
International Journal of
Reproductive Biomedicine
Fri, Jun 12, 2026
[Archive]
Volume 20, Issue 10 (October 2022)
IJRM 2022, 20(10): 841-850 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadat Eshaghi F, Dehghan Tezerjani M, Ghasemi N, Dehghani M. Association Study of ESR1 rs9340799, rs2234693, and MMP2 rs243865 Variants in Iranian Women with Premature Ovarian Insufficiency: A case-control study. IJRM 2022; 20 (10) :841-850
URL: http://ijrm.ir/article-1-2370-en.html
URL: http://ijrm.ir/article-1-2370-en.html



1- Department of Genetics, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2- Abortion Research Center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3- Medical Genetics Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,dehghani.dr@gmail.com
2- Abortion Research Center, Yazd Reproductive Sciences Institute, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3- Medical Genetics Research Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. ,
Keywords: Matrix metalloproteinase-2, Estrogen receptor alpha, Primary ovarian insufficiency, Female infertility.
Full-Text [PDF 851 kb]
(1365 Downloads)
| Abstract (HTML) (2069 Views)
1. Introduction
Primary ovarian insufficiency (POI) is a rare disease with hyper gonadotrophic amenorrhea in women before the age of 40 yr {Chen, 2020 #1}(1). It occurs in around 1/1000 women < 30 yr and 1/10000 < 20 yr (2). The main causes of POI in most women are still unknown; however, genetic reasons (chromosomal abnormalities and gene mutations), infections, and metabolic and autoimmunity disorders are associated with developing POI (3, 4). This condition is clinically characterized by amenorrhea, decreased levels of estradiol (E2) and anti-mullerian hormone (AMH); and an increased level of luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Several studies suggested a possible association between matrix metallopeptidase 2 (MMP2) genetic variants and vulnerability to POI. This gene on chromosome 16q13-21 has 17 exons and belongs to the MMP2 gene family involved in breaking down signal transduction molecules and extracellular matrix components (5-7). The expression of MMP2 has been identified in both the testis and ovary. MMP2 is localized to the oogonium/oocyte cytoplasm in the ovary, with varying intensities. In addition, it was detected in the ovarian stroma (8).
Different studies have also investigated the association of polymorphism in the estrogen receptor 1 (ESR1) gene with developing POI (9); however, their results are controversial in different populations. This gene located on 6q25.1-q25.2 with 23 exons, encodes a ligand-activated transcription factor as well as an estrogen receptor. The receptor has a fundamental role in the pathogenesis of endometrial cancer, breast cancer, and osteoporosis. rs2234693 and rs9340799 polymorphism in ESR1 is the most studied variant in women suffering from POI. Although rs2234693 polymorphism is located in the intronic section of the ESR1 gene, it was reported to be associated with normal menopause in Korean and Dutch women (10). This polymorphism was also investigated in Chinese, Brazilian, and European women, and the results revealed a significant association with the onset of POI (11-13). The other polymorphism in this gene, rs9340799, decreases the risk of developing POI in the Korean population. However, no association of this polymorphism was found with Chinese and Brazilian women (11, 12, 14).
This study aimed to evaluate the association of rs243865 polymorphism in the MMP2 gene and rs2234693 and rs9340799 polymorphisms in the ESR1 gene with the risk of POI in women under 35 yr.
2. Materials and Methods
2.1. Sample collection
150 women with POI and 150 healthy women as a control group were involved in this case-control study. The samples were collected from Yazd Reproductive Sciences Institute, Yazd, Iran from May-October 2020. POI women were selected based on FSH measurements of > 40 mIU/ml; and AMH < 2 ng/ml. Inclusion criteria for healthy participants were negative autoantibodies (anti-ovarian thyroid, antinuclear antibodies), regular menstrual cycles, and at least one live birth. Women with pelvic surgery, positive for autoantibodies, a history of cancer, radiation exposure, and genetic syndrome were excluded.
2.2. Hormonal evaluation
LH, E2, AMH, thyroid stimulating hormone, prolactin, and FSH have been evaluated in both groups using the Pishtaz Teb kit (Pishtaz Teb, Iran) on the Stat Fax system (Awareness Technology, USA). Samples were collected on the 3rd or 4th days of menstrual cycles in the control group.
2.3. DNA extraction and polymerase chain reaction (PCR)
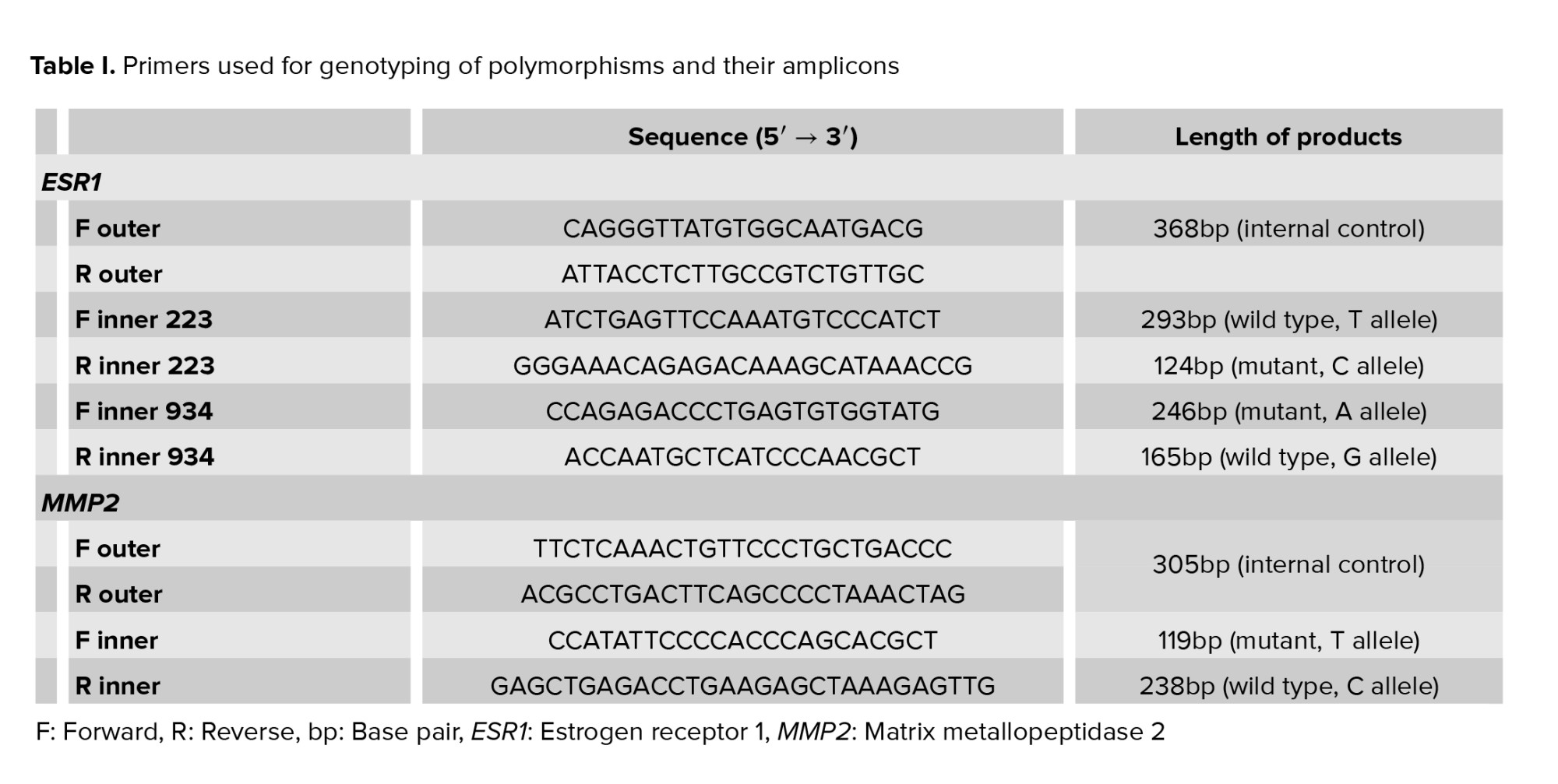
DNA was extracted from blood samples of individuals using a DNA extraction kit (Simbiolab, Iran) according to the manufacturer’s instructions. The quality of the extracted genomic DNA was evaluated using agarose gel electrophoresis, and the quantity of the samples were checked by a Nanodrop (Thermo Scientific, Wilmington, DE). Then, we used Tetra-primer amplification refractory mutation system PCR to genotype the 3 polymorphisms (15, 16) (Table I).
