
International Journal of
Reproductive Biomedicine
Mon, Jul 27, 2026
[Archive]
Volume 21, Issue 8 (August 2023)
IJRM 2023, 21(8): 647-656 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asemi-Rad A, Heidari Z, Mahmoudzadeh-Sagheb H, Mehdipour Y, Moudi B, Sheibak N et al . Prevalence of congenital anomalies and related factors in live births in Zahedan, Southeast of Iran: A cross-sectional study. IJRM 2023; 21 (8) :647-656
URL: http://ijrm.ir/article-1-2730-en.html
URL: http://ijrm.ir/article-1-2730-en.html
Azam Asemi-Rad1 

 , Zahra Heidari2 , Hamidreza Mahmoudzadeh-Sagheb *3 , Yousef Mehdipour4 , Bita Moudi5 , Nadia Sheibak6 , Saeid Ebrahimi7
, Zahra Heidari2 , Hamidreza Mahmoudzadeh-Sagheb *3 , Yousef Mehdipour4 , Bita Moudi5 , Nadia Sheibak6 , Saeid Ebrahimi7
, Zahra Heidari2 , Hamidreza Mahmoudzadeh-Sagheb *3 , Yousef Mehdipour4 , Bita Moudi5 , Nadia Sheibak6 , Saeid Ebrahimi7
1- Department of Anatomical Sciences, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran. Cellular and Molecular Research Center, Zahedan University of Medical Sciences, Zahedan, Iran.
2- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran. Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran.
3- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran ,histology@ymail.com
4- Department of Health Information Technology, School of Paramedical Sciences, Torbat Heydarieh University of Medical Sciences, Torbat Heydarieh, Iran.
5- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran
6- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran.
7- Department of Health Information Technology, Zahedan University of Medical Sciences, Zahedan, Iran.
2- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran. Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran.
3- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran ,
4- Department of Health Information Technology, School of Paramedical Sciences, Torbat Heydarieh University of Medical Sciences, Torbat Heydarieh, Iran.
5- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran Infectious Diseases and Tropical Medicine Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences, Zahedan, Iran
6- Department of Histology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran.
7- Department of Health Information Technology, Zahedan University of Medical Sciences, Zahedan, Iran.
Full-Text [PDF 759 kb]
(1297 Downloads)
| Abstract (HTML) (1702 Views)
1. Introduction
Congenital anomalies (CAs) represent a group of abnormalities that occur during pregnancy and are associated with prenatal death, childhood mortality, and adolescent disability (1, 2). Since 1960, general supervision for the emergence of infants with CAs has been carried out in various populations worldwide. It has been shown that the prevalence of preterm labor and CA noticeably varies in different countries (3, 4). In the United States, the prevalence rate of CA in newborns is 3% (3). According to the European Congenital Abnormalities Organization, the average rate of birth defects was 24.26 per 1000 births from 2010-2014 (5). The prevalence of CA in Iran has been reported in some studies. In northern Iran, the prevalence rate of congenital heart abnormalities was 6-8 per 1000 live births (6). In another study in the Northeast, Iran, the CA rate was about 29.11 per 1000 live birth (7).
Typically, the most common causes of neonatal mortality are disorders associated with developmental defects (1, 2). As defined by the World Health Organization (WHO), these defects include single or multiple structural defects, such as cleft lip, and cleft palate, or functional defects that contain biochemical and molecular defects that can be identified at birth (8). CA is divided into 2 categories based on severity, major and minor defects. Major defects are defined as anatomical defects that affect a person's life and appearance. Minor defects are structural changes that do not require treatment or are recovered with simple methods (9). Based on the categories provided by the WHO, CA includes defects in the nervous system, eyes, ears, face and neck, cardiovascular system, respiratory system, cleft lip and palate, gastrointestinal system, urinary and genital system, musculoskeletal system, clinical syndromes, and chromosomal abnormalities. Each category contains a sub-division (10).
