
International Journal of
Reproductive Biomedicine
Thu, Apr 18, 2024
[Archive]
Volume 5, Issue 5 (7-2007)
IJRM 2007, 5(5): 187-190 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gharabaghi P, Abdollahifard S, Gharabaghi M, Nouri M. Comparing the levels of ßHCG, progesterone and estradiol between ectopic pregnancy and normal intrauterine pregnancy. IJRM 2007; 5 (5) :187-190
URL: http://ijrm.ir/article-1-90-en.html
URL: http://ijrm.ir/article-1-90-en.html


1- Department of Obstetrics and Gynecology, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran , pm_gharabaghi@yahoo.com
2- Department of Obstetrics and Gynecology, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
3- Department of Pediatrics, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
4- Department of Biochemistry, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
2- Department of Obstetrics and Gynecology, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
3- Department of Pediatrics, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
4- Department of Biochemistry, Alzahra Hospital, Tabriz University of Medical Sciences, Tabriz, Iran
Keywords: Beta subunit of Human Chorionic Gonadotropin (ßHCG), Estradiol, Progesterone, Ectopic pregnancy, Normal intrauterine pregnancy.
Full-Text [PDF 41 kb]
(452 Downloads)
| Abstract (HTML) (2826 Views)
Introduction
Ectopic pregnancy is a potentially life-threatening condition in which the embryo implants outside the uterine endometrial cavity. There was dramatic advances in the diagnosis and treatment of this potentially fatal condition last few decades. With earlier diagnosis, the prognosis for ectopic pregnancy has shifted from a grave, life threatening disease to a more benign condition. The treatment goal also shifted from preventing mortality to reducing morbidity and preserving fertility. To reduce maternal mortality and morbidity, early recognition of ectopic pregnancy is critical (1, 2).
History and physical examination may or may not provide useful diagnostic information. The accuracy of initial clinical evaluation is less than 50%. Additional tests are frequently required to differentiate early viable intrauterine pregnancy with suspected ectopic or abnormal intrauterine pregnancy (3, 4).
Human chorionic gonadotropin (HCG), is a glycoprotein made by placental syncytiotrophoblast (1-5). It is detectable in plasma of pregnant women about 7.5 to 9.5 days after the midcycle surge of LH (5). Therefore, the level of HCG in blood increases rapidly with maximal level of 50000-100000 mlu/ml attained at about 8-10 weeks of gestation (5,6). Nonetheless, HCG is present in the plasma and urine of probably all women with ectopic pregnancies, albeit generally in lower concentration than in women with normal pregnancies of comparable stages, because of the ectopic implantation, disruption of trophoblasts by hemorrhage, or embryonic death (4,5,7). Progesterone is largely produced by the corpus luteum until about 10 weeks of gestation. In the first 5-6 weeks of pregnancy, HCG stimulation of the corpus luteum results in the daily secretion of about 25 mg of progesterone and 0.5 mg of estradiol. Although estrogen levels begin to increase at 4-5 weeks due to placental secretion, progesterone production by the placenta does not significantly increase until about 10-11 weeks after ovulation (6). A single serum progesterone measurement in early gestation has been found by several groups to be of great use in differentiating an ectopic from an intrauterine gestation (8, 9). However, the diagnostic value of simple E2 and P in the patients with EPs could not identify a discriminatory cut-off value because there was a considerable overlap in serum P and E2 between the patients with intrauterine pregnancy and ectopic pregnancy (10,11).
Materials and methods
This case-control study was performed in Alzahra Educational Treatment Center. The study group included 43 women with symptoms or ultrasound finding of ectopic pregnancy. Which was confirmed by laparascopy or laparatomy in all cases. The controls were 42 women of normal intrauterine pregnancy of similar gestational age as assessed by menstrual dates and confirmed by ultrasound scans. All women gave informed consent to the study, which had been approved by the local institutional review board.
Blood samples for the measurement of betasubunit human chorionic gonadotropin, estradiol and progesterone were drawn in all the women upon admission. Exdra blood sample was drawn for measurement of ßHCG 24 hours after admission. Women with hemodynamically unstable status were excluded. From the study Serum level of ßHCG were measured by Radio Immuno Assay (RIA- incstar kit), progesterone by Enzyme Linked Immuno Sorbent Assay (ELISA- pantex kit), and estradiol by (RIA- analyze kit). Sample size calculations, assuming 80% power and 0.05 type I error to detect mean differences, indicated the need for at least 41 patients in each group. SPSS.13/win statistical software was used for analyzing the data. Data were presented as mean±standard deviation. A parametric independent sample t test was used to compare differences between two groups. Level of statistical significance was set at p<0.05. By determining cut-off levels of these parameters the efficiency and sensitivity of each in prediction of ectopic pregnancy were estimated.