Each vial of PCR for the rs2234693 polymorphism in the ESR1 gene contained 1 ml of DNA, (0.4 μL of FO+0.4 μL RO+1 ml FI+1 μL RI) primers, 12 ml of master mix (Amplicon), and 9.2 μL of water in a final volume of 25 μL. The vial for testing the rs9340799 polymorphism in the ESR1 included 1 μl of DNA, (0.5 μL of FO+0.5 μL RO+1.2 μL FI + 1.2 μL RI) primers, 12 μL of master mix (Amplicon), and 8.6 μL of water in a final volume of 25 μL. The volume of each vial for the rs243865 polymorphism in the MMP2 gene is 10 μL master mix, 0.4 μL external forward primer, 0.4 μL external reverse primer, 0.8 μL internal forward primer, 0.8 μL internal reverse primer, 6.6 ml of water, and 1 μL of DNA in a final volume of 20 μL.
The PCR condition was done by following steps: 95oC for 10 min as initial denaturation, denaturation at 95oC for 30 sec, annealing at 64.5oC (rs243865), 62oC (rs2234693), 61oC (rs9340799) for 30 sec, and extension at 72oC for 30 sec (for 38 cycles) and final extension at 72oC for 5 min. Next, the PCR products were loaded on 2% agarose gel. To check the genotyping quality, we sequenced all polymorphisms in random samples bidirectionally.
2.4. Ethical considerations
The study was approved by the local ethics committee of the Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.MEDICINE.REC.1399.030). Written informed consent was also obtained from all the participants.
2.5. Statistical analysis
The Statistical Package for the Social Sciences, version 21, SPSS Inc, Chicago, Illinois, USA software was applied to analyze the data. For the evaluation of clinical features for healthy and POI individuals, we calculated the p-values by independent 2-sample t test. The difference in genotypes and allele frequency between the control and case groups were also investigated by Fisher’s exact test. To analyze the strength of the association between the genotypes/alleles of the polymorphism and susceptibility to POI, the odds ratio (OR) and their 95% confidence intervals (95% CI) were estimated. Age was considered a covariate, and its effects were removed from the analysis. We considered p-value < 0.05 as a significant value. In addition, an SNPanalyzer (v2) was employed for haplotype and linkage disequilibrium analyses.
3. Results
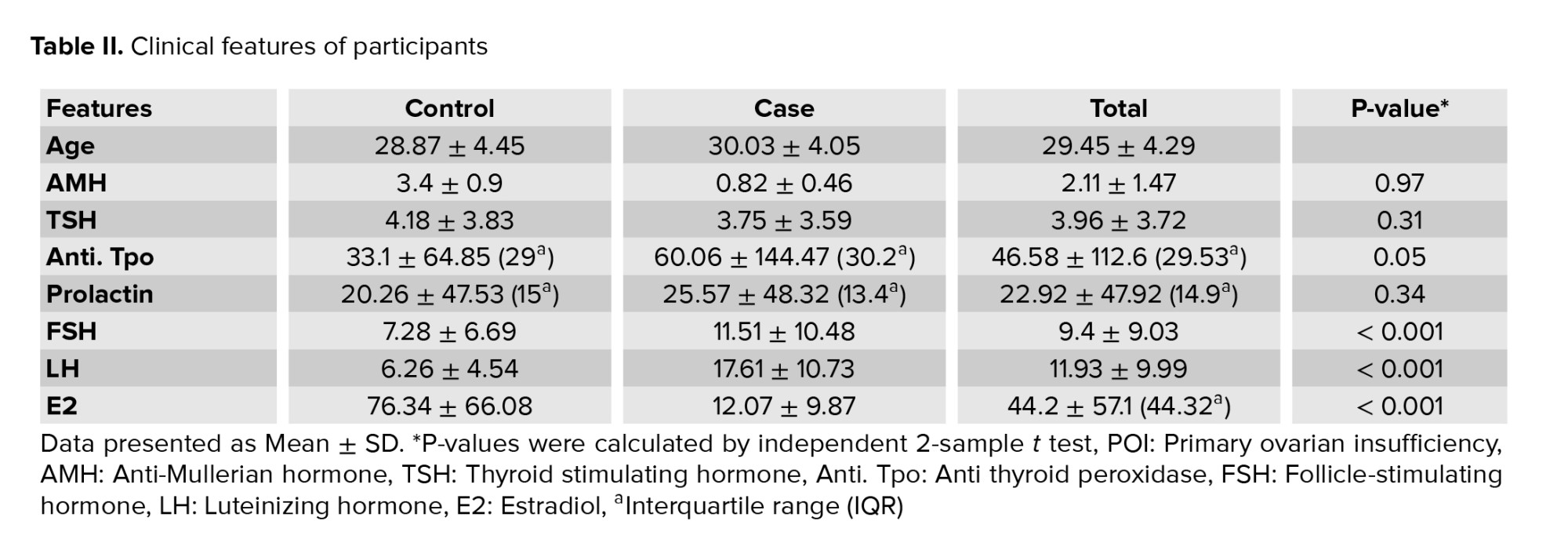
The clinical features and characteristics of the participants are described in table II. The FSH, LH, and E2 showed a significant difference between the case and control groups (p < 0.001). However, no significant differences were found for other clinical features.