The prevention of CA requires background knowledge. The prevalence rate of these deficiencies can contribute somewhat to their prevention (8). The majority of CAs have unknown reasons (11) and are caused by different factors, like physical and chemical environmental factors as well as various maternal factors, such as age, type of pregnancy, delivery type, and maternal health (12).
According to the fact that the estimation of the prevalence rate of CA is crucial to developing prevention strategies, and to the best of our knowledge, there have been few or no studies directly related to the prevalence of CA and predisposing risk factors in Southeast Iran. This study aimed to evaluate the prevalence of CAs and related risk factors in live births from 2009-2019 in Zahedan, Southeast Iran.
2. Materials and Methods
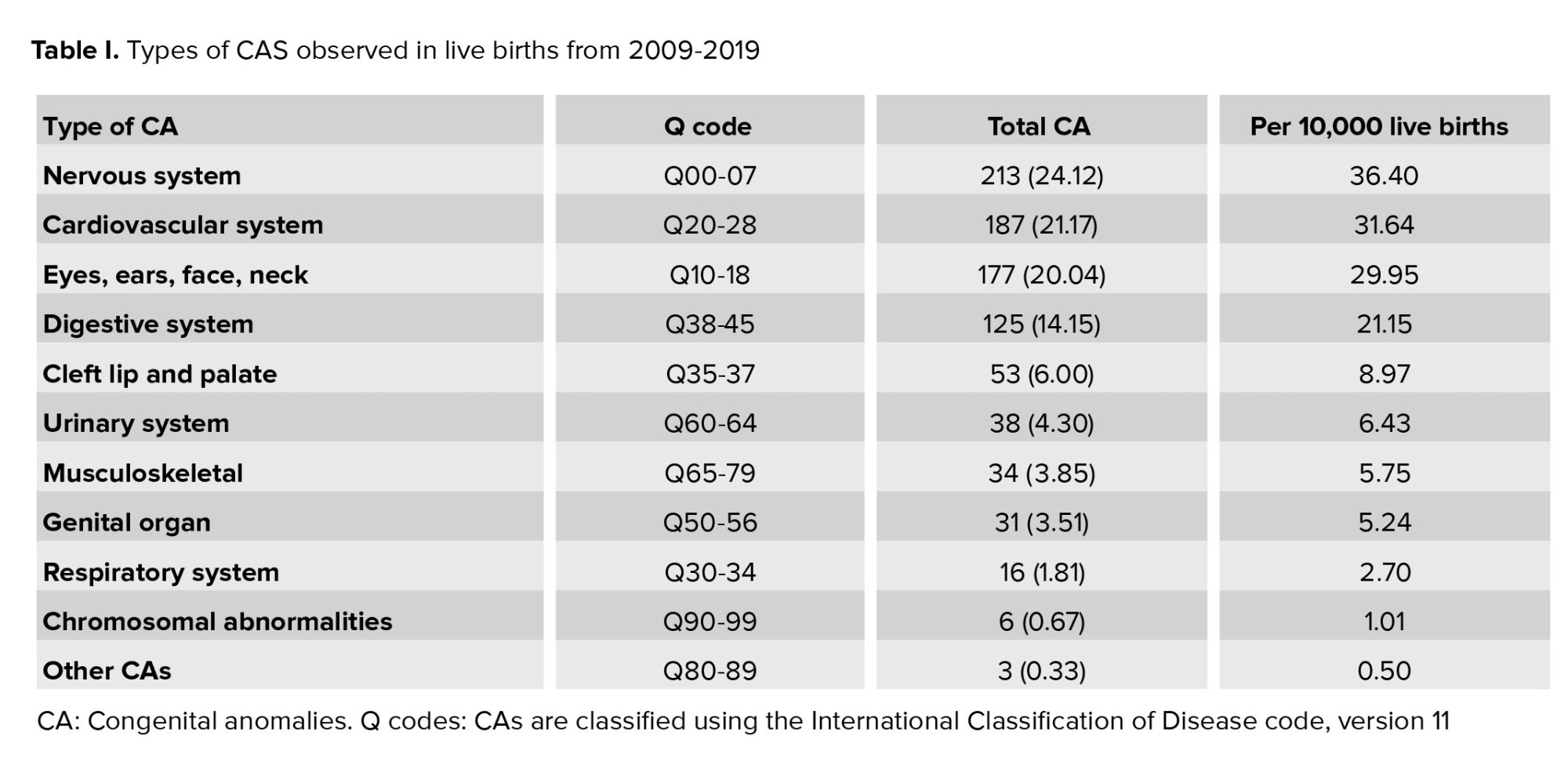
This cross-sectional hospital-based study was conducted retrospectively, assessing the medical records of all newborns delivered in the Ali-Ibn-Abitaleb referral hospital of Zahedan, Iran over a 10 yr period, from April 2009-2019. Inclusion and exclusion criteria were as follows, cases with stillbirth were eliminated from the study; pediatricians examined all live births, and anomalies were registered. Newborns with at least one diagnosed CA were enrolled in the study. For this study, CA was defined as major structural defects that existed at birth or in infancy, either clinically or through screening methods. These anomalies were classified using the International Classification of Disease Code, version 11 (Table I) (10).
The information obtained consisted of sex, birth age, birth weight, mother's age, delivery type, pregnancy type, mother's underlying disease, mother’s medicine consumption, parents smoking and drug usage, consanguinity marriage between parents, the existence of CA in family and relatives, and history of hospitalization.
2.1. Ethical considerations
The Ethics Committee of Zahedan University of Medical Science, Zahedan, Iran approved this study (Code: IR.ZAUMS.REC.1398.076). A written consent form was signed by each participants.
2.2. Statistical analysis
A student t test was used to determine whether 2 independent groups had significantly different means. Quantitative variables were compared using the ANOVA test, while qualitative variables were compared using the Chi-square test. Finally, the results are reported as mean ± SEM. The statistical tests were conducted using SPSS software version 20. Statistical significance was defined as p ≤ 0.05.
3. Results
In the current study, 705 newborns with a single anomaly and 178 newborns with multiple anomalies were enrolled; 523 cases were male and 358 were female, while the gender of the 2 cases were unknown due to ambiguous genitalia.
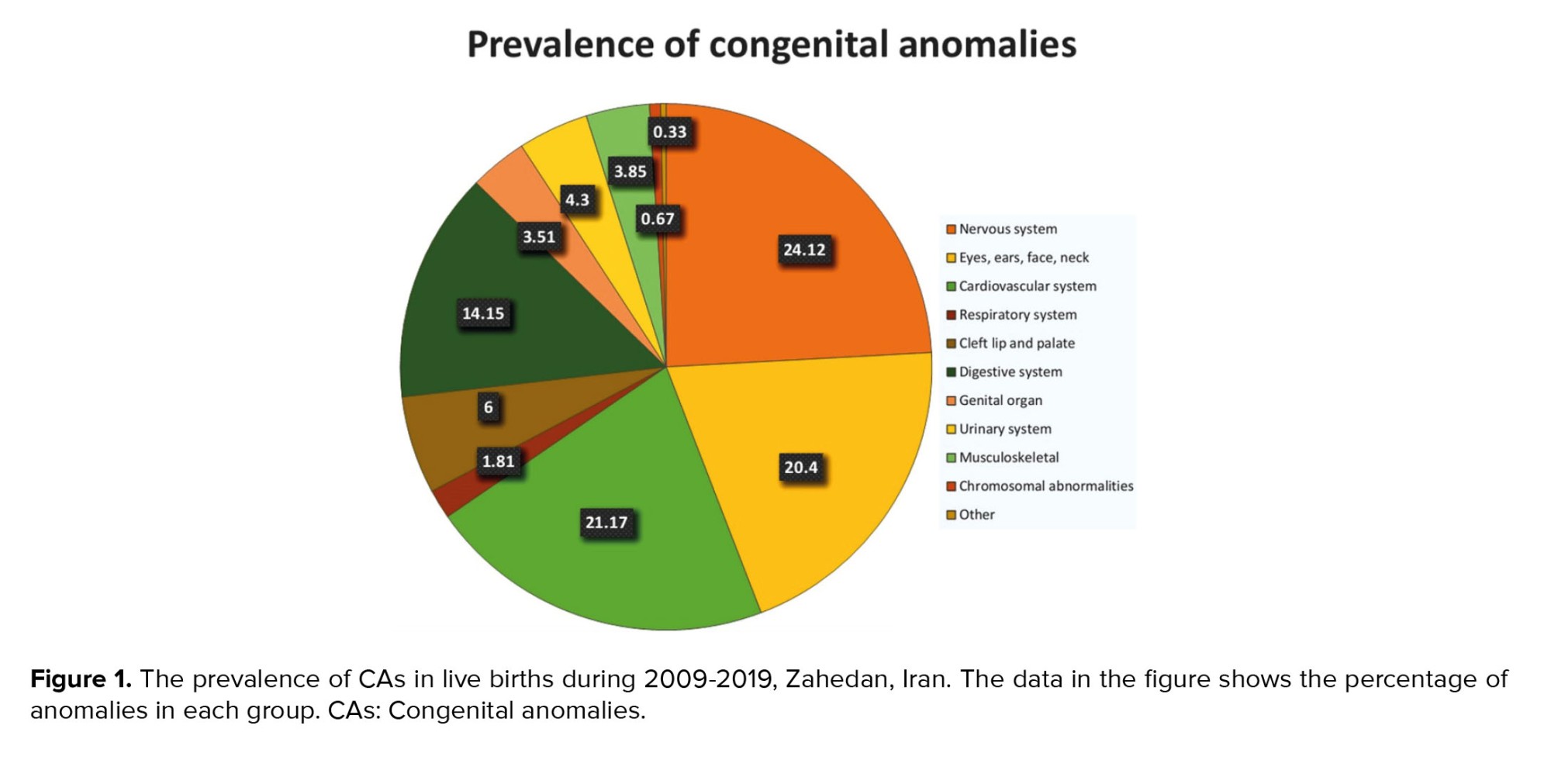
The results of this study indicated that the obvious CAs were 883 in 59,085 neonate live births in April 2009-2019, giving an overall prevalence rate of 1.49% (Table I). As reported in table II, CA in the nervous system was a frequent anomaly and after the other CAs and chromosomal abnormalities, malformations of the respiratory system had the lowest prevalence. CAs in the cardiovascular system and the eyes, ears, face, and neck was the second and third highest after the nervous system, respectively. Moreover, the CAs of the digestive system is more frequent than the malformation of the cleft lip and palate (Table I, Figure 1).
