
International Journal of
Reproductive Biomedicine
Sat, Apr 27, 2024
[Archive]
Volume 5, Issue 3 (7-2007)
IJRM 2007, 5(3): 65-0 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shahrokh Tehrani Nejad E, Moini A, Amirchaghmaghi E, Hossein Rashidi B, Jaberi Pour P, Azimi Neko E. Effect of intramural uterine myoma on the outcome of ART cycles. IJRM 2007; 5 (3) :65-0
URL: http://ijrm.ir/article-1-69-en.html
URL: http://ijrm.ir/article-1-69-en.html
Ensieh Shahrokh Tehrani Nejad * 
 1, Ashraf Moini2 , Elham Amirchaghmaghi2 , Batol Hossein Rashidi3 , Parvin Jaberi Pour4 , Elham Azimi Neko5
1, Ashraf Moini2 , Elham Amirchaghmaghi2 , Batol Hossein Rashidi3 , Parvin Jaberi Pour4 , Elham Azimi Neko5
1, Ashraf Moini2 , Elham Amirchaghmaghi2 , Batol Hossein Rashidi3 , Parvin Jaberi Pour4 , Elham Azimi Neko5
1- Endocrinology and Female Infertility Department, Royan Institute,Tehran ,Iran , tehraninejad @royaninstitute.org
2- Endocrinology and Female Infertility Department, Royan Institute,Tehran ,Iran
3- Gynecology and Obstetrics Department, Faculty of Medicine, Tehran University of Medical Sciences,Tehran , Iran
4- Gynecologist, Tehran,Iran
5- Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
2- Endocrinology and Female Infertility Department, Royan Institute,Tehran ,Iran
3- Gynecology and Obstetrics Department, Faculty of Medicine, Tehran University of Medical Sciences,Tehran , Iran
4- Gynecologist, Tehran,Iran
5- Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran
Full-Text [PDF 100 kb]
(484 Downloads)
| Abstract (HTML) (3187 Views)
Full-Text: (376 Views)
Introduction
Uterine leiomyomas (fibroids) appear to be the most common female pelvic tumor (1-4), occurring in as many as 30% of women > 30 years of age (1, 5). Although leiomyomas may be asymptomatic (1, 4), they are associated with various symptoms, including menorrhagia, pelvic pain, and urinary symptoms (1). Although fibroids are implicated as a possible cause of subfertility, this is not accepted universally (5). In addition to the possible adverse effects of uterine leiomyomas on female fecundity,
some evidence suggests that leiomyomas are associated with an increased risk of spontaneous abortion (6).The mechanism by which the association with subfertility occurs may depend on the size and location of the fibroids (5). The association of submucosal fibroids with subfertility is well recognized (7), and pregnancy rates of up to 43% have been achieved following hysteroscopic resection (8, 9). Submucosal and intramural leiomyomata which distort the endometrial cavity clearly affect outcome. Bajekal and Li (2000) in their review article stated that intramural fibroids have an intermediate role for infertility and miscarriage (10) .However, the impact and possible mechanism of action of intramural lesions, which do not clearly alter the contour of the endometrial cavity, remain controversial (11). Some theories include corneal occlusion that could be caused if the intramural fibroid is adjacent to the intramural tubal segment (12). Other theories are that fibroids could interfere with ovum pick transport, sperm migration, impairment of blood supply to the endometrium, atrophy and ulceration the endometrium (13-16) .Other recent studies have evaluated alterations in gene expression and local cytokine release which may also play a role(11).As mentioned ,some theories suggest that obstruction of gamete transport may be responsible for the decrease in fertility (17) .This is the reason for choosing IVF group to study since at least obstruction to gamete or sperm transport would be eliminated.The aim of the present study was to evaluate the effect of uterine intramural myoma, below 6cm and not encroaching on the endometrium, on the outcome of IVF/ICSI cycles.
