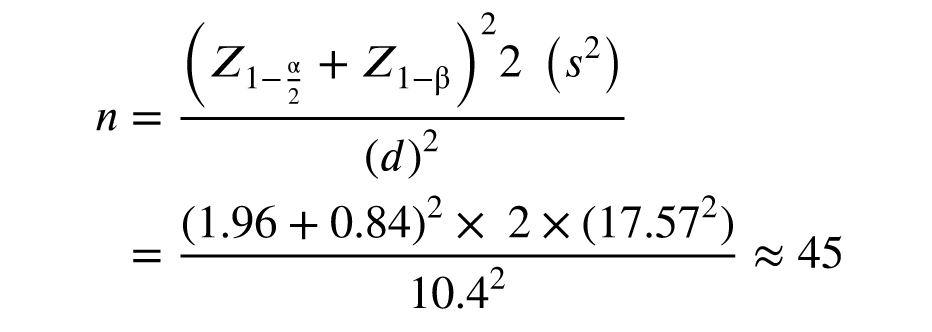
In total, 100 women participated in our study. The mean age of participants in the RPL group was 35.62 ± 5.59 yr, compared with 34.00 ± 6.45 yr in the control group; no statistically significant difference was observed between the 2 groups (p = 0.205). After enrollment and initial assessments, blood tests were performed. The findings are summarized in table I.
3.1. Serum levels of protein S, protein C, and calprotectin
The analysis of coagulation and inflammatory markers revealed that the mean protein S level was significantly lower in the RPL group (66.05 ± 25.36%) compared with the control group (78.28 ± 17.41%, p = 0.03). For greater accuracy in interpreting the results, in addition to reporting the mean protein S level, the proportion of individuals with subnormal levels was also presented. In the RPL group, 18 participants (36%) had protein S levels below 60%, whereas control group had 6 participants (12%) (p = 0.01).
In contrast, although the mean levels of protein C (RPL: 91.74 ± 16.74% vs. control: 97.12 ± 19.76%, p = 0.14) and calprotectin (RPL: 72.47 ± 66.99 ng/ml vs. control: 85.29 ± 76.16 ng/ml, p = 0.17) were lower in the RPL group, the differences did not reach statistical significance.
3.2. CBC findings
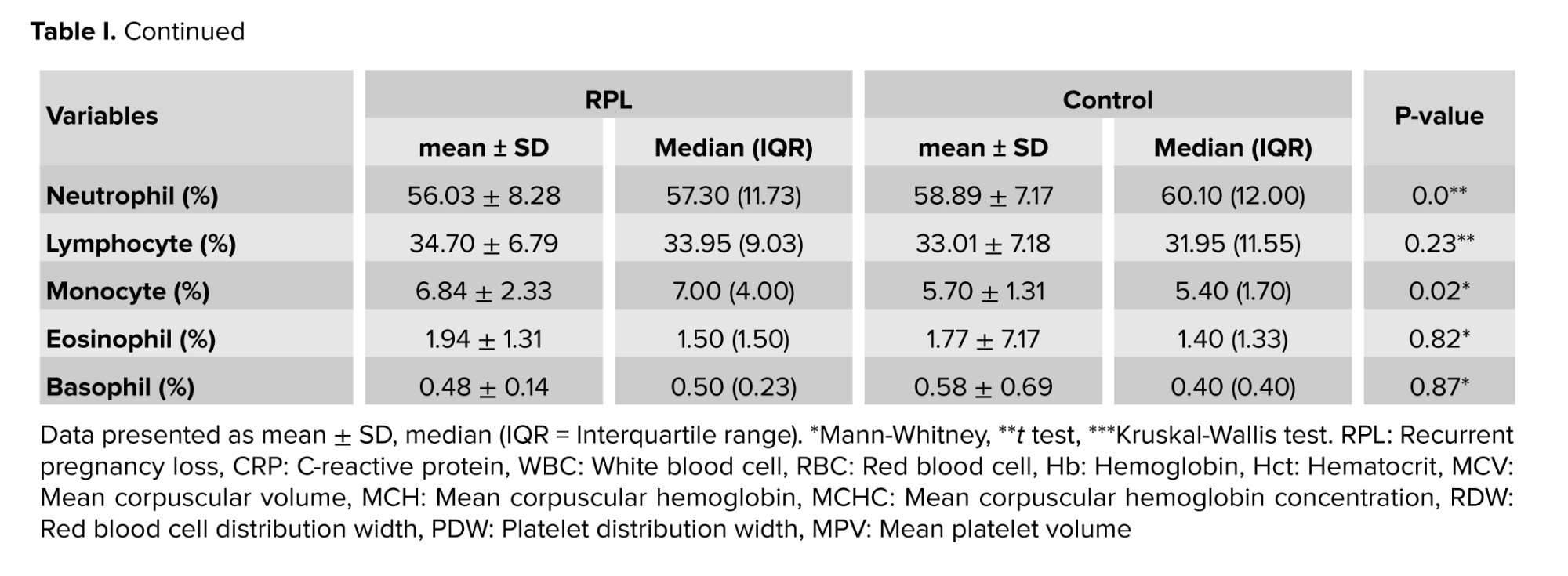
The CBC parameters indicated that the RPL group exhibited significantly lower mean values of red blood cells (RBC), Hb, hematocrit (Hct), MCV, mean corpuscular hemoglobin (MCH), and platelet distribution width compared with the control group. Conversely, the levels of CRP, mean corpuscular hemoglobin concentration (MCHC), and monocyte ratio were significantly higher in the RPL group.