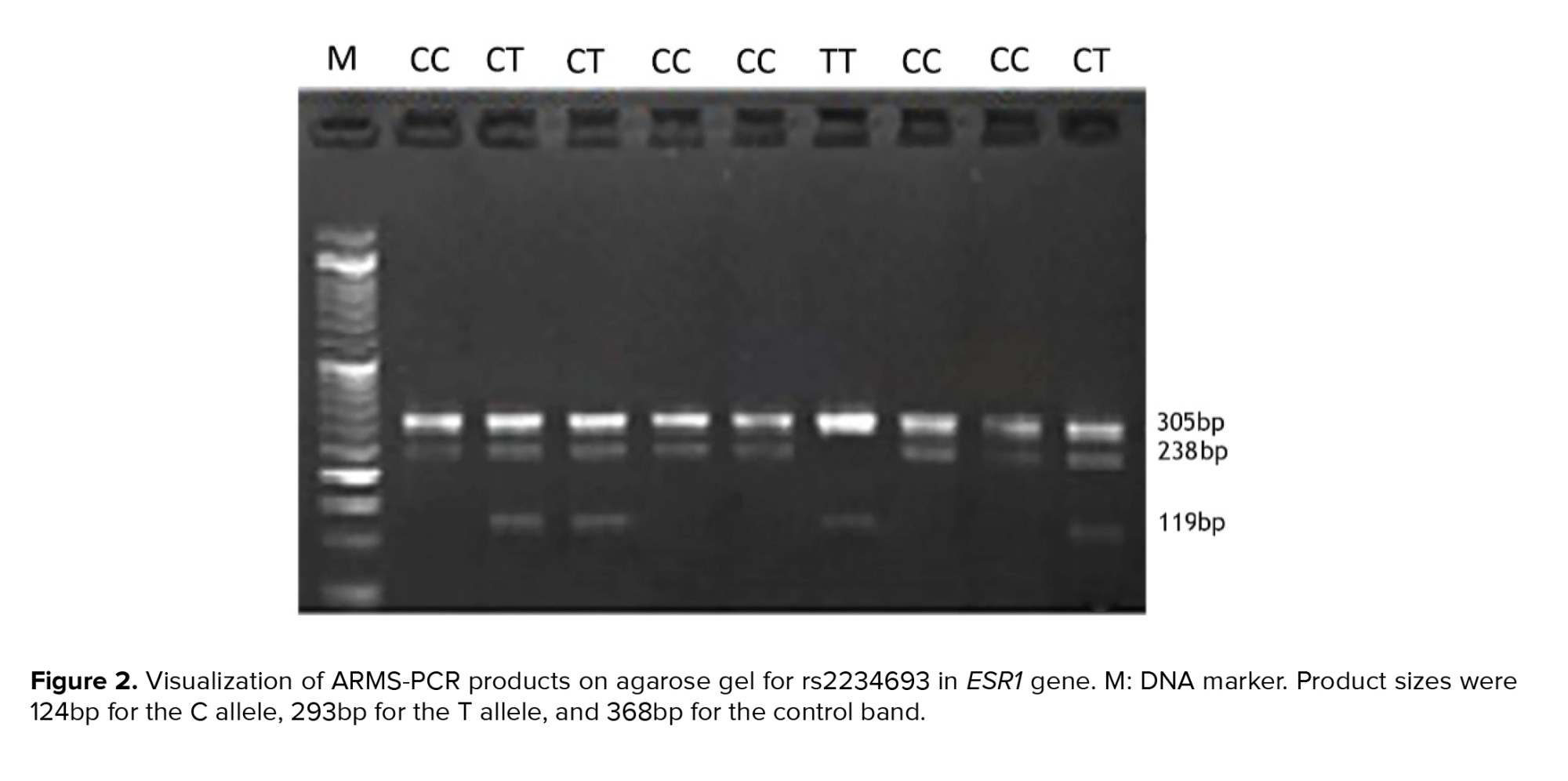
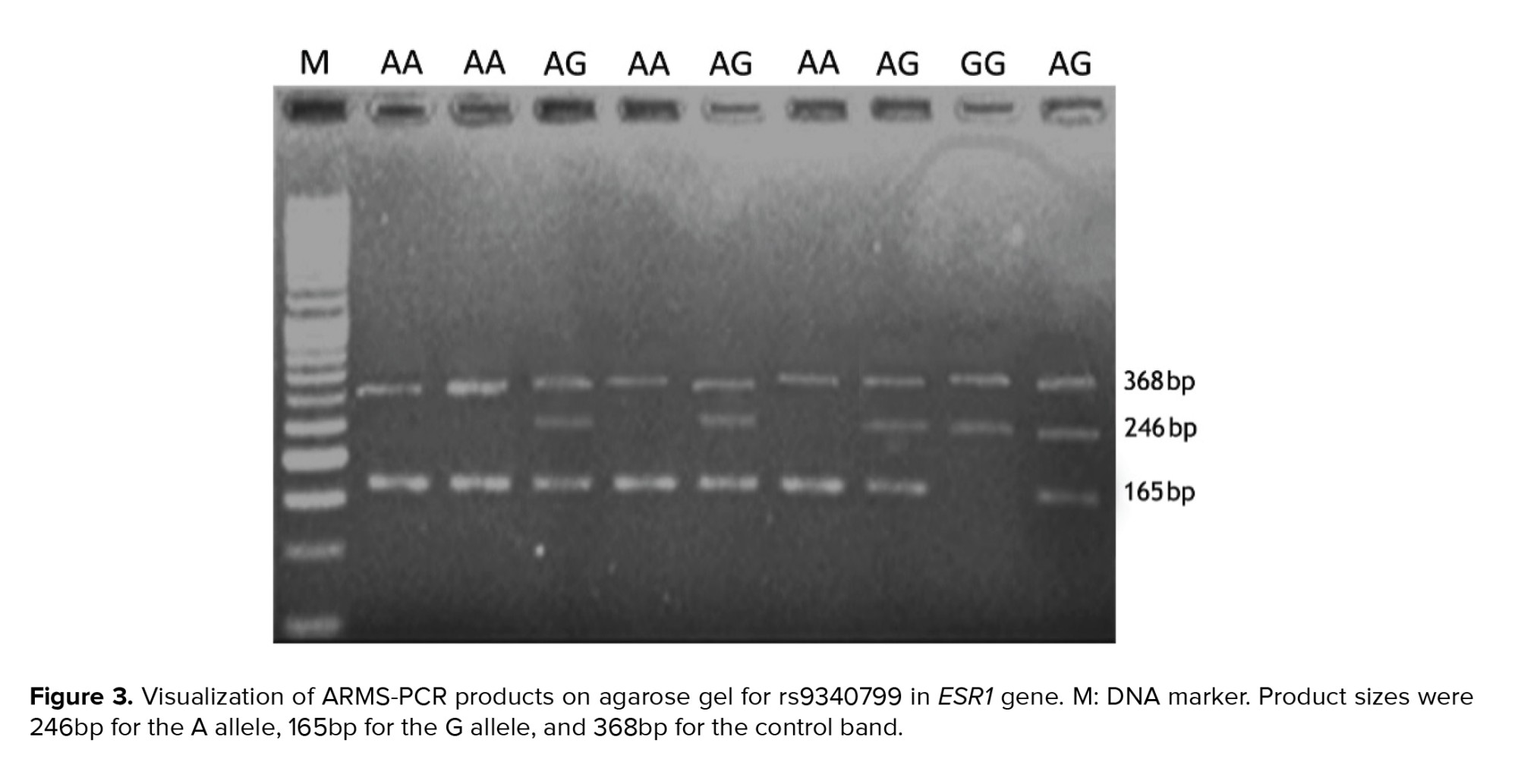
The visualization of amplification refractory mutation system PCR products on agarose gel for MMP2 -rs243865, ESR1-rs2234693, and ESR1-rs9340799 are shown in figures 1, 2, and 3, respectively.