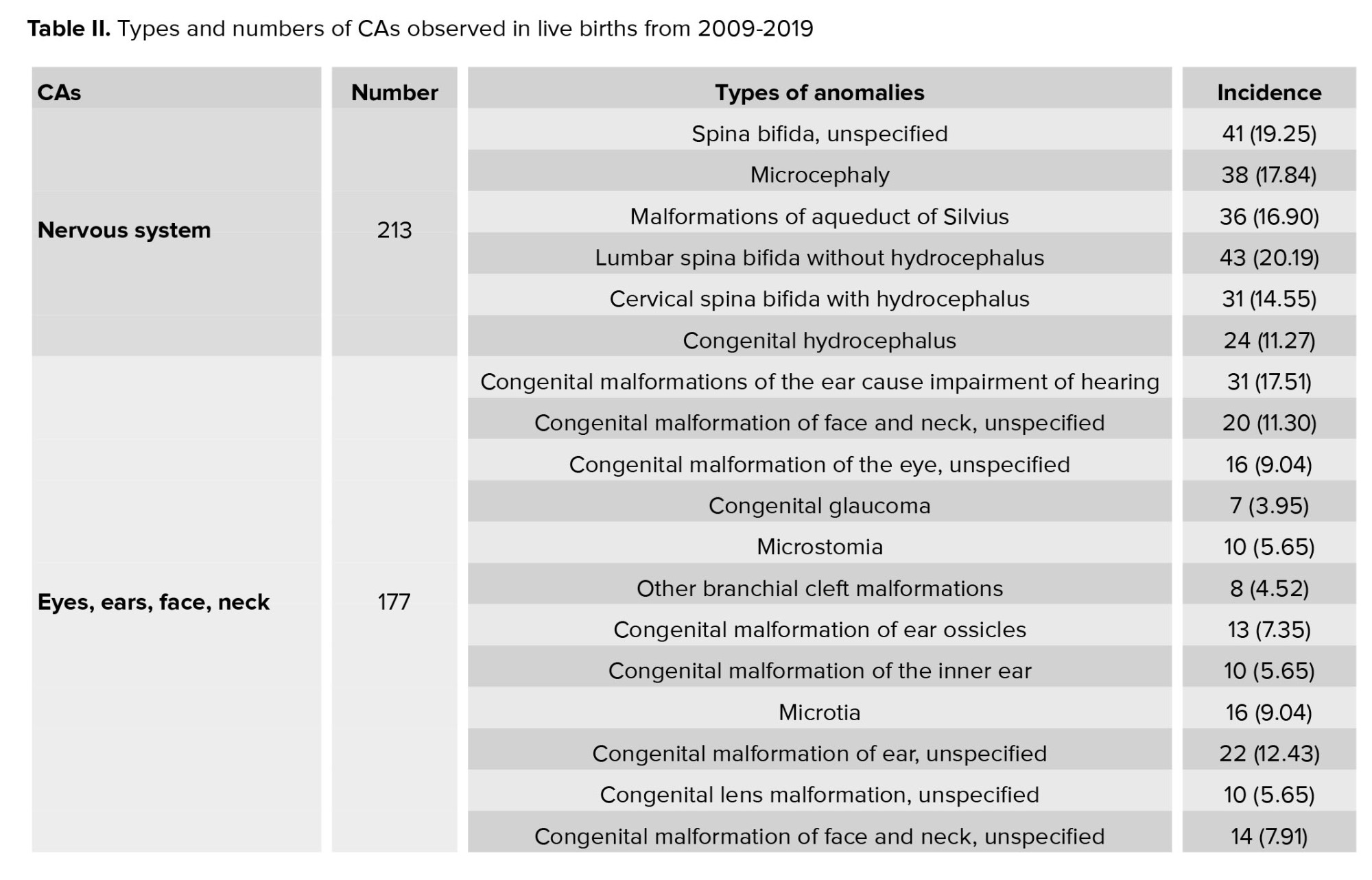
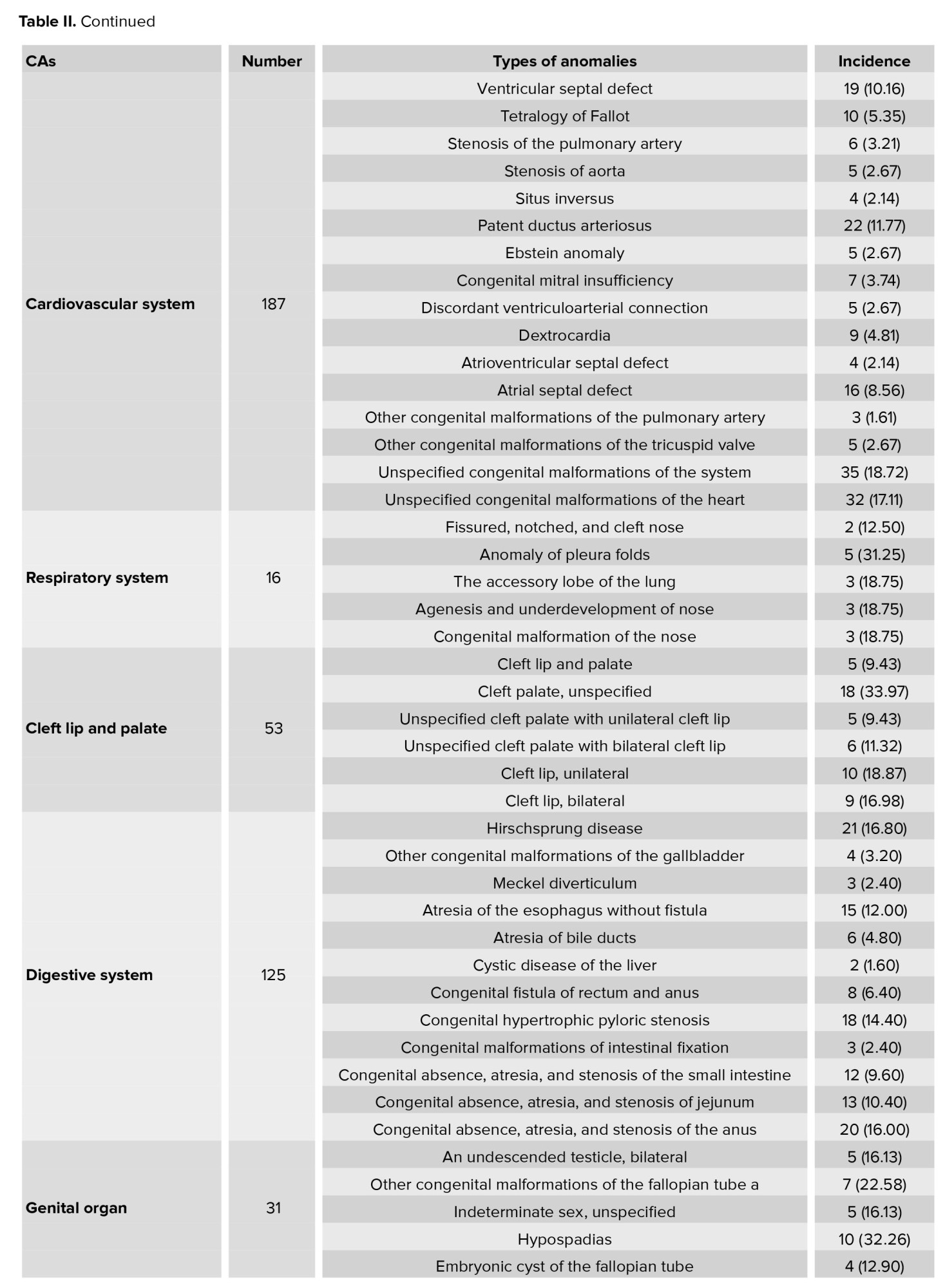
A large percentage of CAs in the nervous system are affected by unspecified spina bifida. The most common anomalies in the cardiovascular system were unspecified malformations of the heart, unspecified malformations of the cardiovascular system, and patent ductus arteriosus. Moreover, unilateral cleft lip showed a higher prevalence compared to bilateral disorder.
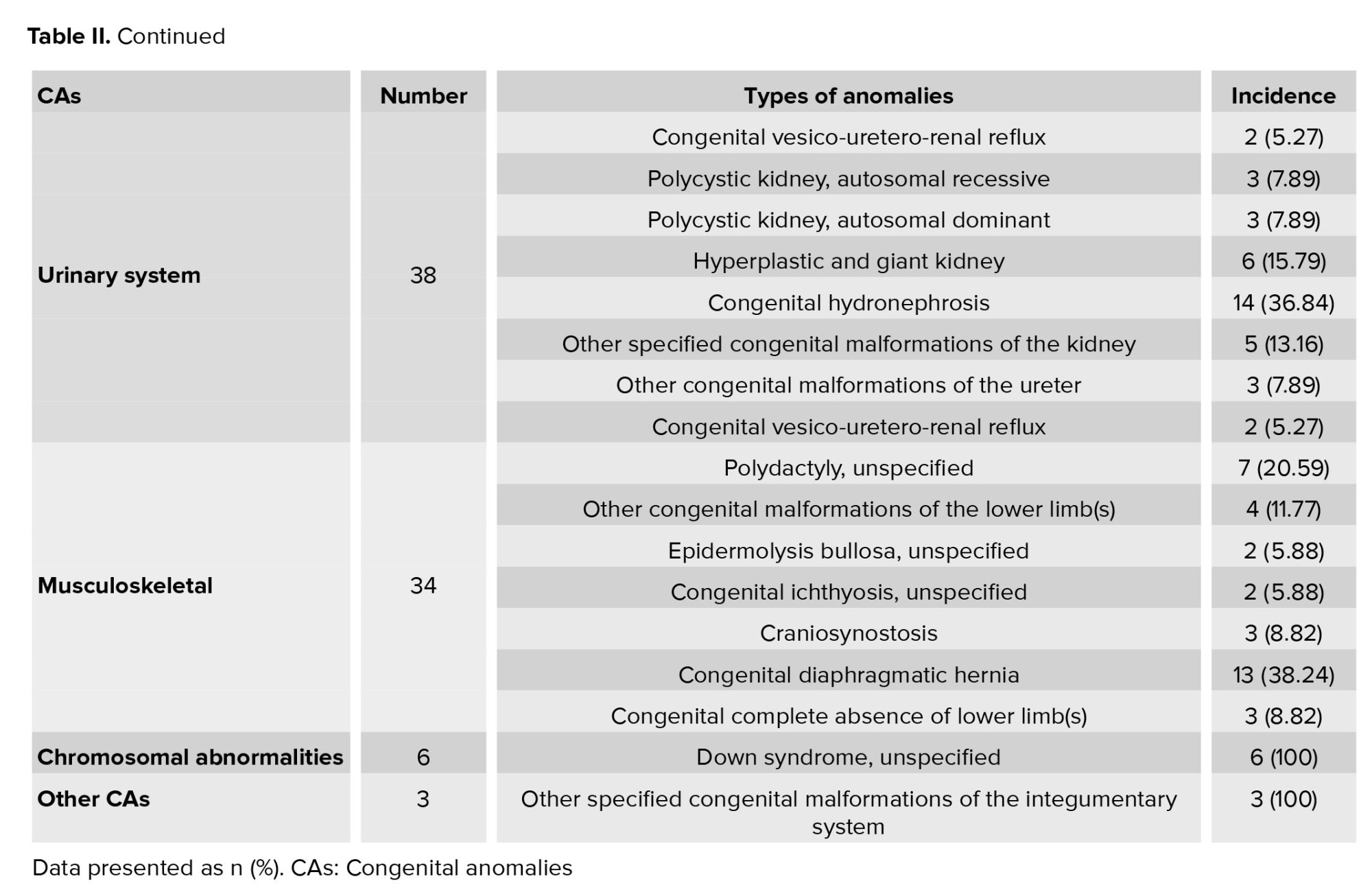
Out of all anomalies in the eyes, ears, face, and neck, malformations of the ear causing hearing impairment was the most common. Further, the most prevalent anomaly in the genital system was hypospadias. In this study, congenital hydronephrosis represented the highest percentage of urinary system anomalies and the congenital diaphragmatic hernia also had the highest number of musculoskeletal anomalies. We found that the anomaly of pleura folds was the most common among the abnormalities affecting the respiratory system. Eventually, Down syndrome became the most prevalent anomaly in the category of other CAs (Table II).