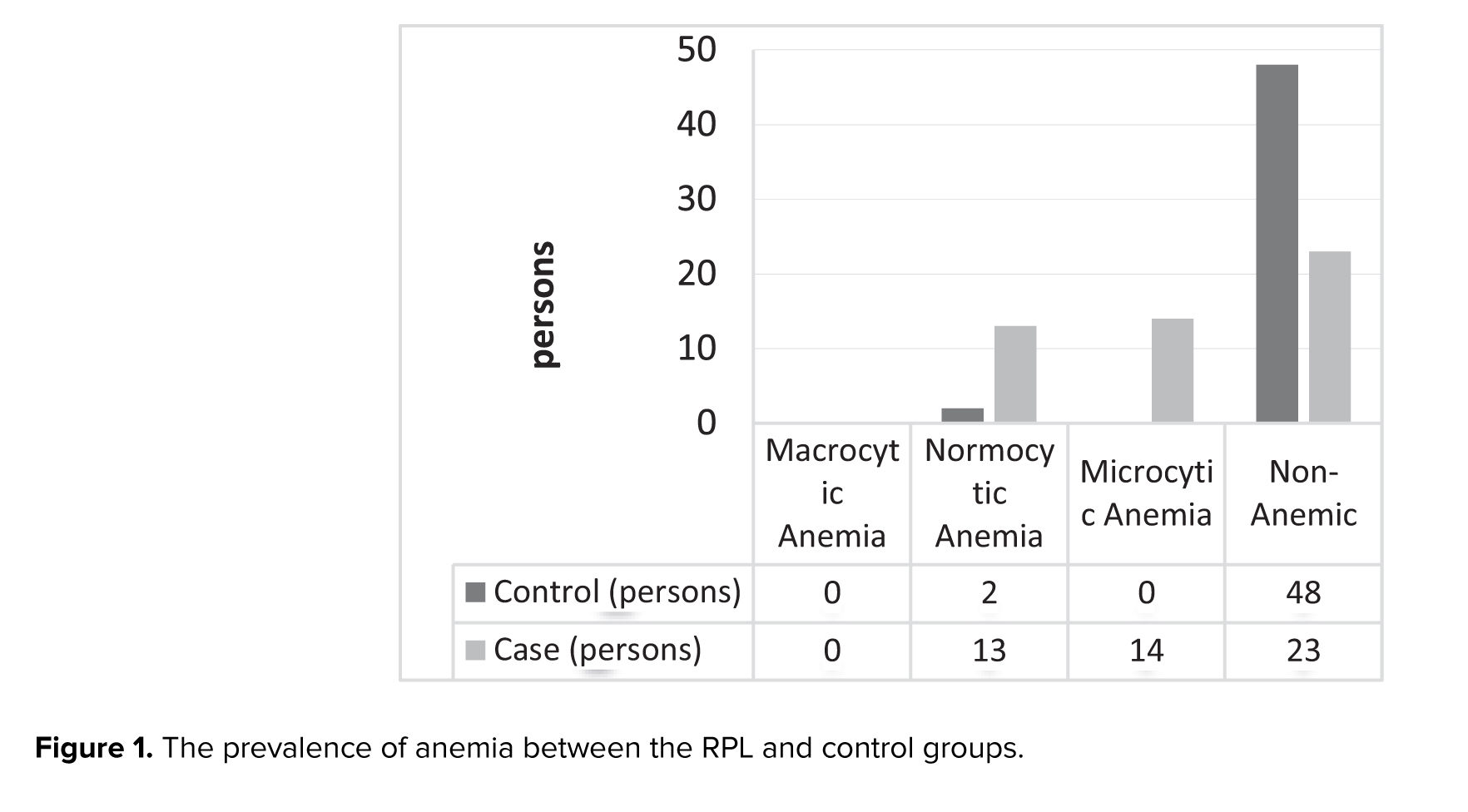
In total, 29 participants were diagnosed with anemia, and the status of anemia in the 2 groups is illustrated in figure 1. The difference in the prevalence of anemia between the RPL group and the control group was statistically significant (p < 0.001).
Table I presents the detailed laboratory parameters for both groups. In total, 29 participants were diagnosed with anemia. As shown in figure 1, the prevalence of anemia was significantly greater in the RPL group than in the control group (p < 0.001).