Results
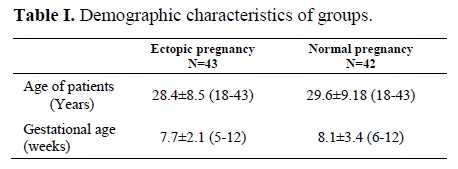
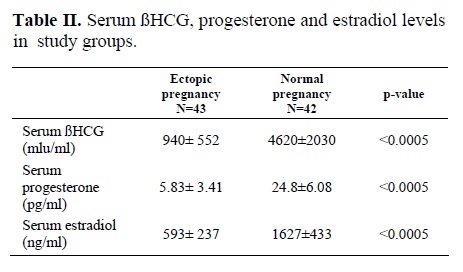
In this study, no substantial differences were noted in descriptions of the two groups regarding maternal age (Table 1). Study cases with suspicious ectopic pregnancy had a positive pregnancy test, lower abdominal pain, and vaginal bleeding. Women with normal intrauterine pregnancy (control group) had no evidence of abortion. The mean serum level of ßHCG was 940 ± 552 miu/ml in the case group and 4620 ± 2030 miu/ml in the control group (p<0.0005) (Table 2). The average rate of ßHCG rising was 8.2 % for 24 hours in the patients with ectopic pregnancy and 32.8% for 24 hours in the women with normal intrauterine pregnancy. The mean serum level of progesterone and estradiol in patients with ectopic pregnancy (5.83 ± 3.41 ng/ml, 593± 237 pg/ml, respectively) were significantly lower than in women with normal intrauterine pregnancy (24.8 ± 6.08 ng/ml, 1627 ± 433 pg/ml, respectively) (p<0.0005).
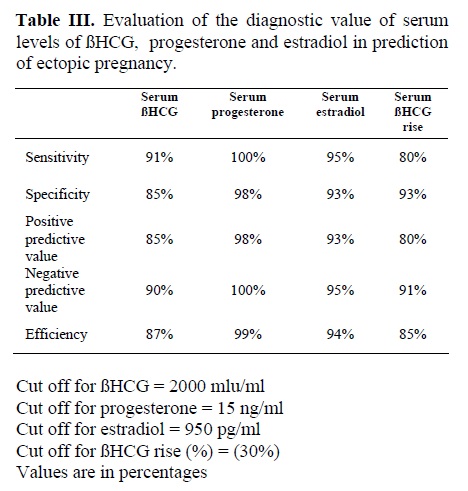
Serum ßHCG level had 91% sensitivity and 85% specifity at a cut-off value of 2000 miu/ml in diagnosis of ectopic pregnancy. Our results showed that ßHCG rising with 80% sensitivity and 93% specificity at a cut-off value of 30% can use for diagnosis. Serum level of progesterone had the greatest sensitivity (100%) and specificity (98%) at a cut-off value of 15 ng/ml. While serum level of estradiol showed 95% sensitivity and 93% specificity at a cut-off value of 950 pg/m. However we could not identify a discriminatory cut-off value because there was a considerable overlap in serum P and E2 levels between the patients with EP and NIUP (10).
Discussion
During the past decade, as modern refinements for identification of ectopic pregnancy have evolved, the majority of these cases (perhaps 80%) are diagnosed before rupture. Coincidentally, the death rate has decreased appreciably (5). The intial step of diagnosis of ectopic pregnancy is to screen for presence of pregnancy (1). Today, early diagnosis of ectopic pregnancy is possible with highly sensitive and rapid ß subunit of human chorionic gonadotropin assay with the aid of vaginal ultrasound (1,2) if ß-HCG is not detected with the use of radioimmunoassay of serum, the diagnosis of ectopic pregnancy can, with a rare exception, be ruled out (8). The early diagnosis is more beneficial from the point of possibility of medical therapy or conservative surgery (12). According to the results of this study, significant differences between serum ßHCG levels in case and control group were noticed (p<0.0005). The specificity and sensitivity of single HCG measurement in detection of ectopic pregnancy at the cut-off level of 2000 mlu/ml were 91% and 85% respectively. Although about 85% of women with ectopic pregnancy have serum HCGlevels lower than those seen in normal pregnancy at a similar age. However a single quantitative HCG assay can not be used for diagnosis of ectopic pregnancy because the actual dates of ovulation and conception are not known for most women (8). There is considerable overlap of values between normal and abnormal pregnancies at a given gestational age (3).