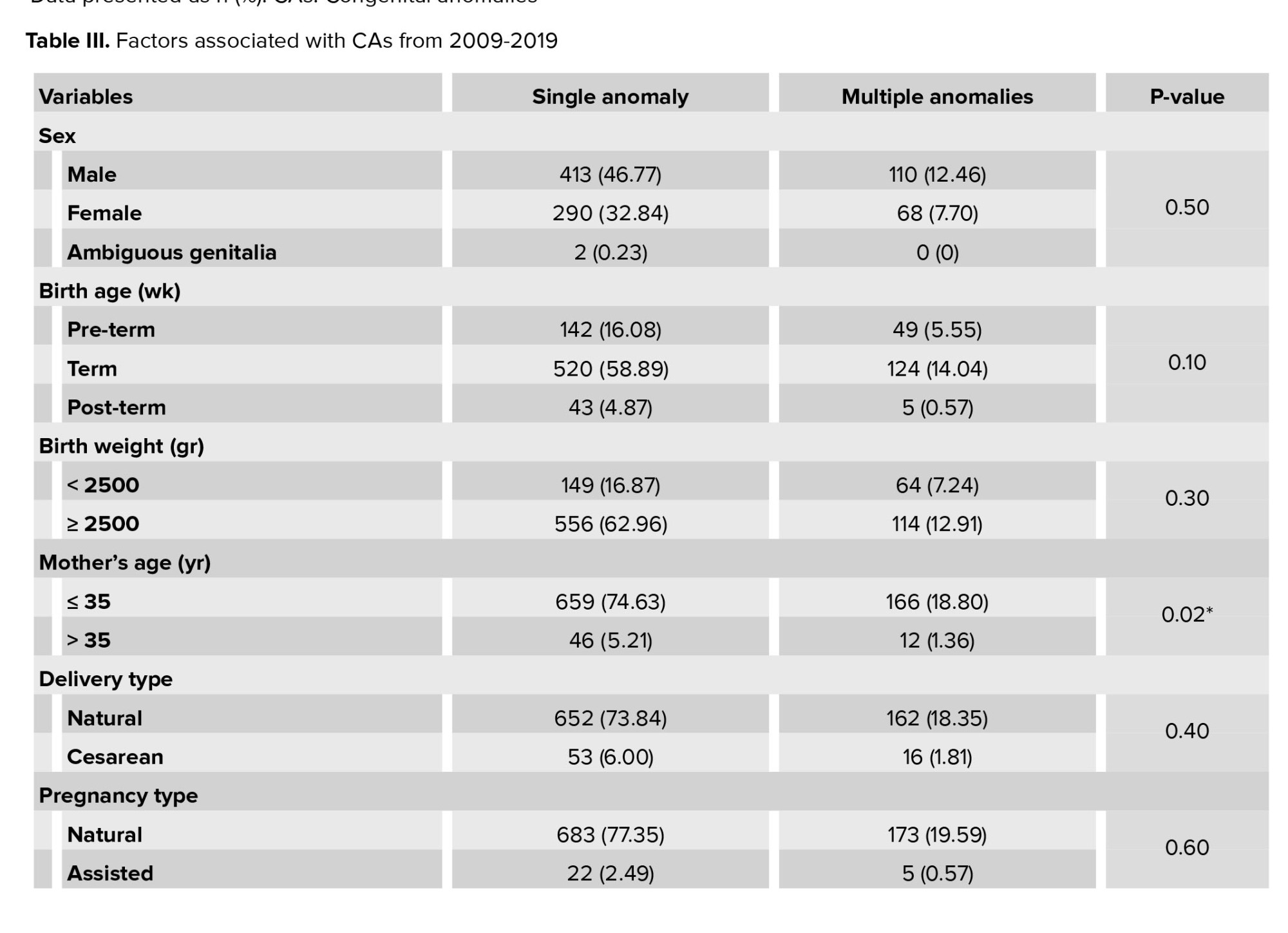
More detailed demographic data of newborns enrolled in the present study, including newborns' sex, birth age, and weight, delivery, and pregnancy types, and information about their parents, such as maternal age, consanguineous marriage, maternal health, and family history, are presented in table III.
Statistical analysis showed no correlation between CAs and sex, birth age, pregnancy type, or delivery type (p = 0.40, Table III). No significant relationship was observed between the type of CA and medicine consumption (p = 0.09). Besides underlying diseases, smoking, and drug usage do not correlate with the type of CA (respectively, p = 0.20, p = 0.50). In contrast, a significant correlation was observed between CA and the parent’s consanguinity marriage (p = 0.02). The probability of having a baby with multiple CAs was significantly higher in mothers over 35 (p = 0.02).
A significant relationship existed between an existing anomaly in the family and relatives with CA (p < 0.001, p = 0.01). Furthermore, hospitalization significantly correlates with multiple anomalies (p < 0.001; Table III).
4. Discussion
The current study showed that the total prevalence of CA in live birth was 149 per 10,000 births (1.49%) in Zahedan. Anomalies of the nervous and cardiovascular systems were the most frequent anomalies in live births and spina bifida was the most common anomaly of the central nervous system. The most common anomalies of the cardiovascular system were unspecified heart malformations, cardiovascular malformations, and patent ductus arteriosus. We found significant correlations between the parent's consanguinity marriages, the mother's age, an existing anomaly in the family, and relatives with the presence of single and multiple CAs.
By reviewing the hospital centers, the WHO has reported a rate of 2.20% for congenital malformations (13). This incidence rate is about 2-5% in Europe and the United States (14). According to a report on the prevalence of live birth with CAs in Europe, the prevalence was more than 10.4 per 1000 live births (15). A study of the prevalence of CAs in newborns in São Paulo indicated a prevalence of 1.6 per 100 live births (16). A lower rate in the current study may be due to lower health care service usage for delivery, considering some indigenous beliefs.