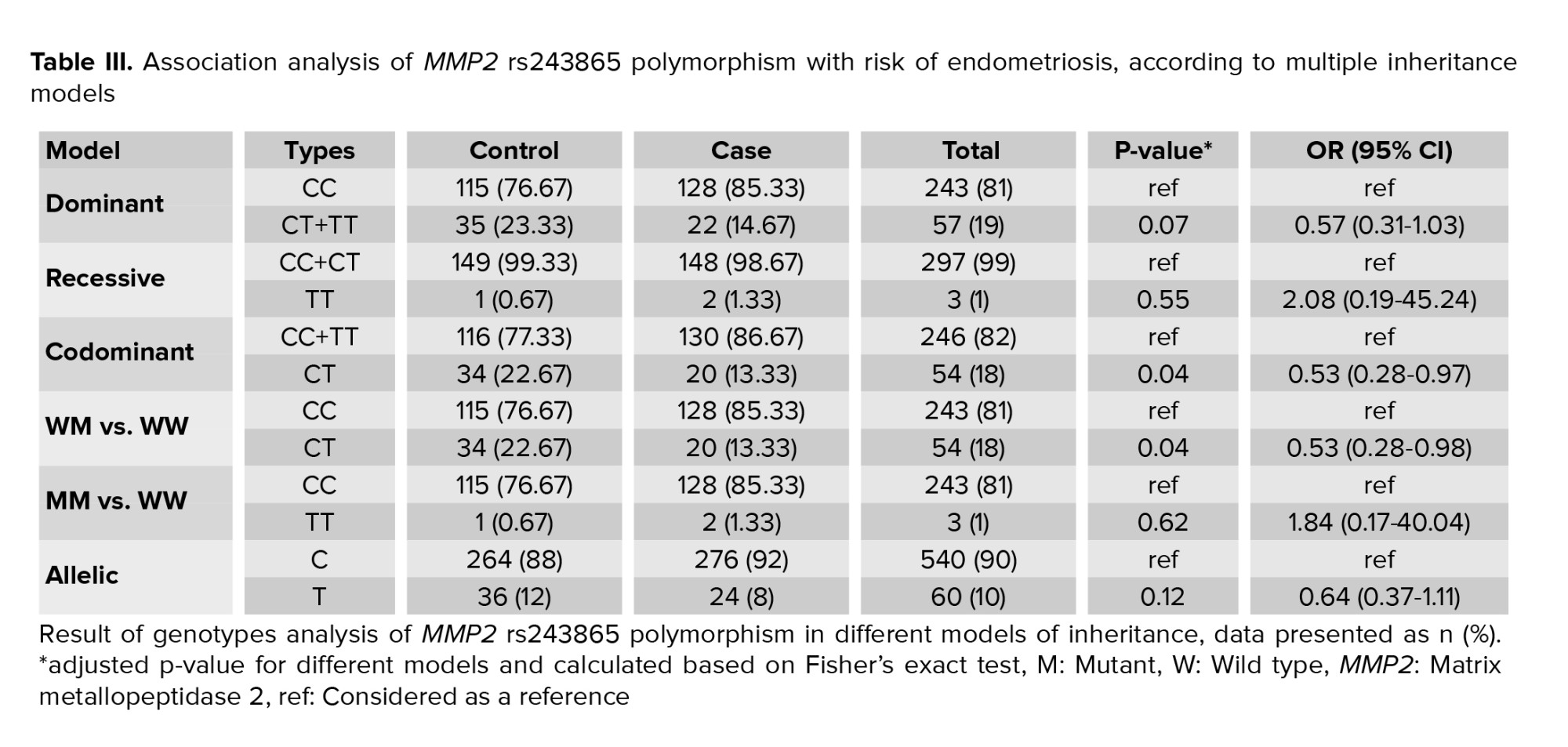
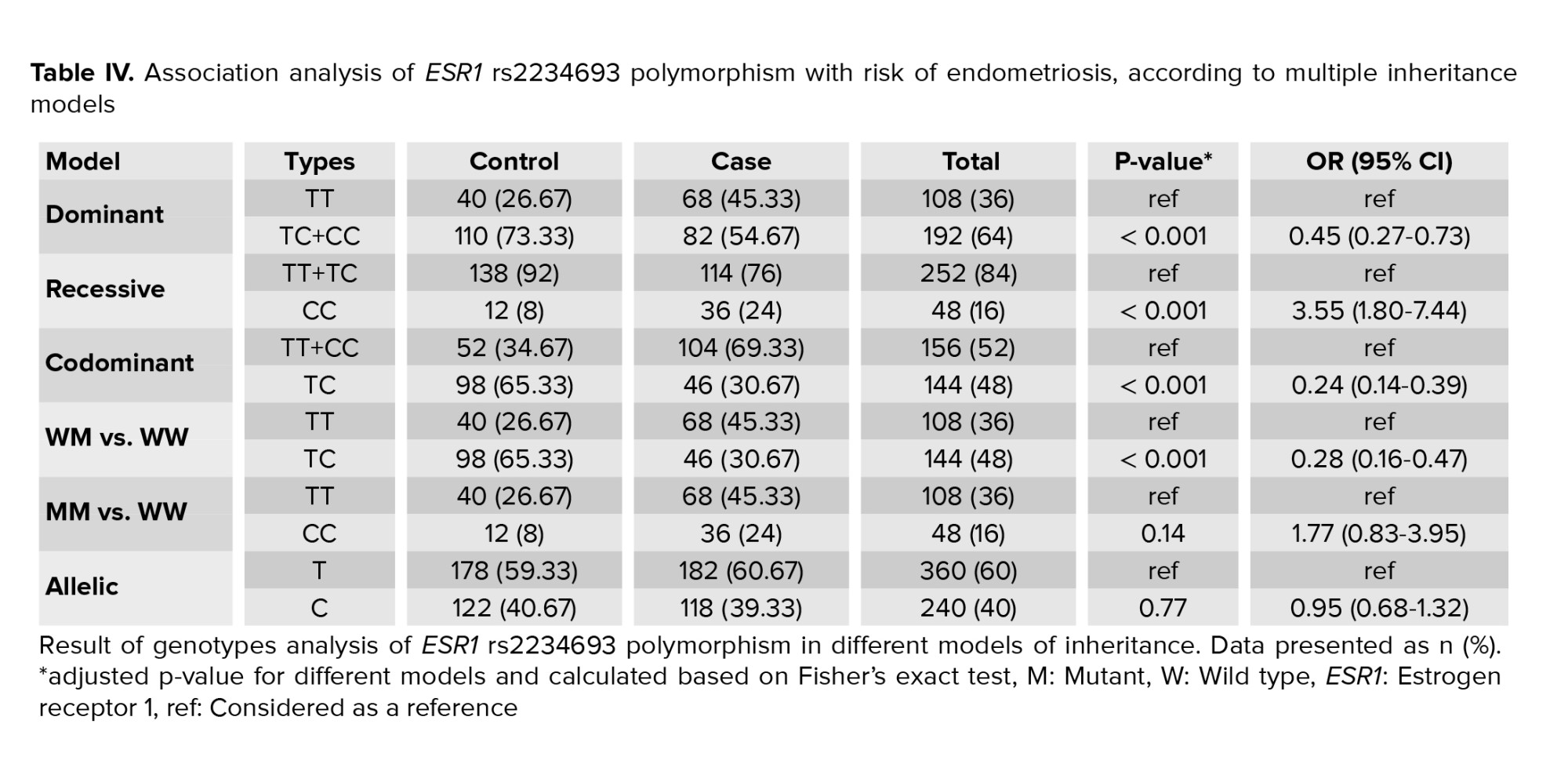
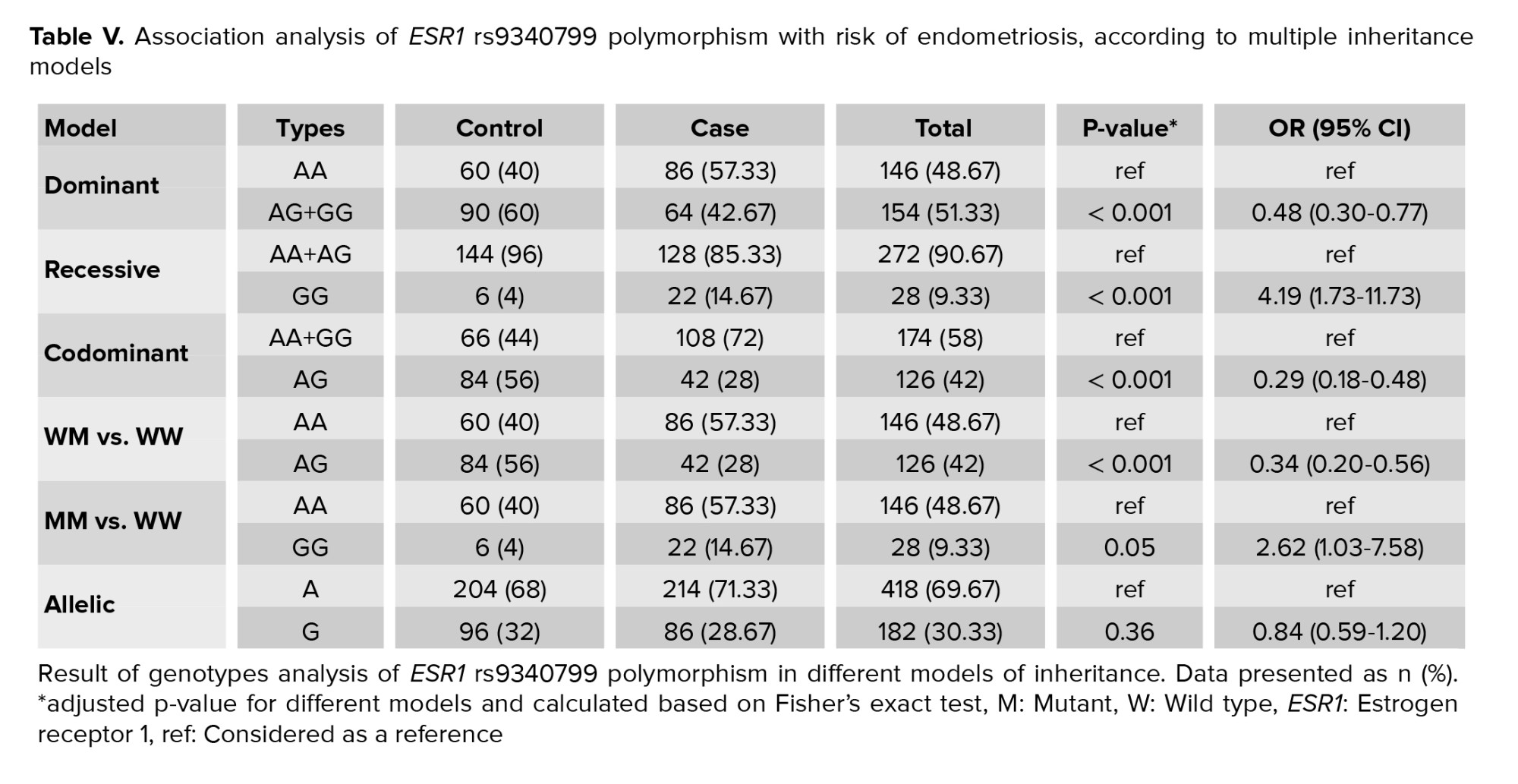
The genotype frequencies and ORs for MMP2 -rs243865, ESR1-rs2234693, and ESR1-rs9340799 are also shown in tables III, IV, and V, respectively. Our study shows the frequency of rs243865 TT, CC genotypes in the MMP2 gene and rs2234693 CC, TT; and rs9340799 GG, AA in the ESR1 gene were more prevalent in the case group compared to the control group. There was a significant association of ESR1 rs2234693 and rs9340799 genotypes with the disease in our population (p < 0.001). No significant association was found for these 3 polymorphisms at the allelic level. Analysis of different models of inheritance revealed that the codominant model (CT vs. CC+TT) and CT vs. CC for rs243865 polymorphism (Table III); and dominant model (TC+CC vs. TT), recessive model (CC vs. TT+TC), codominant model (TC vs. TT+CC) and TC vs. TT (WM vs. WW) for rs2234693 polymorphism (Table IV); and dominant model (AG+GG vs. AA), recessive model (GG vs. AA+AG), codominant model (AG vs. AA+GG) and AG vs. AA (WM vs. WW) for rs9340799 polymorphism (Table V) were significantly different between the case and control group.