3.3. Receiver operating characteristic curve analysis of protein S
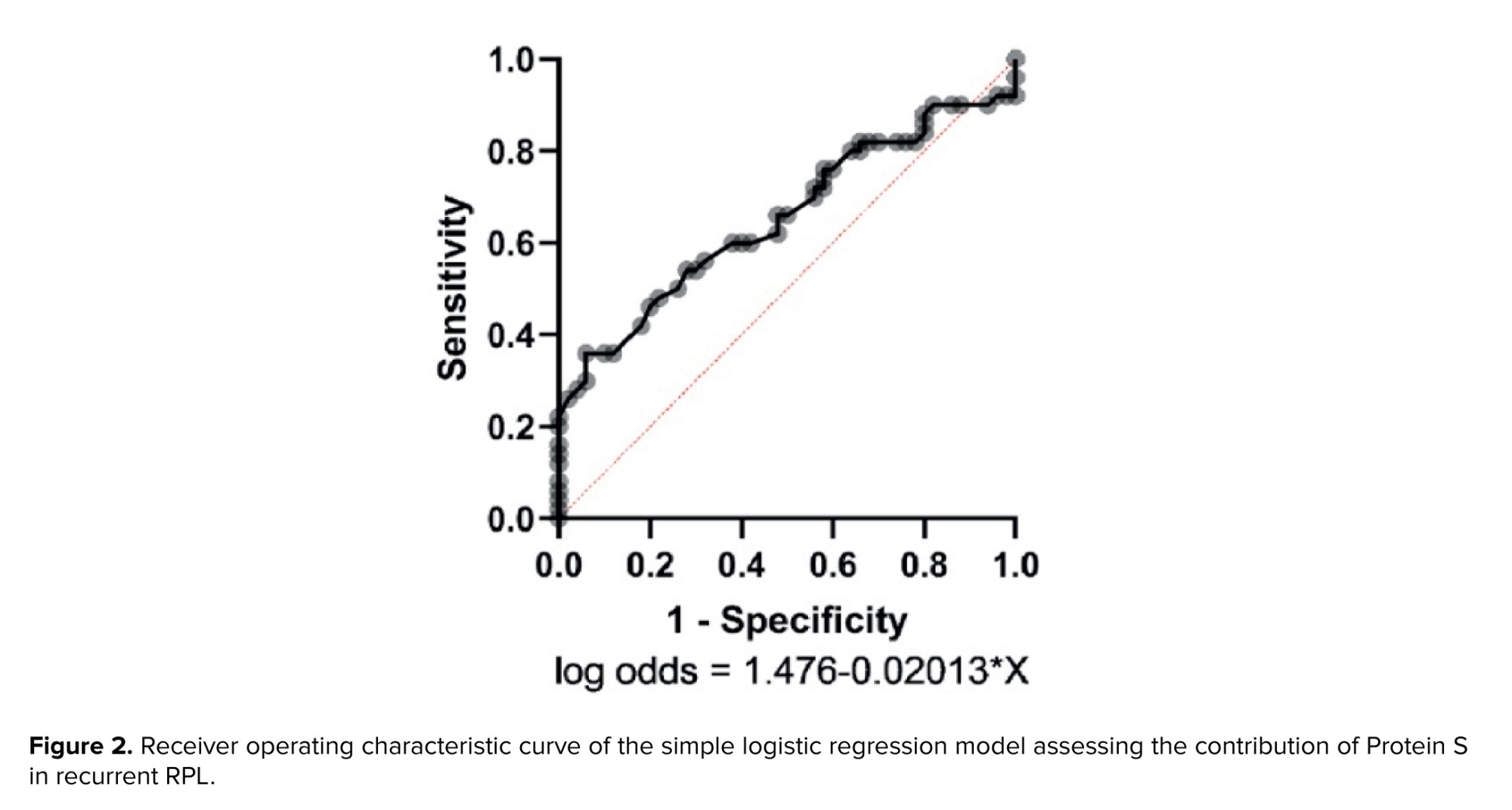
To further investigate the association between protein S levels and RPL, a logistic regression analysis was performed. This analysis revealed that the decrease in protein S levels was associated with a 4.38-fold increase in the risk of RPL (odds ratio [OR] = 4.376, Z = 2.074, p = 0.0309; Figure 2). Furthermore, the threshold protein S level corresponding to a 50% risk was determined to be 73.33 ± 10.17, suggesting that levels < 60% markedly elevate the likelihood of RPL.