Also, midwives may not have registered anomalies at the delivery facility centers. The current study was a partial estimation about the physical examination of newborns, and additional disabilities diagnosed with age or abnormalities that cause death during the fetal period were not counted. Besides, some abnormalities present at birth are not obvious until a while later. In this study, the frequency of cases with CAs in male neonates was higher than in female neonates. 2 other studies also reported a higher prevalence of CA in male newborns (9, 17).
According to the previous results, nervous system anomalies are the most frequent defects. The study's findings showed that the incidence of CA in the central nervous system was about 3.64 per 1000 births. The prevalence of nervous system defects reported about 0.4 per 1000 births (15). In a study in Iran, it was demonstrated that the prevalence of neural tube defects was about 1.01-8.29 per 1000 live births (4).
The most prevalent system affected by CA after the nervous system is the cardiovascular system, the eyes, ears, face, neck, and digestive system, respectively, with a prevalence rate between 21 and 31 per 10,000 live births.
In a study that analyzed the prevalence of congenital heart disease (CHD)-related articles worldwide, the result demonstrated that the prevalence of CHD was 9.4 in 1000 live births and globally increased and changed around the world with a considerable increase in Asia (18). The age of CHD diagnosis and the method used for screening are the main reasons for the difference in CHD prevalence (19). It is indicated that the possibility of a CHD diagnosis increases as the gestational age increases (20).
Around the world, the cleft palate with or without a cleft lip occurs in about one in every 700 live births (13). The global prevalence of cleft palate in every 1000 live births was estimated about 0.33 and the prevalence of cleft lip and palate was 0.45 per 10,000 live births (21), and our results demonstrated 8.97 per 10,000 live birth.
The current study showed that the prevalence of CA in the urinary system, musculoskeletal system, and genital system affects about 6.43 to 5.24 per 10,000 live births. The prevalence of congenital disorders of the urinary system among newborns in the US was estimated at 2% (22). In another study in Egypt, the CA of the genital system was about 5.4% (23). Abnormalities in the kidney and urinary systems are associated with lower gestational age and genetic disorders, so they are diagnosed earlier in pregnancy (22).
The current study found that the respiratory system, chromosomal abnormalities, and other CAs had a lower prevalence rate. Notably, this information is acquired from the hospital's information technology system and includes only a fraction of the newborn population.
The difference between the results of the abovementioned studies may be due to low socioeconomic status and education. Although increasing public information accompanied by access to healthcare may lead to increased detection of minor abnormalities, termination of pregnancy with severe anomalies can also decrease incidence (18).
No significant relationship was observed between CA and sex, birth weight, type of delivery, smoking, or drug usage. Consanguinity marriage between parents, a person with CA in the family, and relatives had a significant relationship with multiple anomalies, and hospitalization was more likely in cases with multiple anomalies. Consanguinity marriage is known as a risk factor for CA. It is shown that the risk of giving birth to a baby with CA in parents with a consanguinity marriage is higher than in others (24, 25). The prevalence of consanguineous marriage in different parts of Iran is around 37.40% (26), and the difference in the probability of risk obtained in different studies may be due to differences in the prevalence of consanguineous marriage in different regions.
Moreover, consanguinity marriage is common in Iran, especially among the ethnicities, including Sistani and Baluch, which have a relatively high frequency. Previous studies have indicated that the consanguinity of parents could increase the risk of CAs (27). In this study, the frequency of CAs was higher in infants born to women aged over 37 yr, and this difference was statistically significant. The risk of fetal chromosomal abnormalities increased with maternal age (28).
The current study demonstrates the prevalence rate of CAs in live birth in Zahedan, Iran, where there is no report about the CA. The study strength was an adequate time period of around 10 yr, which allowed the study of abnormalities in 59,085 live births. However, we may have significantly underestimated the actual incidence of these anomalies in the general population. Moreover, we did not include abortions and stillbirths in this study. However, the prevalence of CA is higher among aborted fetuses and stillbirths (29). Also, the anomaly data may not be registered at the delivery facility centers by midwives.
5. Conclusion
Congenital disabilities are the leading cause of death in children under the age of 5. Therefore, to prevent and evaluate birth defects accurately, obtaining data about the prevalence of birth defects is necessary. Using the obtained data, effective interventions can be performed on some defects, such as NTDs, which can be prevented by taking folic acid during pregnancy (29).
The current study estimated the prevalence of CAs at 14.6 per 1000 live births. Because some families do not utilize medical services for delivery, as well as the initial assessments of the newborn, it is necessary to have a preconception visit. Also, increasing general knowledge about the leading causes of fetal defects and prenatal screening can progressively reduce the apparent prevalence of CAs. Furthermore, after alerting physicians concerning the importance of visiting newborns and diagnosing CAs, training the nurses and midwives is essential for accurately recording cases and having the exact statistics, because this region is a high-traffic border between the countries. Also, by creating a monitoring system, the precise pattern, the possible etiology, and the prevalence of abnormalities in the general population could be determined. It must be considered in childbearing and population-youth policies.
Acknowledgments
The authors would like to thank the Vice Chancellor of Research and Technology of Zahedan University of Medical Sciences, Zahedan, Iran (grant no: 9366) and all those who willingly helped in this study.
Conflicts of Interest
The authors declare that there is no conflict of interest.
Full-Text: (280 Views)
1. Introduction
Congenital anomalies (CAs) represent a group of abnormalities that occur during pregnancy and are associated with prenatal death, childhood mortality, and adolescent disability (1, 2). Since 1960, general supervision for the emergence of infants with CAs has been carried out in various populations worldwide. It has been shown that the prevalence of preterm labor and CA noticeably varies in different countries (3, 4). In the United States, the prevalence rate of CA in newborns is 3% (3). According to the European Congenital Abnormalities Organization, the average rate of birth defects was 24.26 per 1000 births from 2010-2014 (5). The prevalence of CA in Iran has been reported in some studies. In northern Iran, the prevalence rate of congenital heart abnormalities was 6-8 per 1000 live births (6). In another study in the Northeast, Iran, the CA rate was about 29.11 per 1000 live birth (7).
Typically, the most common causes of neonatal mortality are disorders associated with developmental defects (1, 2). As defined by the World Health Organization (WHO), these defects include single or multiple structural defects, such as cleft lip, and cleft palate, or functional defects that contain biochemical and molecular defects that can be identified at birth (8). CA is divided into 2 categories based on severity, major and minor defects. Major defects are defined as anatomical defects that affect a person's life and appearance. Minor defects are structural changes that do not require treatment or are recovered with simple methods (9). Based on the categories provided by the WHO, CA includes defects in the nervous system, eyes, ears, face and neck, cardiovascular system, respiratory system, cleft lip and palate, gastrointestinal system, urinary and genital system, musculoskeletal system, clinical syndromes, and chromosomal abnormalities. Each category contains a sub-division (10).