Materials and methods
In this prospective cohort study, infertile women under 38 years old who were candidate for IVF/ICSI cycles in Royan Institute for the first time were enrolled. This study was approved by Ethics committee of Royan Institute and carried out between January 2001 and December 2002. All patients, in whom a myoma was reported, were evaluated for its exact position with vaginal sonography (Prob7, Aloka 1000, Japan). Ninety four patients with intramural fibroids less than 6cm not encroaching on the endometrial cavity were included in this study as myoma group while 184 age-matched patients without uterine myoma were considered as control group. All patients signed informed consent forms. Patients undergoing IVF/ICSI cycles involving oocyte donation, transfer of cryopreserved embryo, patients with intramural myoma greater than 6 cm or with intramural myoma encroaching on the endometrial cavity, patients with history of myomectomy and patients who were prone to OHSS were excluded.
Long GnRH agonist protocol was used for ovarian stimulation. In this protocol, the women had first been down regulated with GnRH analogue (Buserline, Hoechst, Germany), which was administered 500 µg/day subcutaneously from 21st day of previous menstrual cycle. When pituitary suppression was achieved (on second day of menstrual cycle FSH≤ 5 IU/ml, LH≤ 5IU/ml, progestrone≤ 1ng/ml, Estradiol≤ 50pg/ml), Buserline was reduced to 200µg/day and 150-225 IU human Menopausal Gonadotrophin (Menopur, Ferring, Germany) was administrated intramuscularly from second day of menstrual cycle daily. After 3 or more follicles had reached 18mm in diameter, 10000 IU human Chorionic gonadotropins (hCG, Organon, Holland) was used to induce oocyte maturation. Oocytes were aspirated transvaginally with ultrasound guidance 34-36 h later. After that IVF or ICSI were done. Uterine embryo transfer was performed two days after oocyte retrieval. Beta hCG was checked two weeks after embryo transfer. Clinical pregnancy was defined as the presence of at least one gestational sac with detectable fetal heart activity by transvaginal sonography.
Statistical analysis
Student t-test and χ2 (Chi-square) test were used for the statistical analysis. Results were presented as mean value ±SD. P value < 0.05 was considered as statistically significant level.
Results
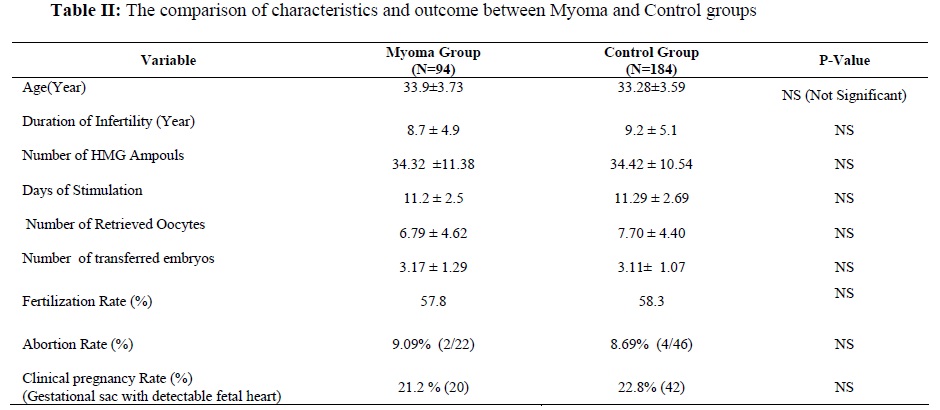
In this study, 94 women as myoma group and 184 women as control group were studied .The cause of infertility in each group is shown in Table I and included: male factor, tubal factor, Endometriosis, ovulatory factor and unexplained infertility. In total, 89.4% of myoma group and 89.1% of control group had primary infertility.There was no statistically significant differences between two groups in respect to cause of infertility and type of infertility (primary or secondary).The mean age of patients was 33.9 ±3.37 years in myoma group and 33.28 ±3.59 years in control group .The mean duration of infertility was 8.7 ±4.9 years in myoma group and 9.2 ±5.1 years in control group which these differences were not statistically significant (p>0.05).The mean duration and number of used HMG ampoules, number of retrieved oocytes, fertilization rate, abortion rate and number of transferred embryos did not significantly differ between two groups (Table II). In myoma group, 55.3% had intramural myoma <3 cm while others had myoma between 3-6 cm in diameter .Also 21.4% had single myoma while 78.6% had multiple myoma .Pregnancy rate was 19.2% in patients who had myoma <3 cm in comparison to

Discussion
Although the fibroids are common, their influence on fertility remains controversial. Assisted reproductive technologies give a setting in which one can examine the effect of fibroids on implantation (18). It is well accepted that the anatomical location of the fibroids is an important factor, with submucous, intramural and subserosal fibroids being in decreasing order of importance, in causing infertility (10). One question facing a physician is whether myomectomy should be performed prior to embryo transfer. Unfortunately there have been several conflicting studies as to whether smaller intramural fibroids adversely affect IVF pregnancy outcome .The aim of present study was to evaluate whether the presence of intramural fibroids less than 6 cm, in the absence of uterine cavity distortion, had a detrimental effect on pregnancy rate after IVF/ICSI.