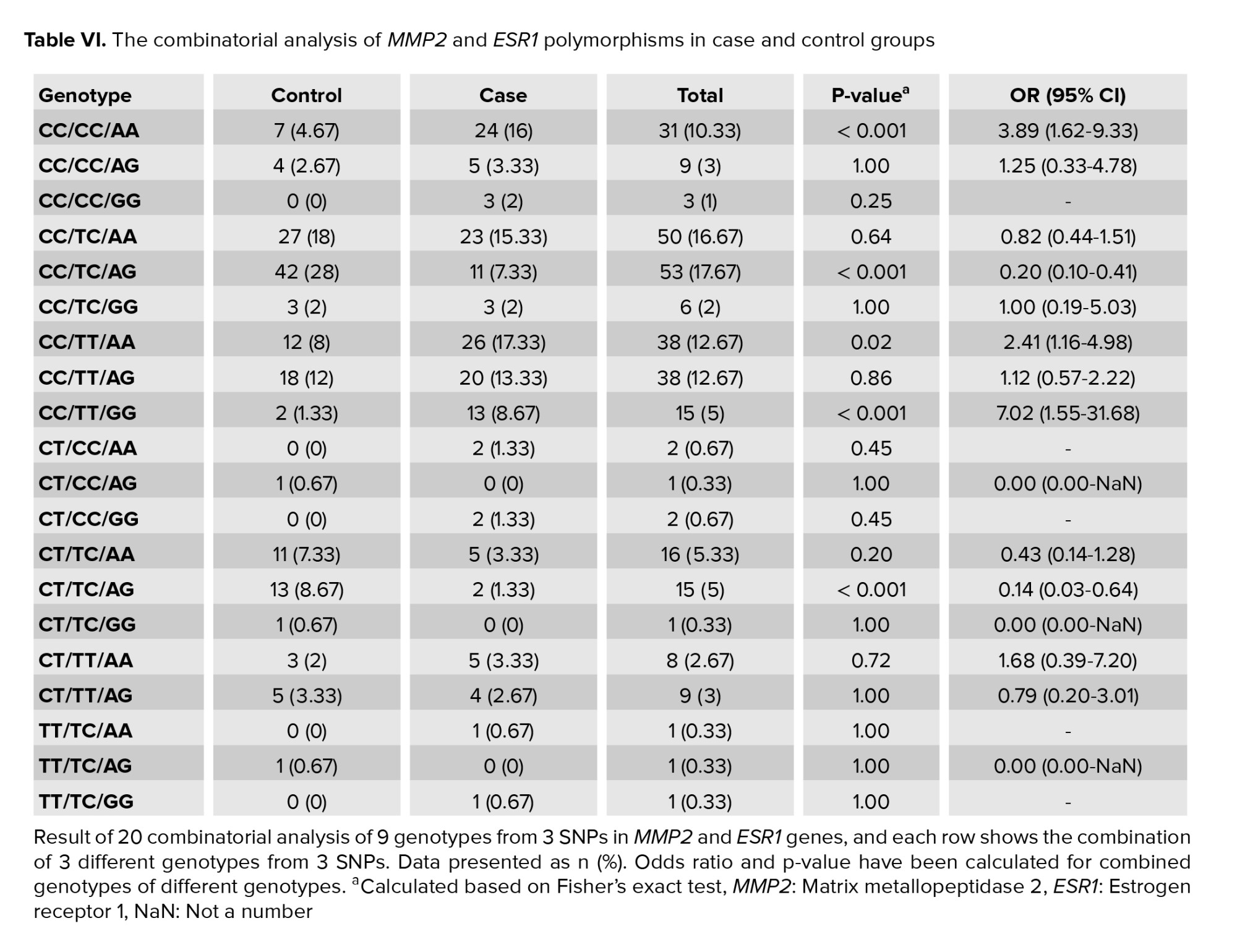
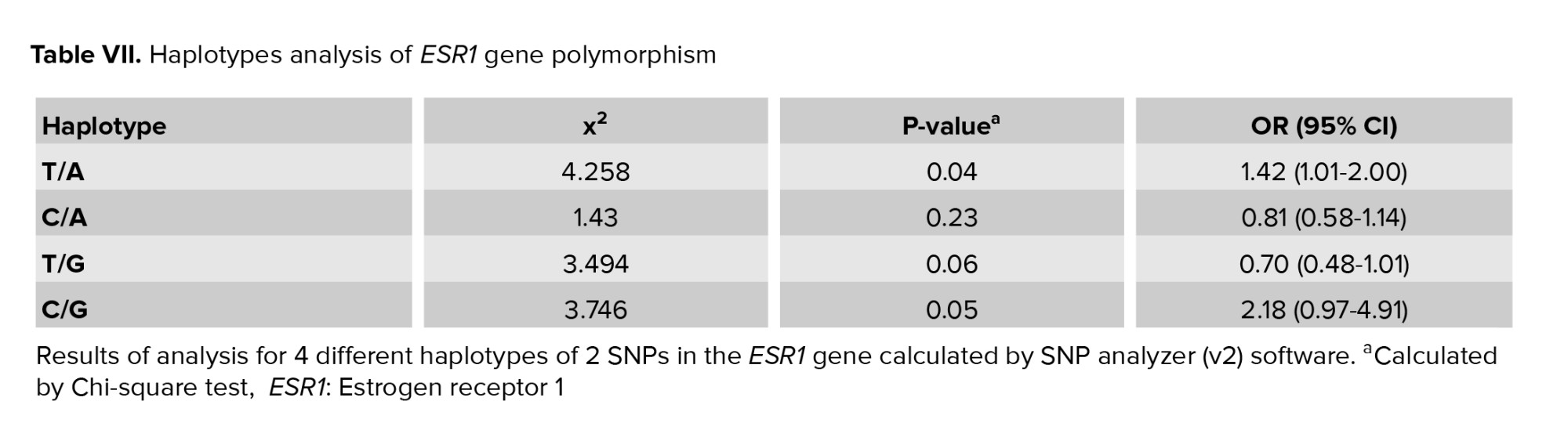
The combinational analysis also revealed that rs243865 CC/rs2234693 CC/rs9340799 AA, rs243865 CC/rs2234693TC/rs9340799 AG, rs243865 CC/rs2234693 TT/rs9340799 AA, rs243865 CC/rs2234693 TT/rs9340799 GG, and rs243865 CT/rs2234693 TC/rs9340799 AG genotypes were significantly associated with the susceptibility to POI in our population (table VI). Among the 4 haplotypes for 2 polymorphisms in the ESR1 gene, rs2234693T/rs9340799A haplotype was found to be associated with conferring risk to POI (p = 0.04, OR = 1.42) (Table VII). Pairwise LD analysis also showed a moderate LD (D՛:30) for ESR1 -351 A/G (rs9340799) and ESR1 -397 T/C (rs2234693) polymorphisms in our population.

4. Discussion
Like other multifactorial diseases, POI originated from various genetics and environmental factors (1). Therefore, we performed a case-control study to investigate the possible association of 3 polymorphisms in the MMP2 and ESR1 gene and susceptibility to POI in Iranian women. Our study showed a significant association of ESR1 rs2234693 and rs9340799 genotypes with the disease in our population. In addition, the codominant model (CT vs. CC+TT) and CT vs. CC of MMP2 rs243865 polymorphism were found to be correlated with the risk of POI. No allelic association was found for these 3 polymorphisms. In the ESR1 gene, rs2234693T/rs9340799A haplotype was also associated with developing vulnerability to POI.
The ESR1 gene encoding estrogen α receptor is one of the fundamental molecules in the human reproductive system (17). Estrogen has a positive or negative impact on the regulation of gonadotropin secretion, folliculogenesis, and ovulation. Therefore, any variations in its gene may affect the time of menarche or menopause, resulting in developing POI (17, 18). In addition, the polymorphisms in this gene have been investigated in different diseases related to females, such as breast cancer, endometriosis, and uterine fibroid (19-21). Although some studies revealed the positive association of ESR1 -397 T/C (rs2234693) and -351 A/G (rs9340799) with POI (22, 23), others showed conflicting results (24, 25). Similar to our study, a study on Caucasian women revealed a positive association of these 2 polymorphisms with POI (23). In addition, a significant association of these 2 polymorphisms and their haplotype with POI was found in the Chinese population (22). However, a meta-analysis study showed no association of these polymorphisms with susceptibility to POI (26). In contrast to our study, a study on Korean women also found no association of ESR1 -397 T/C (rs2234693) with the disease (27). Following our study, another meta-analysis investigating these 2 polymorphisms (3 case-control studies with 1396 subjects) revealed a significant association of ESR1 -397 T/C (rs2234693) polymorphism with POI in the Asian population in all models; however, no significant association was found for any models in the European population. In terms of -351 A/G (rs9340799) polymorphism, this meta-analysis showed no association overall, but under dominant model was associated with POI in the Asian population (18). A functional study also indicated that CC genotypes of rs2234693 significantly reduces the ESR1 expression level (28). C allele decreases the binding of AP-4 as a transcriptional activator to the sense strand and the binding of ZNF238 as a transcriptional repressor to the antisense strand, resulting in unstable ESR1 mRNA (29, 30).