3.4. Multivariable logistic regression analysis of protein S
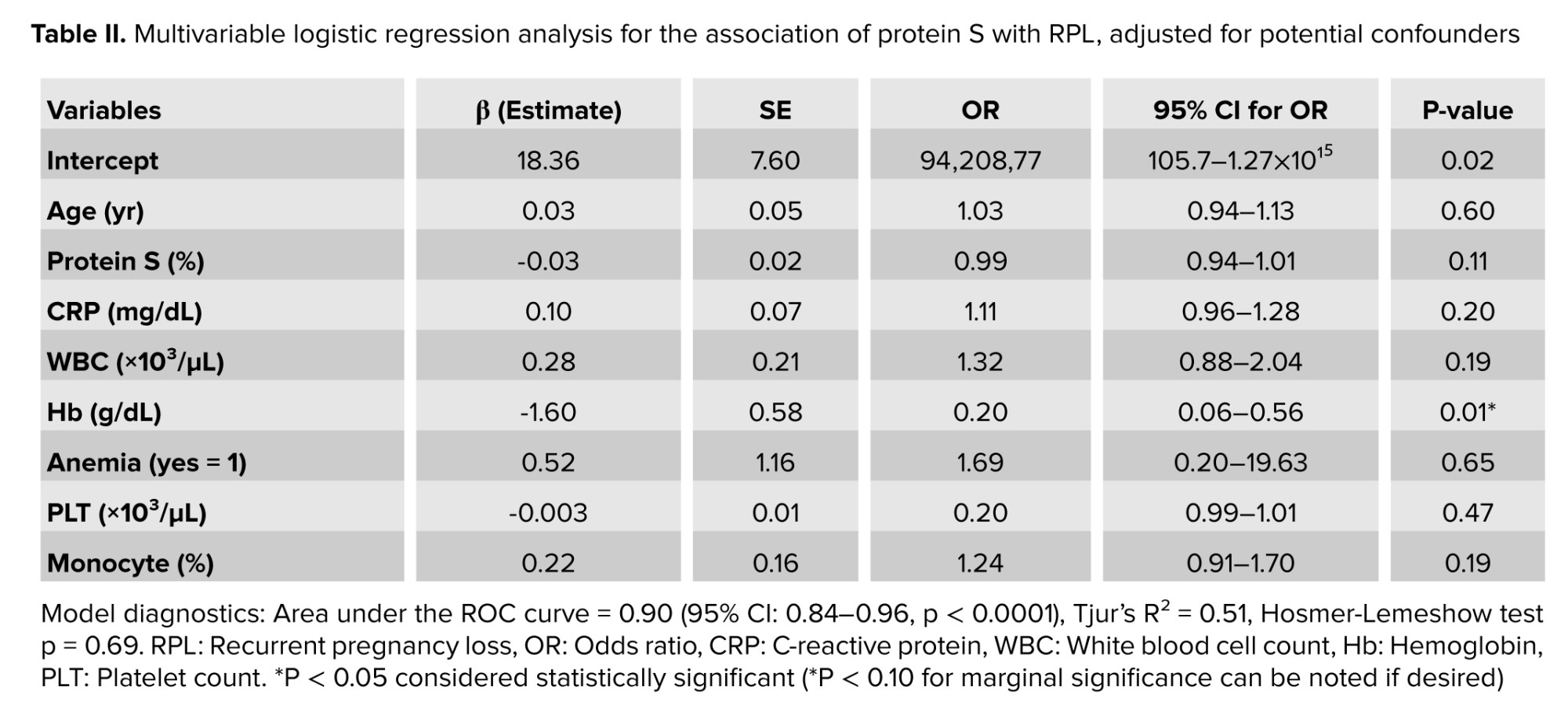
Multivariable logistic regression analysis was performed to evaluate the independent associations of protein S with RPL cases, while adjusting for potential confounders. The following covariates were included in all models: age, CRP, white blood cell (WBC), monocyte, Hb, anemia (yes = 1), and platelet count (PLT).
These covariates were selected because they exhibited significant or borderline significant differences (p < 0.20) between the RPL and control groups in univariable analyses (Table I) and are recognized in the literature as potential confounders in studies of RPL, given their associations with inflammation, hematological status, thrombotic risk, and the outcome of interest.
To minimize multicollinearity and avoid overfitting, highly correlated hematological parameters (e.g., RBC, Hct, MCV, MCH, MCHC) were excluded, with Hb and anemia retained as representative indicators of anemia status. Among differential WBC counts, only monocyte percentage (which showed a significant univariable difference) and total WBC were included. PLT was retained due to its strong univariable association, whereas related variables (mean platelet volume [MPV] and platelet distribution width) were omitted owing to high correlation with PLT. The number of independent variables was limited to 8 per model (plus the primary variable) to maintain an acceptable events-per-variable ratio (approximately 5.6) and reduce the risk of overfitting.
Model fit was assessed using the area under the receiver operating characteristic curve, Tjur’s R², and the Hosmer-Lemeshow goodness-of-fit test. P < 0.05 was considered statistically significant.
Protein S levels were initially evaluated using a clinically established cutoff of < 60% (a threshold commonly used to define mild deficiency in non-pregnant women of reproductive age). In univariable logistic regression, protein S levels below 60% were significantly associated with an increased risk of RPL (unadjusted OR = 4.38, p = 0.03), indicating that individuals with levels in this range had over 4 times the odds of RPL compared to those with levels ≥ 60%.