The result of this study showed that the presence of this type of intramural myoma had no adverse effect on clinical pregnancy and abortion rate. These results were similar to Oliveira et al (19) while inconsistenc with Hart et al (5) and Khalaf et al (20) studies. Oliveira et al (2004) in a retrospective study, evaluated 245 women with subserosal and or intramural fibroids that didn,t compress the uterine cavity and 245 women with no evidence of fibroids undergoing IVF/ICSI cycles. Their results showed patients with subserosal or intramural fibroids <4 cm had IVF-ICSI outcomes (pregnancy, implantation, and abortion rates) similar to those of controls while patients with intramural fibroids >4 cm had lower pregnancy rates than patients with intramural fibroids ≤ 4.0 cm (19) .In recent survey by Khalaf et al (2006), only patients with small (≤ 5 cm) intramural fibroids not encroaching upon the endometrial cavity (n=112) were compared with control group (n=322). Results showed that the pregnancy rate was statistically significant lower in myoma group in comparison with control group (23.6% vs. 32.9%, respectively) (20). Yarali and Bukulmez (2002) assessed 108 women with uterine fibroids (intramural and subserous) and 324 age and BMI matched- controls undergoing ICSI cycles in their retrospective study. The implantation and clinical pregnancy rates were similar .They concluded that the presence of intramural and subserous fibroids does not adversely affect clinical pregnancy and implantation rates in patients undergoing ICSI (18) although they did not excluded the myomas distorted the uterine cavity .Check et al (2002) in their prospective study , compared 61 women with intramural fibroids ≤ 5 cm with 61 age matched control patients .The results showed that clinical pregnancy and spontaneous abortion did not significantly differ between two groups although there was a distinct trend for lower live delivery rates (21).In another prospective study ,Hart et al (2001) studied 112 women with and 322 women without intramural fibroids undergoing IVF/ICSI cycles. In their study, implantation, pregnancy and ongoing pregnancy rates were significantly reduced compared with control group (5) .It is necessary to mention that in Hart,s study, women in myoma groups were older than control group (average two years older) while in present study, we studied age matched patients.
Conclusion
According to the controversies and side effects of myomectomy especially for small myoma such as adhesion and recurrence of myoma , we believed that uterine intramural myoma should not be necessarily excised when was diagnosed in infertile patients as long as it is not encroaching on the cavity with below 6 cm in diameter. If repeated IVF failure occurred in these cases, myomectomy can be suggested.
Acknowledgment
The authors wish to thank staff of Royan Institute for their cooperation.
Uterine leiomyomas (fibroids) appear to be the most common female pelvic tumor (1-4), occurring in as many as 30% of women > 30 years of age (1, 5). Although leiomyomas may be asymptomatic (1, 4), they are associated with various symptoms, including menorrhagia, pelvic pain, and urinary symptoms (1). Although fibroids are implicated as a possible cause of subfertility, this is not accepted universally (5). In addition to the possible adverse effects of uterine leiomyomas on female fecundity,
some evidence suggests that leiomyomas are associated with an increased risk of spontaneous abortion (6).The mechanism by which the association with subfertility occurs may depend on the size and location of the fibroids (5). The association of submucosal fibroids with subfertility is well recognized (7), and pregnancy rates of up to 43% have been achieved following hysteroscopic resection (8, 9). Submucosal and intramural leiomyomata which distort the endometrial cavity clearly affect outcome. Bajekal and Li (2000) in their review article stated that intramural fibroids have an intermediate role for infertility and miscarriage (10) .However, the impact and possible mechanism of action of intramural lesions, which do not clearly alter the contour of the endometrial cavity, remain controversial (11). Some theories include corneal occlusion that could be caused if the intramural fibroid is adjacent to the intramural tubal segment (12). Other theories are that fibroids could interfere with ovum pick transport, sperm migration, impairment of blood supply to the endometrium, atrophy and ulceration the endometrium (13-16) .Other recent studies have evaluated alterations in gene expression and local cytokine release which may also play a role(11).As mentioned ,some theories suggest that obstruction of gamete transport may be responsible for the decrease in fertility (17) .This is the reason for choosing IVF group to study since at least obstruction to gamete or sperm transport would be eliminated.The aim of the present study was to evaluate the effect of uterine intramural myoma, below 6cm and not encroaching on the endometrium, on the outcome of IVF/ICSI cycles.