MMP2 is involved in the AMH regression pathway and indirectly reduces AMH in POI women. Genetic variants in this gene, including 1306C > T, may affect the expression of this gene, and any changes in its expression can lead to ovarian structural and follicular growth changes (7). A functional study showed that the T allele in the SP1 sequence, a consensus sequence in the MMP2 promoter (-1306 site; -1307C(C/T) ACC-1303) can disrupt the activity of the promoter and lower MMP2 gene expression (31). Therefore, evaluating the polymorphism can pave the way for finding the disease pathogenesis and genes involved in its development. There is only one study investigating the association of MMP2 -1306C > T rs243865 with POI. Contrary to our study in which only the CT vs. CC model is related to POI, Kim and colleagues indicated that MMP2 -1306CT + TT was associated with POI susceptibility (7).
To the best of our knowledge, this is the first study investigating the association of these 3 polymorphisms with POI in the Iranian population. Although, more functional studies with more samples and more polymorphisms in these genes can provide more strong results.
5. Conclusion
This study indicated that rs2234693 and rs9340799 polymorphisms of the ESR1 gene and MMP2 -1306C > T rs243865 in the codominant model are significant in relation to vulnerability to POI among Iranian women. Finding genotypes in susceptibility to POI would help detect POI and provide precious information for counseling of pregnancy loss in the young couple.
Acknowledgments
The authors thank all the patients and individuals who attended this study.
Conflict of Interest
The authors declare that they do not have any conflict of interest.
Full-Text: (327 Views)
1. Introduction
Primary ovarian insufficiency (POI) is a rare disease with hyper gonadotrophic amenorrhea in women before the age of 40 yr {Chen, 2020 #1}(1). It occurs in around 1/1000 women < 30 yr and 1/10000 < 20 yr (2). The main causes of POI in most women are still unknown; however, genetic reasons (chromosomal abnormalities and gene mutations), infections, and metabolic and autoimmunity disorders are associated with developing POI (3, 4). This condition is clinically characterized by amenorrhea, decreased levels of estradiol (E2) and anti-mullerian hormone (AMH); and an increased level of luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Several studies suggested a possible association between matrix metallopeptidase 2 (MMP2) genetic variants and vulnerability to POI. This gene on chromosome 16q13-21 has 17 exons and belongs to the MMP2 gene family involved in breaking down signal transduction molecules and extracellular matrix components (5-7). The expression of MMP2 has been identified in both the testis and ovary. MMP2 is localized to the oogonium/oocyte cytoplasm in the ovary, with varying intensities. In addition, it was detected in the ovarian stroma (8).
Different studies have also investigated the association of polymorphism in the estrogen receptor 1 (ESR1) gene with developing POI (9); however, their results are controversial in different populations. This gene located on 6q25.1-q25.2 with 23 exons, encodes a ligand-activated transcription factor as well as an estrogen receptor. The receptor has a fundamental role in the pathogenesis of endometrial cancer, breast cancer, and osteoporosis. rs2234693 and rs9340799 polymorphism in ESR1 is the most studied variant in women suffering from POI. Although rs2234693 polymorphism is located in the intronic section of the ESR1 gene, it was reported to be associated with normal menopause in Korean and Dutch women (10). This polymorphism was also investigated in Chinese, Brazilian, and European women, and the results revealed a significant association with the onset of POI (11-13). The other polymorphism in this gene, rs9340799, decreases the risk of developing POI in the Korean population. However, no association of this polymorphism was found with Chinese and Brazilian women (11, 12, 14).
This study aimed to evaluate the association of rs243865 polymorphism in the MMP2 gene and rs2234693 and rs9340799 polymorphisms in the ESR1 gene with the risk of POI in women under 35 yr.
2. Materials and Methods
2.1. Sample collection
150 women with POI and 150 healthy women as a control group were involved in this case-control study. The samples were collected from Yazd Reproductive Sciences Institute, Yazd, Iran from May-October 2020. POI women were selected based on FSH measurements of > 40 mIU/ml; and AMH < 2 ng/ml. Inclusion criteria for healthy participants were negative autoantibodies (anti-ovarian thyroid, antinuclear antibodies), regular menstrual cycles, and at least one live birth. Women with pelvic surgery, positive for autoantibodies, a history of cancer, radiation exposure, and genetic syndrome were excluded.
2.2. Hormonal evaluation
LH, E2, AMH, thyroid stimulating hormone, prolactin, and FSH have been evaluated in both groups using the Pishtaz Teb kit (Pishtaz Teb, Iran) on the Stat Fax system (Awareness Technology, USA). Samples were collected on the 3rd or 4th days of menstrual cycles in the control group.
2.3. DNA extraction and polymerase chain reaction (PCR)
DNA was extracted from blood samples of individuals using a DNA extraction kit (Simbiolab, Iran) according to the manufacturer’s instructions. The quality of the extracted genomic DNA was evaluated using agarose gel electrophoresis, and the quantity of the samples were checked by a Nanodrop (Thermo Scientific, Wilmington, DE). Then, we used Tetra-primer amplification refractory mutation system PCR to genotype the 3 polymorphisms (15, 16) (Table I).
Each vial of PCR for the rs2234693 polymorphism in the ESR1 gene contained 1 ml of DNA, (0.4 μL of FO+0.4 μL RO+1 ml FI+1 μL RI) primers, 12 ml of master mix (Amplicon), and 9.2 μL of water in a final volume of 25 μL. The vial for testing the rs9340799 polymorphism in the ESR1 included 1 μl of DNA, (0.5 μL of FO+0.5 μL RO+1.2 μL FI + 1.2 μL RI) primers, 12 μL of master mix (Amplicon), and 8.6 μL of water in a final volume of 25 μL. The volume of each vial for the rs243865 polymorphism in the MMP2 gene is 10 μL master mix, 0.4 μL external forward primer, 0.4 μL external reverse primer, 0.8 μL internal forward primer, 0.8 μL internal reverse primer, 6.6 ml of water, and 1 μL of DNA in a final volume of 20 μL.
The PCR condition was done by following steps: 95oC for 10 min as initial denaturation, denaturation at 95oC for 30 sec, annealing at 64.5oC (rs243865), 62oC (rs2234693), 61oC (rs9340799) for 30 sec, and extension at 72oC for 30 sec (for 38 cycles) and final extension at 72oC for 5 min. Next, the PCR products were loaded on 2% agarose gel. To check the genotyping quality, we sequenced all polymorphisms in random samples bidirectionally.