To fully utilize the continuous nature of the data and avoid potential loss of information associated with dichotomization, protein S was subsequently modeled as a continuous variable in multivariable logistic regression. After adjusting for potential confounders (age, CRP, WBC, Hb, anemia, PLT, and monocyte percentage), each 1% decrease in protein S level was associated with a marginally higher risk of RPL (adjusted OR = 0.98, 95% CI: 0.94-1.01, p = 0.11; Table II). The attenuation of the association in the multivariable model suggests that part of the crude effect observed with the dichotomous approach may be explained by confounding factors, particularly anemia and inflammatory markers.
4. Discussion
3.1. Serum levels of protein S, protein C, and calprotectin
The analysis of coagulation and inflammatory markers revealed that the mean protein S level was significantly lower in the RPL group (66.05 ± 25.36%) compared with the control group (78.28 ± 17.41%, p = 0.03). For greater accuracy in interpreting the results, in addition to reporting the mean protein S level, the proportion of individuals with subnormal levels was also presented. In the RPL group, 18 participants (36%) had protein S levels below 60%, whereas control group had 6 participants (12%) (p = 0.01).
In contrast, although the mean levels of protein C (RPL: 91.74 ± 16.74% vs. control: 97.12 ± 19.76%, p = 0.14) and calprotectin (RPL: 72.47 ± 66.99 ng/ml vs. control: 85.29 ± 76.16 ng/ml, p = 0.17) were lower in the RPL group, the differences did not reach statistical significance.
3.2. CBC findings
The CBC parameters indicated that the RPL group exhibited significantly lower mean values of red blood cells (RBC), Hb, hematocrit (Hct), MCV, mean corpuscular hemoglobin (MCH), and platelet distribution width compared with the control group. Conversely, the levels of CRP, mean corpuscular hemoglobin concentration (MCHC), and monocyte ratio were significantly higher in the RPL group.
In total, 29 participants were diagnosed with anemia, and the status of anemia in the 2 groups is illustrated in figure 1. The difference in the prevalence of anemia between the RPL group and the control group was statistically significant (p < 0.001).
Table I presents the detailed laboratory parameters for both groups. In total, 29 participants were diagnosed with anemia. As shown in figure 1, the prevalence of anemia was significantly greater in the RPL group than in the control group (p < 0.001).
3.3. Receiver operating characteristic curve analysis of protein S
To further investigate the association between protein S levels and RPL, a logistic regression analysis was performed. This analysis revealed that the decrease in protein S levels was associated with a 4.38-fold increase in the risk of RPL (odds ratio [OR] = 4.376, Z = 2.074, p = 0.0309; Figure 2). Furthermore, the threshold protein S level corresponding to a 50% risk was determined to be 73.33 ± 10.17, suggesting that levels < 60% markedly elevate the likelihood of RPL.
3.4. Multivariable logistic regression analysis of protein S
Multivariable logistic regression analysis was performed to evaluate the independent associations of protein S with RPL cases, while adjusting for potential confounders. The following covariates were included in all models: age, CRP, white blood cell (WBC), monocyte, Hb, anemia (yes = 1), and platelet count (PLT).
These covariates were selected because they exhibited significant or borderline significant differences (p < 0.20) between the RPL and control groups in univariable analyses (Table I) and are recognized in the literature as potential confounders in studies of RPL, given their associations with inflammation, hematological status, thrombotic risk, and the outcome of interest.
To minimize multicollinearity and avoid overfitting, highly correlated hematological parameters (e.g., RBC, Hct, MCV, MCH, MCHC) were excluded, with Hb and anemia retained as representative indicators of anemia status. Among differential WBC counts, only monocyte percentage (which showed a significant univariable difference) and total WBC were included. PLT was retained due to its strong univariable association, whereas related variables (mean platelet volume [MPV] and platelet distribution width) were omitted owing to high correlation with PLT. The number of independent variables was limited to 8 per model (plus the primary variable) to maintain an acceptable events-per-variable ratio (approximately 5.6) and reduce the risk of overfitting.
Model fit was assessed using the area under the receiver operating characteristic curve, Tjur’s R², and the Hosmer-Lemeshow goodness-of-fit test. P < 0.05 was considered statistically significant.
Protein S levels were initially evaluated using a clinically established cutoff of < 60% (a threshold commonly used to define mild deficiency in non-pregnant women of reproductive age). In univariable logistic regression, protein S levels below 60% were significantly associated with an increased risk of RPL (unadjusted OR = 4.38, p = 0.03), indicating that individuals with levels in this range had over 4 times the odds of RPL compared to those with levels ≥ 60%.