Materials and methods
In this prospective cohort study, infertile women under 38 years old who were candidate for IVF/ICSI cycles in Royan Institute for the first time were enrolled. This study was approved by Ethics committee of Royan Institute and carried out between January 2001 and December 2002. All patients, in whom a myoma was reported, were evaluated for its exact position with vaginal sonography (Prob7, Aloka 1000, Japan). Ninety four patients with intramural fibroids less than 6cm not encroaching on the endometrial cavity were included in this study as myoma group while 184 age-matched patients without uterine myoma were considered as control group. All patients signed informed consent forms. Patients undergoing IVF/ICSI cycles involving oocyte donation, transfer of cryopreserved embryo, patients with intramural myoma greater than 6 cm or with intramural myoma encroaching on the endometrial cavity, patients with history of myomectomy and patients who were prone to OHSS were excluded.
Long GnRH agonist protocol was used for ovarian stimulation. In this protocol, the women had first been down regulated with GnRH analogue (Buserline, Hoechst, Germany), which was administered 500 µg/day subcutaneously from 21st day of previous menstrual cycle. When pituitary suppression was achieved (on second day of menstrual cycle FSH≤ 5 IU/ml, LH≤ 5IU/ml, progestrone≤ 1ng/ml, Estradiol≤ 50pg/ml), Buserline was reduced to 200µg/day and 150-225 IU human Menopausal Gonadotrophin (Menopur, Ferring, Germany) was administrated intramuscularly from second day of menstrual cycle daily. After 3 or more follicles had reached 18mm in diameter, 10000 IU human Chorionic gonadotropins (hCG, Organon, Holland) was used to induce oocyte maturation. Oocytes were aspirated transvaginally with ultrasound guidance 34-36 h later. After that IVF or ICSI were done. Uterine embryo transfer was performed two days after oocyte retrieval. Beta hCG was checked two weeks after embryo transfer. Clinical pregnancy was defined as the presence of at least one gestational sac with detectable fetal heart activity by transvaginal sonography.
Statistical analysis
Student t-test and χ2 (Chi-square) test were used for the statistical analysis. Results were presented as mean value ±SD. P value < 0.05 was considered as statistically significant level.
Results
In this study, 94 women as myoma group and 184 women as control group were studied .The cause of infertility in each group is shown in Table I and included: male factor, tubal factor, Endometriosis, ovulatory factor and unexplained infertility. In total, 89.4% of myoma group and 89.1% of control group had primary infertility.There was no statistically significant differences between two groups in respect to cause of infertility and type of infertility (primary or secondary).The mean age of patients was 33.9 ±3.37 years in myoma group and 33.28 ±3.59 years in control group .The mean duration of infertility was 8.7 ±4.9 years in myoma group and 9.2 ±5.1 years in control group which these differences were not statistically significant (p>0.05).The mean duration and number of used HMG ampoules, number of retrieved oocytes, fertilization rate, abortion rate and number of transferred embryos did not significantly differ between two groups (Table II). In myoma group, 55.3% had intramural myoma <3 cm while others had myoma between 3-6 cm in diameter .Also 21.4% had single myoma while 78.6% had multiple myoma .Pregnancy rate was 19.2% in patients who had myoma <3 cm in comparison to
26.1% in patients with myoma between 3-6 cm (p-value=0.302) also it was 22.38 % in patients with one myoma and 22.22 % in patients with more than one myomas which these differences were not statistically significant.