In normal pregnancies with early gestational age, the level of circulating HCG doubles about every 2 days. In our study the mean percentages of ßHCG rising in EP and NIUP after 24 hours were 8.2 and 32.8, respectively. Serial measurement of HCG with 80% sensitivity and 93% specificity at the cut off level of 30% is the great assistance in early diagnosis of unruptured ectopic pregnancy. In abnormal pregnancies (ectopic pregnancy and those destined to abort), HCG level usually doesn't increase at the same rate.
However, a differentiation between increasing rate of HCG in women with an ectopic pregnancy is similar to an impending intrauterine abortion (8). In these cases the measurement of serum progestrone is helpful. A serum progesterone level less than 5 ng/ml is highly suggestive of an abnormal pregnancy, but it is not 100% predictive. The risk of normal pregnancy with a serum progesterone level less than 5.0 ng/ml is approximately 1/1500 (3). A single progesterone or estradiol measurement may suggest non viability of a pregnancy without precise knowledge of gestational age, even when the serum HCG is below the discriminatory zone (1).
When the serum progesterone level is less than 2.5 ng/ml, uterin curettage may be performed to distinguish between nonviable intrauterine and extra uterin pregnancies. It is not necessary to wait 48 hours for a repeat HCG (1). In this study, by determining the cut-off level of 15 ng/ml for progesterone, and 950 pg/ml for estradiol, the sensitivity of single measurement of serum progesterone level was 100% and specificity was 98%. The sensitivity of single measurement of serum estradiol was 95% and its specificity was 93%. It is not possible to define a cut off discriminatory value of p and E2 that completely separates ectopic from NIUP but the addition of these assays to the work-up of a patient with suspected Ep may facilitate the earlier diagnosis of EP (10, 11).
Acknowledgment
We acknowledge Dr. M. Ghojazadeh, Ph.D. and Dr. R. Todehzaim, Ph.D. for their assistance with coordination of data and outcome results.
Full-Text: (290 Views)
Introduction
Ectopic pregnancy is a potentially life-threatening condition in which the embryo implants outside the uterine endometrial cavity. There was dramatic advances in the diagnosis and treatment of this potentially fatal condition last few decades. With earlier diagnosis, the prognosis for ectopic pregnancy has shifted from a grave, life threatening disease to a more benign condition. The treatment goal also shifted from preventing mortality to reducing morbidity and preserving fertility. To reduce maternal mortality and morbidity, early recognition of ectopic pregnancy is critical (1, 2).
History and physical examination may or may not provide useful diagnostic information. The accuracy of initial clinical evaluation is less than 50%. Additional tests are frequently required to differentiate early viable intrauterine pregnancy with suspected ectopic or abnormal intrauterine pregnancy (3, 4).
Human chorionic gonadotropin (HCG), is a glycoprotein made by placental syncytiotrophoblast (1-5). It is detectable in plasma of pregnant women about 7.5 to 9.5 days after the midcycle surge of LH (5). Therefore, the level of HCG in blood increases rapidly with maximal level of 50000-100000 mlu/ml attained at about 8-10 weeks of gestation (5,6). Nonetheless, HCG is present in the plasma and urine of probably all women with ectopic pregnancies, albeit generally in lower concentration than in women with normal pregnancies of comparable stages, because of the ectopic implantation, disruption of trophoblasts by hemorrhage, or embryonic death (4,5,7). Progesterone is largely produced by the corpus luteum until about 10 weeks of gestation. In the first 5-6 weeks of pregnancy, HCG stimulation of the corpus luteum results in the daily secretion of about 25 mg of progesterone and 0.5 mg of estradiol. Although estrogen levels begin to increase at 4-5 weeks due to placental secretion, progesterone production by the placenta does not significantly increase until about 10-11 weeks after ovulation (6). A single serum progesterone measurement in early gestation has been found by several groups to be of great use in differentiating an ectopic from an intrauterine gestation (8, 9). However, the diagnostic value of simple E2 and P in the patients with EPs could not identify a discriminatory cut-off value because there was a considerable overlap in serum P and E2 between the patients with intrauterine pregnancy and ectopic pregnancy (10,11).
Materials and methods
This case-control study was performed in Alzahra Educational Treatment Center. The study group included 43 women with symptoms or ultrasound finding of ectopic pregnancy. Which was confirmed by laparascopy or laparatomy in all cases. The controls were 42 women of normal intrauterine pregnancy of similar gestational age as assessed by menstrual dates and confirmed by ultrasound scans. All women gave informed consent to the study, which had been approved by the local institutional review board.