To fully utilize the continuous nature of the data and avoid potential loss of information associated with dichotomization, protein S was subsequently modeled as a continuous variable in multivariable logistic regression. After adjusting for potential confounders (age, CRP, WBC, Hb, anemia, PLT, and monocyte percentage), each 1% decrease in protein S level was associated with a marginally higher risk of RPL (adjusted OR = 0.98, 95% CI: 0.94-1.01, p = 0.11; Table II). The attenuation of the association in the multivariable model suggests that part of the crude effect observed with the dichotomous approach may be explained by confounding factors, particularly anemia and inflammatory markers.
4. Discussion
The present study investigated the association of serum calprotectin, protein C, and protein S levels in women with RPL. We found that the mean protein S level was significantly lower in the case group (66.05 ± 25.36) compared to the control group (78.28 ± 17.41). Although protein C levels were also lower in the case group (91.74 ± 16.74) relative to the control group (97.19 ± 12.76), this difference was not statistically significant. Given that protein S has a defined normal reference range, interpreting a reduction in its mean level without considering the proportion of individuals falling below the normal threshold may be misleading. In the present study, although the mean level of protein S was significantly lower in the RPL group, a more detailed analysis showed that the percentage of women with a marked reduction (below 60%) was considerably higher. This finding is more closely associated with the risk of RPL. Therefore, drawing conclusions based on the proportion of individuals below the normal range is more valid and clinically more interpretable.
Another major finding was that a deficiency in protein S was significantly associated with RPL, conferring an approximately 4.38‐fold increased risk. In contrast, although protein C and calprotectin levels were lower in RPL cases compared to controls, these differences were not statistically significant.
These observations add to the complex picture of coagulation and inflammation disturbances in RPL, underscoring the multifactorial etiology of this condition. Several studies have consistently reported that deficiencies in natural anticoagulants are linked to adverse pregnancy outcomes. One study reported that protein S deficiency was significantly associated with recurrent miscarriage, particularly in cases of second‐trimester losses. In contrast, the relationship with protein C deficiency did not reach statistical significance (10). In their study involving 90 women, a reduced protein S level was observed in the case group with recurrent losses, and PLTs showed no significant association with miscarriage. This finding aligns with our results, emphasizing the pivotal role of protein S in maintaining placental vascular integrity and preventing thrombosis. Similarly, another study compared protein C and protein S levels between women with recurrent early pregnancy loss and those with normal pregnancies. They reported that approximately 10% of individuals showed low levels of both proteins, and that these deficiencies were associated with adverse fetal outcomes such as intrauterine growth restriction and abnormal umbilical artery Doppler flow (6).
In a related study, it was found that the incidence of protein S deficiency, either alone or combined with protein C deficiency, was significantly higher in women with unexplained RPL (11). Consistent observation across these studies supports the hypothesis that even modest reductions in protein S can predispose to placental thrombosis and impair perfusion, thereby contributing to fetal loss. RPL is a prevalent and alarming complication, the cause of which remains unidentified in approximately half of the cases (16).
The role of inflammation in RPL has been increasingly recognized. Elevated CRP levels have been associated with miscarriage even in cases with normal fetal karyotypes (17). These findings suggest that subclinical systemic inflammation might impede maternal immune tolerance toward the fetal semi-allograft, leading to early pregnancy failure. Our study noted an elevation in CRP levels in the RPL group, although no statistically significant difference was observed in serum calprotectin. Calprotectin, a heterodimer composed of S100A8 and S100A9 proteins, is regarded as a sensitive marker of acute and chronic inflammation. A systematic review and prospective cohort study demonstrated that calprotectin levels were elevated in several pregnancy-associated disorders, including pre-eclampsia, even though its levels remain relatively stable in uncomplicated pregnancies (15).
Genetic studies further emphasize the inflammatory component of RPL. Certain CRP gene variants are associated with RPL independent of circulating CRP levels (18). These data indicate that the genetic predisposition to heightened inflammatory responses may contribute to a prothrombotic state, compounding the effects of protein S deficiency. Together, these studies suggest that inflammation and coagulation disturbances are intertwined, whereas systemic inflammatory markers like CRP and local mediators such as calprotectin could disrupt endothelial function and potentiate thrombotic events within the placenta.
The complex interplay between coagulation and inflammation is central to the pathogenesis of RPL (19). In a normal pregnancy, there is a delicate balance of increased procoagulant activity to protect against hemorrhage, while natural anticoagulants such as protein S counterbalance this hypercoagulability. However, in the setting of protein S deficiency, this balance is disturbed, leading to a hypercoagulable state that may result in placental thrombosis and subsequent fetal loss (8, 20). Moreover, inflammatory mediators can downregulate the expression of protein S on endothelial surfaces, further exacerbating the prothrombotic environment. These mechanisms are supported by both in vitro and clinical studies, highlighting the importance of evaluating both coagulation profiles and inflammatory status in women with RPL.
A recent meta-analysis involving a large cohort of cases found that the overall prevalence of inherited thrombophilia, including deficiencies in protein C and S, did not differ significantly between women with RPL and controls (21). This finding suggests that while inherited thrombophilia may not be universally prevalent in RPL, a deficiency in protein S could be an important factor in a specific subset of cases, particularly those with additional risk factors such as a positive family history of thrombosis.