Discussion
Although the fibroids are common, their influence on fertility remains controversial. Assisted reproductive technologies give a setting in which one can examine the effect of fibroids on implantation (18). It is well accepted that the anatomical location of the fibroids is an important factor, with submucous, intramural and subserosal fibroids being in decreasing order of importance, in causing infertility (10). One question facing a physician is whether myomectomy should be performed prior to embryo transfer. Unfortunately there have been several conflicting studies as to whether smaller intramural fibroids adversely affect IVF pregnancy outcome .The aim of present study was to evaluate whether the presence of intramural fibroids less than 6 cm, in the absence of uterine cavity distortion, had a detrimental effect on pregnancy rate after IVF/ICSI.
The result of this study showed that the presence of this type of intramural myoma had no adverse effect on clinical pregnancy and abortion rate. These results were similar to Oliveira et al (19) while inconsistenc with Hart et al (5) and Khalaf et al (20) studies. Oliveira et al (2004) in a retrospective study, evaluated 245 women with subserosal and or intramural fibroids that didn,t compress the uterine cavity and 245 women with no evidence of fibroids undergoing IVF/ICSI cycles. Their results showed patients with subserosal or intramural fibroids <4 cm had IVF-ICSI outcomes (pregnancy, implantation, and abortion rates) similar to those of controls while patients with intramural fibroids >4 cm had lower pregnancy rates than patients with intramural fibroids ≤ 4.0 cm (19) .In recent survey by Khalaf et al (2006), only patients with small (≤ 5 cm) intramural fibroids not encroaching upon the endometrial cavity (n=112) were compared with control group (n=322). Results showed that the pregnancy rate was statistically significant lower in myoma group in comparison with control group (23.6% vs. 32.9%, respectively) (20). Yarali and Bukulmez (2002) assessed 108 women with uterine fibroids (intramural and subserous) and 324 age and BMI matched- controls undergoing ICSI cycles in their retrospective study. The implantation and clinical pregnancy rates were similar .They concluded that the presence of intramural and subserous fibroids does not adversely affect clinical pregnancy and implantation rates in patients undergoing ICSI (18) although they did not excluded the myomas distorted the uterine cavity .Check et al (2002) in their prospective study , compared 61 women with intramural fibroids ≤ 5 cm with 61 age matched control patients .The results showed that clinical pregnancy and spontaneous abortion did not significantly differ between two groups although there was a distinct trend for lower live delivery rates (21).In another prospective study ,Hart et al (2001) studied 112 women with and 322 women without intramural fibroids undergoing IVF/ICSI cycles. In their study, implantation, pregnancy and ongoing pregnancy rates were significantly reduced compared with control group (5) .It is necessary to mention that in Hart,s study, women in myoma groups were older than control group (average two years older) while in present study, we studied age matched patients.
Conclusion
According to the controversies and side effects of myomectomy especially for small myoma such as adhesion and recurrence of myoma , we believed that uterine intramural myoma should not be necessarily excised when was diagnosed in infertile patients as long as it is not encroaching on the cavity with below 6 cm in diameter. If repeated IVF failure occurred in these cases, myomectomy can be suggested.
Acknowledgment
The authors wish to thank staff of Royan Institute for their cooperation.
Type of Study: Original Article |
References
1. Stovall DW, Parrish SB,Van Voorhis BJ, Hahn SJ, Sparks AET, Syrop CH. Uterine leiomyomas reduce the efficacy of assisted reproduction cycles: results of a matched follow-up study. Hum Reprod 1998; 13:192-197. [DOI:10.1093/humrep/13.1.192]
2. Chaker A, Ferchiou M, Lahmar MM, Zhioua F, Meriah S. Uterine fibromyomas: fertility after myomectomy . About 41 cases .Tunis Med 2004;82:1075-1081.