The prevention of CA requires background knowledge. The prevalence rate of these deficiencies can contribute somewhat to their prevention (8). The majority of CAs have unknown reasons (11) and are caused by different factors, like physical and chemical environmental factors as well as various maternal factors, such as age, type of pregnancy, delivery type, and maternal health (12).
According to the fact that the estimation of the prevalence rate of CA is crucial to developing prevention strategies, and to the best of our knowledge, there have been few or no studies directly related to the prevalence of CA and predisposing risk factors in Southeast Iran. This study aimed to evaluate the prevalence of CAs and related risk factors in live births from 2009-2019 in Zahedan, Southeast Iran.
2. Materials and Methods
This cross-sectional hospital-based study was conducted retrospectively, assessing the medical records of all newborns delivered in the Ali-Ibn-Abitaleb referral hospital of Zahedan, Iran over a 10 yr period, from April 2009-2019. Inclusion and exclusion criteria were as follows, cases with stillbirth were eliminated from the study; pediatricians examined all live births, and anomalies were registered. Newborns with at least one diagnosed CA were enrolled in the study. For this study, CA was defined as major structural defects that existed at birth or in infancy, either clinically or through screening methods. These anomalies were classified using the International Classification of Disease Code, version 11 (Table I) (10).
The information obtained consisted of sex, birth age, birth weight, mother's age, delivery type, pregnancy type, mother's underlying disease, mother’s medicine consumption, parents smoking and drug usage, consanguinity marriage between parents, the existence of CA in family and relatives, and history of hospitalization.
2.1. Ethical considerations
The Ethics Committee of Zahedan University of Medical Science, Zahedan, Iran approved this study (Code: IR.ZAUMS.REC.1398.076). A written consent form was signed by each participants.
2.2. Statistical analysis
A student t test was used to determine whether 2 independent groups had significantly different means. Quantitative variables were compared using the ANOVA test, while qualitative variables were compared using the Chi-square test. Finally, the results are reported as mean ± SEM. The statistical tests were conducted using SPSS software version 20. Statistical significance was defined as p ≤ 0.05.
3. Results
In the current study, 705 newborns with a single anomaly and 178 newborns with multiple anomalies were enrolled; 523 cases were male and 358 were female, while the gender of the 2 cases were unknown due to ambiguous genitalia.
The results of this study indicated that the obvious CAs were 883 in 59,085 neonate live births in April 2009-2019, giving an overall prevalence rate of 1.49% (Table I). As reported in table II, CA in the nervous system was a frequent anomaly and after the other CAs and chromosomal abnormalities, malformations of the respiratory system had the lowest prevalence. CAs in the cardiovascular system and the eyes, ears, face, and neck was the second and third highest after the nervous system, respectively. Moreover, the CAs of the digestive system is more frequent than the malformation of the cleft lip and palate (Table I, Figure 1).
A large percentage of CAs in the nervous system are affected by unspecified spina bifida. The most common anomalies in the cardiovascular system were unspecified malformations of the heart, unspecified malformations of the cardiovascular system, and patent ductus arteriosus. Moreover, unilateral cleft lip showed a higher prevalence compared to bilateral disorder.
Out of all anomalies in the eyes, ears, face, and neck, malformations of the ear causing hearing impairment was the most common. Further, the most prevalent anomaly in the genital system was hypospadias. In this study, congenital hydronephrosis represented the highest percentage of urinary system anomalies and the congenital diaphragmatic hernia also had the highest number of musculoskeletal anomalies. We found that the anomaly of pleura folds was the most common among the abnormalities affecting the respiratory system. Eventually, Down syndrome became the most prevalent anomaly in the category of other CAs (Table II).
More detailed demographic data of newborns enrolled in the present study, including newborns' sex, birth age, and weight, delivery, and pregnancy types, and information about their parents, such as maternal age, consanguineous marriage, maternal health, and family history, are presented in table III.
Statistical analysis showed no correlation between CAs and sex, birth age, pregnancy type, or delivery type (p = 0.40, Table III). No significant relationship was observed between the type of CA and medicine consumption (p = 0.09). Besides underlying diseases, smoking, and drug usage do not correlate with the type of CA (respectively, p = 0.20, p = 0.50). In contrast, a significant correlation was observed between CA and the parent’s consanguinity marriage (p = 0.02). The probability of having a baby with multiple CAs was significantly higher in mothers over 35 (p = 0.02).
A significant relationship existed between an existing anomaly in the family and relatives with CA (p < 0.001, p = 0.01). Furthermore, hospitalization significantly correlates with multiple anomalies (p < 0.001; Table III).
4. Discussion
The current study showed that the total prevalence of CA in live birth was 149 per 10,000 births (1.49%) in Zahedan. Anomalies of the nervous and cardiovascular systems were the most frequent anomalies in live births and spina bifida was the most common anomaly of the central nervous system. The most common anomalies of the cardiovascular system were unspecified heart malformations, cardiovascular malformations, and patent ductus arteriosus. We found significant correlations between the parent's consanguinity marriages, the mother's age, an existing anomaly in the family, and relatives with the presence of single and multiple CAs.
By reviewing the hospital centers, the WHO has reported a rate of 2.20% for congenital malformations (13). This incidence rate is about 2-5% in Europe and the United States (14). According to a report on the prevalence of live birth with CAs in Europe, the prevalence was more than 10.4 per 1000 live births (15). A study of the prevalence of CAs in newborns in São Paulo indicated a prevalence of 1.6 per 100 live births (16). A lower rate in the current study may be due to lower health care service usage for delivery, considering some indigenous beliefs.
Also, midwives may not have registered anomalies at the delivery facility centers. The current study was a partial estimation about the physical examination of newborns, and additional disabilities diagnosed with age or abnormalities that cause death during the fetal period were not counted. Besides, some abnormalities present at birth are not obvious until a while later. In this study, the frequency of cases with CAs in male neonates was higher than in female neonates. 2 other studies also reported a higher prevalence of CA in male newborns (9, 17).
According to the previous results, nervous system anomalies are the most frequent defects. The study's findings showed that the incidence of CA in the central nervous system was about 3.64 per 1000 births. The prevalence of nervous system defects reported about 0.4 per 1000 births (15). In a study in Iran, it was demonstrated that the prevalence of neural tube defects was about 1.01-8.29 per 1000 live births (4).