Blood samples for the measurement of betasubunit human chorionic gonadotropin, estradiol and progesterone were drawn in all the women upon admission. Exdra blood sample was drawn for measurement of ßHCG 24 hours after admission. Women with hemodynamically unstable status were excluded. From the study Serum level of ßHCG were measured by Radio Immuno Assay (RIA- incstar kit), progesterone by Enzyme Linked Immuno Sorbent Assay (ELISA- pantex kit), and estradiol by (RIA- analyze kit). Sample size calculations, assuming 80% power and 0.05 type I error to detect mean differences, indicated the need for at least 41 patients in each group. SPSS.13/win statistical software was used for analyzing the data. Data were presented as mean±standard deviation. A parametric independent sample t test was used to compare differences between two groups. Level of statistical significance was set at p<0.05. By determining cut-off levels of these parameters the efficiency and sensitivity of each in prediction of ectopic pregnancy were estimated.
Results
In this study, no substantial differences were noted in descriptions of the two groups regarding maternal age (Table 1). Study cases with suspicious ectopic pregnancy had a positive pregnancy test, lower abdominal pain, and vaginal bleeding. Women with normal intrauterine pregnancy (control group) had no evidence of abortion. The mean serum level of ßHCG was 940 ± 552 miu/ml in the case group and 4620 ± 2030 miu/ml in the control group (p<0.0005) (Table 2). The average rate of ßHCG rising was 8.2 % for 24 hours in the patients with ectopic pregnancy and 32.8% for 24 hours in the women with normal intrauterine pregnancy. The mean serum level of progesterone and estradiol in patients with ectopic pregnancy (5.83 ± 3.41 ng/ml, 593± 237 pg/ml, respectively) were significantly lower than in women with normal intrauterine pregnancy (24.8 ± 6.08 ng/ml, 1627 ± 433 pg/ml, respectively) (p<0.0005).
Serum ßHCG level had 91% sensitivity and 85% specifity at a cut-off value of 2000 miu/ml in diagnosis of ectopic pregnancy. Our results showed that ßHCG rising with 80% sensitivity and 93% specificity at a cut-off value of 30% can use for diagnosis. Serum level of progesterone had the greatest sensitivity (100%) and specificity (98%) at a cut-off value of 15 ng/ml. While serum level of estradiol showed 95% sensitivity and 93% specificity at a cut-off value of 950 pg/m. However we could not identify a discriminatory cut-off value because there was a considerable overlap in serum P and E2 levels between the patients with EP and NIUP (10).
Discussion
During the past decade, as modern refinements for identification of ectopic pregnancy have evolved, the majority of these cases (perhaps 80%) are diagnosed before rupture. Coincidentally, the death rate has decreased appreciably (5). The intial step of diagnosis of ectopic pregnancy is to screen for presence of pregnancy (1). Today, early diagnosis of ectopic pregnancy is possible with highly sensitive and rapid ß subunit of human chorionic gonadotropin assay with the aid of vaginal ultrasound (1,2) if ß-HCG is not detected with the use of radioimmunoassay of serum, the diagnosis of ectopic pregnancy can, with a rare exception, be ruled out (8). The early diagnosis is more beneficial from the point of possibility of medical therapy or conservative surgery (12). According to the results of this study, significant differences between serum ßHCG levels in case and control group were noticed (p<0.0005). The specificity and sensitivity of single HCG measurement in detection of ectopic pregnancy at the cut-off level of 2000 mlu/ml were 91% and 85% respectively. Although about 85% of women with ectopic pregnancy have serum HCGlevels lower than those seen in normal pregnancy at a similar age. However a single quantitative HCG assay can not be used for diagnosis of ectopic pregnancy because the actual dates of ovulation and conception are not known for most women (8). There is considerable overlap of values between normal and abnormal pregnancies at a given gestational age (3).
In normal pregnancies with early gestational age, the level of circulating HCG doubles about every 2 days. In our study the mean percentages of ßHCG rising in EP and NIUP after 24 hours were 8.2 and 32.8, respectively. Serial measurement of HCG with 80% sensitivity and 93% specificity at the cut off level of 30% is the great assistance in early diagnosis of unruptured ectopic pregnancy. In abnormal pregnancies (ectopic pregnancy and those destined to abort), HCG level usually doesn't increase at the same rate.