The evidence from the literature and our study indicates that screening for protein S deficiency should be considered in the diagnostic workup of RPL, especially in cases with unexplained etiology and second-trimester losses. Early identification of protein S deficiency may allow for timely intervention with anticoagulant therapies such as low molecular weight heparin, which has been shown to improve fetal outcomes in thrombophilic women (6). Moreover, therapeutic strategies targeting inflammatory pathways might offer complementary benefits given the observed associations with systemic inflammation.
The current study also demonstrated that anemia is one of the causes of RPL. Anemia, more specifically iron-deficiency anemia, has been previously linked to pregnancy outcomes through its implication in poor oxygen transport to the placenta and fetus. Similarly, anemia can be suggestive of nutritional deficiencies or chronic inflammation; both are related to the pathophysiology of RPL. In this instance, a statistically significant difference between the RPL and control groups supports the concept that anemia may be part of a broader systemic profile affecting reproductive health.
4.1. Strengths and Limitations
Several limitations of the current investigation must be acknowledged. First, the cross-sectional design limits the ability to establish causality between protein S deficiency and RPL. Second, the relatively small sample size and single-center setting may have affected the generalizability of the findings. Third, while our study assessed key coagulation and inflammatory markers, it did not evaluate other thrombophilic factors or genetic predispositions that might modulate these pathways. Future research should focus on large-scale, multicenter, longitudinal studies incorporating comprehensive thrombophilia panels, including genetic analyses, to evaluate additional inflammatory markers. Standardized assay protocols and well-defined case cohorts will be essential to further elucidate the mechanisms underlying RPL and to identify targeted therapeutic strategies.
5. Conclusion
In summary, our study highlights the critical role of protein S deficiency in the pathogenesis of RPL, particularly in the context of second-trimester miscarriages. This study demonstrated that not only was the mean protein S level lower in women with RPL but a substantial proportion of them also have levels below the normal range, which carries greater clinical significance. Therefore, the primary factor associated with increased risk is the drop in protein S levels below the normal threshold, rather than merely the difference in mean values. Although protein C deficiency and calprotectin levels did not differ significantly between groups, the evidence from the literature supports a model in which an interplay between coagulation disturbances and systemic inflammation predisposes to placental thrombosis and fetal loss. Comprehensive evaluation of coagulation profiles, inflammatory markers, and genetic risk factors is warranted in women with RPL to improve diagnostic accuracy and guide personalized therapeutic interventions.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
N. Saki: Performed the study conception and design. F. Bakhshipour: Conducted the laboratory experiments and wrote the first draft of the manuscript. N. Saki and F. Bakhshipour: Revised the manuscript. MA. Jalali Far performed the statistical analyses. M. Torabizadeh and F. Moramezi contributed to patient selection and approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
This research was financially supported by Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. The authors confirm that no artificial intelligence (AI) software was used at any phase of this study, such as translation, editing, grammar checking, or data analysis.
Conflict of Interest
The authors declare that there is no conflict of interest.
Another major finding was that a deficiency in protein S was significantly associated with RPL, conferring an approximately 4.38‐fold increased risk. In contrast, although protein C and calprotectin levels were lower in RPL cases compared to controls, these differences were not statistically significant.
These observations add to the complex picture of coagulation and inflammation disturbances in RPL, underscoring the multifactorial etiology of this condition. Several studies have consistently reported that deficiencies in natural anticoagulants are linked to adverse pregnancy outcomes. One study reported that protein S deficiency was significantly associated with recurrent miscarriage, particularly in cases of second‐trimester losses. In contrast, the relationship with protein C deficiency did not reach statistical significance (10). In their study involving 90 women, a reduced protein S level was observed in the case group with recurrent losses, and PLTs showed no significant association with miscarriage. This finding aligns with our results, emphasizing the pivotal role of protein S in maintaining placental vascular integrity and preventing thrombosis. Similarly, another study compared protein C and protein S levels between women with recurrent early pregnancy loss and those with normal pregnancies. They reported that approximately 10% of individuals showed low levels of both proteins, and that these deficiencies were associated with adverse fetal outcomes such as intrauterine growth restriction and abnormal umbilical artery Doppler flow (6).
In a related study, it was found that the incidence of protein S deficiency, either alone or combined with protein C deficiency, was significantly higher in women with unexplained RPL (11). Consistent observation across these studies supports the hypothesis that even modest reductions in protein S can predispose to placental thrombosis and impair perfusion, thereby contributing to fetal loss. RPL is a prevalent and alarming complication, the cause of which remains unidentified in approximately half of the cases (16).