2.4. Ethical considerations
The study was approved by the local ethics committee of the Shahid Sadoughi University of Medical Sciences, Yazd, Iran (Code: IR.SSU.MEDICINE.REC.1399.030). Written informed consent was also obtained from all the participants.
2.5. Statistical analysis
The Statistical Package for the Social Sciences, version 21, SPSS Inc, Chicago, Illinois, USA software was applied to analyze the data. For the evaluation of clinical features for healthy and POI individuals, we calculated the p-values by independent 2-sample t test. The difference in genotypes and allele frequency between the control and case groups were also investigated by Fisher’s exact test. To analyze the strength of the association between the genotypes/alleles of the polymorphism and susceptibility to POI, the odds ratio (OR) and their 95% confidence intervals (95% CI) were estimated. Age was considered a covariate, and its effects were removed from the analysis. We considered p-value < 0.05 as a significant value. In addition, an SNPanalyzer (v2) was employed for haplotype and linkage disequilibrium analyses.
3. Results
The clinical features and characteristics of the participants are described in table II. The FSH, LH, and E2 showed a significant difference between the case and control groups (p < 0.001). However, no significant differences were found for other clinical features.
The visualization of amplification refractory mutation system PCR products on agarose gel for MMP2 -rs243865, ESR1-rs2234693, and ESR1-rs9340799 are shown in figures 1, 2, and 3, respectively.
The genotype frequencies and ORs for MMP2 -rs243865, ESR1-rs2234693, and ESR1-rs9340799 are also shown in tables III, IV, and V, respectively. Our study shows the frequency of rs243865 TT, CC genotypes in the MMP2 gene and rs2234693 CC, TT; and rs9340799 GG, AA in the ESR1 gene were more prevalent in the case group compared to the control group. There was a significant association of ESR1 rs2234693 and rs9340799 genotypes with the disease in our population (p < 0.001). No significant association was found for these 3 polymorphisms at the allelic level. Analysis of different models of inheritance revealed that the codominant model (CT vs. CC+TT) and CT vs. CC for rs243865 polymorphism (Table III); and dominant model (TC+CC vs. TT), recessive model (CC vs. TT+TC), codominant model (TC vs. TT+CC) and TC vs. TT (WM vs. WW) for rs2234693 polymorphism (Table IV); and dominant model (AG+GG vs. AA), recessive model (GG vs. AA+AG), codominant model (AG vs. AA+GG) and AG vs. AA (WM vs. WW) for rs9340799 polymorphism (Table V) were significantly different between the case and control group.
The combinational analysis also revealed that rs243865 CC/rs2234693 CC/rs9340799 AA, rs243865 CC/rs2234693TC/rs9340799 AG, rs243865 CC/rs2234693 TT/rs9340799 AA, rs243865 CC/rs2234693 TT/rs9340799 GG, and rs243865 CT/rs2234693 TC/rs9340799 AG genotypes were significantly associated with the susceptibility to POI in our population (table VI). Among the 4 haplotypes for 2 polymorphisms in the ESR1 gene, rs2234693T/rs9340799A haplotype was found to be associated with conferring risk to POI (p = 0.04, OR = 1.42) (Table VII). Pairwise LD analysis also showed a moderate LD (D՛:30) for ESR1 -351 A/G (rs9340799) and ESR1 -397 T/C (rs2234693) polymorphisms in our population.
4. Discussion
Like other multifactorial diseases, POI originated from various genetics and environmental factors (1). Therefore, we performed a case-control study to investigate the possible association of 3 polymorphisms in the MMP2 and ESR1 gene and susceptibility to POI in Iranian women. Our study showed a significant association of ESR1 rs2234693 and rs9340799 genotypes with the disease in our population. In addition, the codominant model (CT vs. CC+TT) and CT vs. CC of MMP2 rs243865 polymorphism were found to be correlated with the risk of POI. No allelic association was found for these 3 polymorphisms. In the ESR1 gene, rs2234693T/rs9340799A haplotype was also associated with developing vulnerability to POI.
The ESR1 gene encoding estrogen α receptor is one of the fundamental molecules in the human reproductive system (17). Estrogen has a positive or negative impact on the regulation of gonadotropin secretion, folliculogenesis, and ovulation. Therefore, any variations in its gene may affect the time of menarche or menopause, resulting in developing POI (17, 18). In addition, the polymorphisms in this gene have been investigated in different diseases related to females, such as breast cancer, endometriosis, and uterine fibroid (19-21). Although some studies revealed the positive association of ESR1 -397 T/C (rs2234693) and -351 A/G (rs9340799) with POI (22, 23), others showed conflicting results (24, 25). Similar to our study, a study on Caucasian women revealed a positive association of these 2 polymorphisms with POI (23). In addition, a significant association of these 2 polymorphisms and their haplotype with POI was found in the Chinese population (22). However, a meta-analysis study showed no association of these polymorphisms with susceptibility to POI (26). In contrast to our study, a study on Korean women also found no association of ESR1 -397 T/C (rs2234693) with the disease (27). Following our study, another meta-analysis investigating these 2 polymorphisms (3 case-control studies with 1396 subjects) revealed a significant association of ESR1 -397 T/C (rs2234693) polymorphism with POI in the Asian population in all models; however, no significant association was found for any models in the European population. In terms of -351 A/G (rs9340799) polymorphism, this meta-analysis showed no association overall, but under dominant model was associated with POI in the Asian population (18). A functional study also indicated that CC genotypes of rs2234693 significantly reduces the ESR1 expression level (28). C allele decreases the binding of AP-4 as a transcriptional activator to the sense strand and the binding of ZNF238 as a transcriptional repressor to the antisense strand, resulting in unstable ESR1 mRNA (29, 30).
MMP2 is involved in the AMH regression pathway and indirectly reduces AMH in POI women. Genetic variants in this gene, including 1306C > T, may affect the expression of this gene, and any changes in its expression can lead to ovarian structural and follicular growth changes (7). A functional study showed that the T allele in the SP1 sequence, a consensus sequence in the MMP2 promoter (-1306 site; -1307C(C/T) ACC-1303) can disrupt the activity of the promoter and lower MMP2 gene expression (31). Therefore, evaluating the polymorphism can pave the way for finding the disease pathogenesis and genes involved in its development. There is only one study investigating the association of MMP2 -1306C > T rs243865 with POI. Contrary to our study in which only the CT vs. CC model is related to POI, Kim and colleagues indicated that MMP2 -1306CT + TT was associated with POI susceptibility (7).
To the best of our knowledge, this is the first study investigating the association of these 3 polymorphisms with POI in the Iranian population. Although, more functional studies with more samples and more polymorphisms in these genes can provide more strong results.
5. Conclusion
This study indicated that rs2234693 and rs9340799 polymorphisms of the ESR1 gene and MMP2 -1306C > T rs243865 in the codominant model are significant in relation to vulnerability to POI among Iranian women. Finding genotypes in susceptibility to POI would help detect POI and provide precious information for counseling of pregnancy loss in the young couple.
Acknowledgments
The authors thank all the patients and individuals who attended this study.
Conflict of Interest
The authors declare that they do not have any conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Genetics
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