However, a differentiation between increasing rate of HCG in women with an ectopic pregnancy is similar to an impending intrauterine abortion (8). In these cases the measurement of serum progestrone is helpful. A serum progesterone level less than 5 ng/ml is highly suggestive of an abnormal pregnancy, but it is not 100% predictive. The risk of normal pregnancy with a serum progesterone level less than 5.0 ng/ml is approximately 1/1500 (3). A single progesterone or estradiol measurement may suggest non viability of a pregnancy without precise knowledge of gestational age, even when the serum HCG is below the discriminatory zone (1).
When the serum progesterone level is less than 2.5 ng/ml, uterin curettage may be performed to distinguish between nonviable intrauterine and extra uterin pregnancies. It is not necessary to wait 48 hours for a repeat HCG (1). In this study, by determining the cut-off level of 15 ng/ml for progesterone, and 950 pg/ml for estradiol, the sensitivity of single measurement of serum progesterone level was 100% and specificity was 98%. The sensitivity of single measurement of serum estradiol was 95% and its specificity was 93%. It is not possible to define a cut off discriminatory value of p and E2 that completely separates ectopic from NIUP but the addition of these assays to the work-up of a patient with suspected Ep may facilitate the earlier diagnosis of EP (10, 11).
Acknowledgment
We acknowledge Dr. M. Ghojazadeh, Ph.D. and Dr. R. Todehzaim, Ph.D. for their assistance with coordination of data and outcome results.
Type of Study: Original Article |
References
1. Kim HH, Fox JH. The fallopian tube and ectopic pregnancy In: Ryan KJ, Berkowitz RS, Barbieri RL, Dunaif A. Kistner's Gynecology and women's health. St.Louis, Missouri: Mosby; 1999: 143-166.
2. Mertz HL, Yalcinkaya TM. Early diagnosis of ectopic pregnancy. Duse use of a strict algoritm decrease the incidence of tubal rupture. J reprod Med 2001; 46: 29-33.
3. Stovall TG. Early pregnancy loss and ectopic pregnancy In: Berek Jonathan S. Novak's Gynecology. 13th edition. Philalelphia:Lippincott Williams and Wilkins 2002: 507-548.
4. Kohn MA, Kerr K, Malkevich D, O'Neil N, Kerr MJ, Kaplan BC. ßHCG levels and the likelihood ectopic pregnancy in emergency department patients with abdominal pain or vaginal bleeding. Acad Emerg Med 2003; 10: 119-126. [DOI:10.1197/aemj.10.2.119]
5. Cunmingham FG, Leveno KJ, Steven LB, Hauth JC, Gilstrap LC, Wenstrom KD. Williams Obstetrics, 22nd edition,USA:McGraw-Hill 2005:253-272.
6. Speroff L, Fritz Marc A. Clinical Gynecologic Endocrinology and infertility Lippincott, Philadelphia. Lippincutt, Williams & Wilkins, 7th edition 2005; 259-318,1275-1302.
7. Borrelli PT, Butler SA, Docherty SM, Staite EM, Borrelli AL, Iles RK. Human Chorionic Gonadotropin Isoform in the diagnosis of ectopic pregnancy. Clin Chem 2003:13. [DOI:10.1373/clinchem.2003.022095]
8. Rock John A, Jones Howard W. Telinde's operative Gynecology In: Mark A, Rock John A. Ectopic pregnancy, Damariq. USA: Lippincott Williams & Wilkins:9th edition;2003; 507-537.
9. Graig ZG, Ramery Jm, Rochowiak MW, Brown LH, Teilelbaum H. Serum estradiol in the differential diagnosis of ectopic pregnancy. JAM osteopath Assoc 1996; 96:461-464. [DOI:10.7556/jaoa.1996.96.8.461]
10. Kuscu E, Vicdan K, Turhan No , Oguz S, Zorlu G, Gokmen O. The hormonal profit in ectopic pregnancy. J Park Med assoc 1994; 44: 45-47.
11. Kuscu E, Vicdan K, Turhan No Oguz S, Zorlu G, Gokmen O. The hormonal profit in ectopic pregnancy. Mater Med Pol 1993; 25: 149-152.
12. Mishell DR. Ectopic pregnancy In: Mishell DR, Morton A Stenckever MA, Droegemueler W, Herbst AL. Comprehensive Gynecology, 3rd edition, St.Louis, Missouri:Mosby; 1997: 431-467.
13. Dart R, Dart L, Segal M, Page C, Brancato J. The ability of a single serum progesterone value to identify abnormal pregnancies in patients with beta-human chorionic gonadotropin values less than 1,000 mIU/mL. Acad Emerg Med 1998; 5:304-309. [DOI:10.1111/j.1553-2712.1998.tb02709.x]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