The role of inflammation in RPL has been increasingly recognized. Elevated CRP levels have been associated with miscarriage even in cases with normal fetal karyotypes (17). These findings suggest that subclinical systemic inflammation might impede maternal immune tolerance toward the fetal semi-allograft, leading to early pregnancy failure. Our study noted an elevation in CRP levels in the RPL group, although no statistically significant difference was observed in serum calprotectin. Calprotectin, a heterodimer composed of S100A8 and S100A9 proteins, is regarded as a sensitive marker of acute and chronic inflammation. A systematic review and prospective cohort study demonstrated that calprotectin levels were elevated in several pregnancy-associated disorders, including pre-eclampsia, even though its levels remain relatively stable in uncomplicated pregnancies (15).
Genetic studies further emphasize the inflammatory component of RPL. Certain CRP gene variants are associated with RPL independent of circulating CRP levels (18). These data indicate that the genetic predisposition to heightened inflammatory responses may contribute to a prothrombotic state, compounding the effects of protein S deficiency. Together, these studies suggest that inflammation and coagulation disturbances are intertwined, whereas systemic inflammatory markers like CRP and local mediators such as calprotectin could disrupt endothelial function and potentiate thrombotic events within the placenta.
The complex interplay between coagulation and inflammation is central to the pathogenesis of RPL (19). In a normal pregnancy, there is a delicate balance of increased procoagulant activity to protect against hemorrhage, while natural anticoagulants such as protein S counterbalance this hypercoagulability. However, in the setting of protein S deficiency, this balance is disturbed, leading to a hypercoagulable state that may result in placental thrombosis and subsequent fetal loss (8, 20). Moreover, inflammatory mediators can downregulate the expression of protein S on endothelial surfaces, further exacerbating the prothrombotic environment. These mechanisms are supported by both in vitro and clinical studies, highlighting the importance of evaluating both coagulation profiles and inflammatory status in women with RPL.
A recent meta-analysis involving a large cohort of cases found that the overall prevalence of inherited thrombophilia, including deficiencies in protein C and S, did not differ significantly between women with RPL and controls (21). This finding suggests that while inherited thrombophilia may not be universally prevalent in RPL, a deficiency in protein S could be an important factor in a specific subset of cases, particularly those with additional risk factors such as a positive family history of thrombosis.
The evidence from the literature and our study indicates that screening for protein S deficiency should be considered in the diagnostic workup of RPL, especially in cases with unexplained etiology and second-trimester losses. Early identification of protein S deficiency may allow for timely intervention with anticoagulant therapies such as low molecular weight heparin, which has been shown to improve fetal outcomes in thrombophilic women (6). Moreover, therapeutic strategies targeting inflammatory pathways might offer complementary benefits given the observed associations with systemic inflammation.
The current study also demonstrated that anemia is one of the causes of RPL. Anemia, more specifically iron-deficiency anemia, has been previously linked to pregnancy outcomes through its implication in poor oxygen transport to the placenta and fetus. Similarly, anemia can be suggestive of nutritional deficiencies or chronic inflammation; both are related to the pathophysiology of RPL. In this instance, a statistically significant difference between the RPL and control groups supports the concept that anemia may be part of a broader systemic profile affecting reproductive health.
4.1. Strengths and Limitations
Several limitations of the current investigation must be acknowledged. First, the cross-sectional design limits the ability to establish causality between protein S deficiency and RPL. Second, the relatively small sample size and single-center setting may have affected the generalizability of the findings. Third, while our study assessed key coagulation and inflammatory markers, it did not evaluate other thrombophilic factors or genetic predispositions that might modulate these pathways. Future research should focus on large-scale, multicenter, longitudinal studies incorporating comprehensive thrombophilia panels, including genetic analyses, to evaluate additional inflammatory markers. Standardized assay protocols and well-defined case cohorts will be essential to further elucidate the mechanisms underlying RPL and to identify targeted therapeutic strategies.
5. Conclusion
In summary, our study highlights the critical role of protein S deficiency in the pathogenesis of RPL, particularly in the context of second-trimester miscarriages. This study demonstrated that not only was the mean protein S level lower in women with RPL but a substantial proportion of them also have levels below the normal range, which carries greater clinical significance. Therefore, the primary factor associated with increased risk is the drop in protein S levels below the normal threshold, rather than merely the difference in mean values. Although protein C deficiency and calprotectin levels did not differ significantly between groups, the evidence from the literature supports a model in which an interplay between coagulation disturbances and systemic inflammation predisposes to placental thrombosis and fetal loss. Comprehensive evaluation of coagulation profiles, inflammatory markers, and genetic risk factors is warranted in women with RPL to improve diagnostic accuracy and guide personalized therapeutic interventions.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
N. Saki: Performed the study conception and design. F. Bakhshipour: Conducted the laboratory experiments and wrote the first draft of the manuscript. N. Saki and F. Bakhshipour: Revised the manuscript. MA. Jalali Far performed the statistical analyses. M. Torabizadeh and F. Moramezi contributed to patient selection and approved the final manuscript. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
This research was financially supported by Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. The authors confirm that no artificial intelligence (AI) software was used at any phase of this study, such as translation, editing, grammar checking, or data analysis.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