3. Begum S, Khan S. Audit of leiomyoma uterus at Khyber hospital Peshawar. J Ayub Med Coll Abbottabad. 2004;16:46-49.
4. Eldar-Geva T, Meagher S, Healy DL, MacLachlan V, Breheny S, Wood C. Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril 1998; 70:687-691. [DOI:10.1016/S0015-0282(98)00265-9]
5. Hart R, Khalaf Y, Yeong CH, Seed P, Taylor A, Braude P.A prospective controlled study of the effect of intramural uterine fibroids on the outcome of assisted conception. Hum Reprod 2001;16: 2411-2417. [DOI:10.1093/humrep/16.11.2411]
6. Matsunaga E, Shiota K. Ectopic pregnancy and myoma uteri: teratogenic effects and maternal characteristics. Teratology 1980;21:61-69. [DOI:10.1002/tera.1420210108]
7. Surrey ES. Impact of intramural leiomyomata on in-vitro fertilization - embryo transfer cycle outcome. Curr Opin Obstet Gynecol 2003;15:239-242. [DOI:10.1097/00001703-200306000-00005]
8. Hart R, Molnar BG, Magos A. Long term follow-up of hysteroscopic myomectomy assessed by survival analysis. Br J Obstet. Gynaecol 1999; 106:700-705. [DOI:10.1111/j.1471-0528.1999.tb08370.x]
9. Bernard G, Darai E, Poncelet C, Benifla JL, Madelenat P. Fertility after hysteroscopic myomectomy: effect of intramural myomas associated. Eur J Obstet Gynecol Reprod Biol 2000; 88: 85-90. [DOI:10.1016/S0301-2115(99)00123-2]
10. Bajekal N, Li TC. Fibroids, infertility and pregnancy wastage. Hum Reprod Update 2000; 6:614-620. [DOI:10.1093/humupd/6.6.614]
11. Surrey ES. Impact of intramural leiomyomata on in-vitro fertilization-embryo transfer cycle outcome. Curr Opin Obstet Gynecol 2003;15:239-242. [DOI:10.1097/00001703-200306000-00005]
12. Ingersoll FM. Fertility following myomectomy. Fertil Steril 1963;14:596. [DOI:10.1016/S0015-0282(16)35042-7]
13. Hunt JE, Wallach EE. Uterine factor in infertility: an overview. Clin Gynecol 1974; 17: 44-64. [DOI:10.1097/00003081-197412000-00004]
14. Buttram VC, Reiter RC. Uterine leiomyomata: etiology symptomatology, and management. Fertil Steril 1981; 36:433-445. [DOI:10.1016/S0015-0282(16)45789-4]
15. Iosif CS, Akerland M. Fibromyomas and uterine activity. Acta Obstet Gynecol Scand 1983;62:165-167. [DOI:10.3109/00016348309155784]
16. Vollenhoven BJ, Lawrence AS, Hely, DL. Uterine fibroids: A clinical review. Br. J. Obstet. Gynecol 1990;97:285-298. [DOI:10.1111/j.1471-0528.1990.tb01804.x]
17. Farhi J, Ashkenazi J, Feldberg D, Dicker D, Orvieto R, Ben Rafael Z. Effect of uterine leiomyomata on the results of in-vitro fertilization treatment. Hum. Reprod 1995;10:2576-2578. [DOI:10.1093/oxfordjournals.humrep.a135748]
18. Yarali H, Bukulmez O. The effect of intramural and subserous uterine fibroids on implantation and clinical pregnancy rates in patients having intracytoplasmic sperm injection. Arch Gynecol Obstet 2002; 266:30-33. [DOI:10.1007/PL00007491]
19. Oliveira FG, Abdelmassih VG, Diamond MP, Dozortsev D, Melo NR, Abdelmassih R. Impact of subserosal and intramural uterine fibroids that do not distort the endometrial cavity on the outcome of in vitro fertilization-intracytoplasmic sperm injection. Fertil Steril 2004; 81:582-587. [DOI:10.1016/j.fertnstert.2003.08.034]
20. Khalaf Y, Ross C, El-Toukhy T, Hart R, Seed P, Braude P. The effect of small intramural uterine fibroids on the cumulative outcome of assisted conception. Hum Reprod 2006:21:2640-2644. [DOI:10.1093/humrep/del218]
21. Check JH, Choe JK, Lee G, Dietterich C. The effect on IVF outcome of small intramural fibroids not compressing the uterine cavity as determined by a prospective matched control study. Hum Rep 2002; 17:1244-1248. [DOI:10.1093/humrep/17.5.1244]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