The most prevalent system affected by CA after the nervous system is the cardiovascular system, the eyes, ears, face, neck, and digestive system, respectively, with a prevalence rate between 21 and 31 per 10,000 live births.
In a study that analyzed the prevalence of congenital heart disease (CHD)-related articles worldwide, the result demonstrated that the prevalence of CHD was 9.4 in 1000 live births and globally increased and changed around the world with a considerable increase in Asia (18). The age of CHD diagnosis and the method used for screening are the main reasons for the difference in CHD prevalence (19). It is indicated that the possibility of a CHD diagnosis increases as the gestational age increases (20).
Around the world, the cleft palate with or without a cleft lip occurs in about one in every 700 live births (13). The global prevalence of cleft palate in every 1000 live births was estimated about 0.33 and the prevalence of cleft lip and palate was 0.45 per 10,000 live births (21), and our results demonstrated 8.97 per 10,000 live birth.
The current study showed that the prevalence of CA in the urinary system, musculoskeletal system, and genital system affects about 6.43 to 5.24 per 10,000 live births. The prevalence of congenital disorders of the urinary system among newborns in the US was estimated at 2% (22). In another study in Egypt, the CA of the genital system was about 5.4% (23). Abnormalities in the kidney and urinary systems are associated with lower gestational age and genetic disorders, so they are diagnosed earlier in pregnancy (22).
The current study found that the respiratory system, chromosomal abnormalities, and other CAs had a lower prevalence rate. Notably, this information is acquired from the hospital's information technology system and includes only a fraction of the newborn population.
The difference between the results of the abovementioned studies may be due to low socioeconomic status and education. Although increasing public information accompanied by access to healthcare may lead to increased detection of minor abnormalities, termination of pregnancy with severe anomalies can also decrease incidence (18).
No significant relationship was observed between CA and sex, birth weight, type of delivery, smoking, or drug usage. Consanguinity marriage between parents, a person with CA in the family, and relatives had a significant relationship with multiple anomalies, and hospitalization was more likely in cases with multiple anomalies. Consanguinity marriage is known as a risk factor for CA. It is shown that the risk of giving birth to a baby with CA in parents with a consanguinity marriage is higher than in others (24, 25). The prevalence of consanguineous marriage in different parts of Iran is around 37.40% (26), and the difference in the probability of risk obtained in different studies may be due to differences in the prevalence of consanguineous marriage in different regions.
Moreover, consanguinity marriage is common in Iran, especially among the ethnicities, including Sistani and Baluch, which have a relatively high frequency. Previous studies have indicated that the consanguinity of parents could increase the risk of CAs (27). In this study, the frequency of CAs was higher in infants born to women aged over 37 yr, and this difference was statistically significant. The risk of fetal chromosomal abnormalities increased with maternal age (28).
The current study demonstrates the prevalence rate of CAs in live birth in Zahedan, Iran, where there is no report about the CA. The study strength was an adequate time period of around 10 yr, which allowed the study of abnormalities in 59,085 live births. However, we may have significantly underestimated the actual incidence of these anomalies in the general population. Moreover, we did not include abortions and stillbirths in this study. However, the prevalence of CA is higher among aborted fetuses and stillbirths (29). Also, the anomaly data may not be registered at the delivery facility centers by midwives.
5. Conclusion
Congenital disabilities are the leading cause of death in children under the age of 5. Therefore, to prevent and evaluate birth defects accurately, obtaining data about the prevalence of birth defects is necessary. Using the obtained data, effective interventions can be performed on some defects, such as NTDs, which can be prevented by taking folic acid during pregnancy (29).
The current study estimated the prevalence of CAs at 14.6 per 1000 live births. Because some families do not utilize medical services for delivery, as well as the initial assessments of the newborn, it is necessary to have a preconception visit. Also, increasing general knowledge about the leading causes of fetal defects and prenatal screening can progressively reduce the apparent prevalence of CAs. Furthermore, after alerting physicians concerning the importance of visiting newborns and diagnosing CAs, training the nurses and midwives is essential for accurately recording cases and having the exact statistics, because this region is a high-traffic border between the countries. Also, by creating a monitoring system, the precise pattern, the possible etiology, and the prevalence of abnormalities in the general population could be determined. It must be considered in childbearing and population-youth policies.
Acknowledgments
The authors would like to thank the Vice Chancellor of Research and Technology of Zahedan University of Medical Sciences, Zahedan, Iran (grant no: 9366) and all those who willingly helped in this study.
Conflicts of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Perinatology
References
1. Dolk H, Loane M, Teljeur C, Densem J, Greenlees R, McCullough N, et al. Detection and investigation of temporal clusters of congenital anomaly in Europe: Seven years of experience of the EUROCAT surveillance system. Eur J Epidemiol 2015; 30: 1153-1164. [DOI:10.1007/s10654-015-0012-y] [PMID] [PMCID]
2. Almli LM, Ely DM, Ailes EC, Abouk R, Grosse SD, Isenburg JL, et al. Infant mortality attributable to birth defects-United States, 2003-2017. Morb Mortal Wkly Rep 2020; 69: 25-29. [DOI:10.15585/mmwr.mm6902a1] [PMID] [PMCID]
3. Willis MD, Carozza SE, Hystad P. Congenital anomalies associated with oil and gas development and resource extraction: A population-based retrospective cohort study in Texas. J Expo Sci Environ Epidemiol 2023; 33: 84-93. [DOI:10.1038/s41370-022-00505-x] [PMID] [PMCID]
4. Mohammadi N, Mobasheri E, Golalipour MJ. Birth prevalence of neural tube defects in Iran: A systematic review. J Pediatr Rev 2018; 6: 15-20. [DOI:10.5812/jpr.62091]
5. Baumgartner H, Budts W, Chessa M, Deanfield J, Eicken A, Holm J, et al. Recommendations for organization of care for adults with congenital heart disease and for training in the subspecialty of 'Grown-up Congenital Heart Disease'in Europe: A position paper of the Working Group on Grown-up Congenital Heart Disease of the European Society of Cardiology. Eur Heart J 2014; 35: 686-690. [DOI:10.1093/eurheartj/eht572] [PMID]
6. Ebrahimi M, Esmaeili H. Frequency and diversity of congenital heart disease in children in northern Iran. J Clin Basic Res 2022; 6: 17-22.
7. Mashhadi Abdolahi H, Kargar Maher MH, Afsharnia F, Dastgiri S. Prevalence of congenital anomalies: A community-based study in the Northwest of Iran. ISRN Pediatr 2014; 2014: 920940. [DOI:10.1155/2014/920940] [PMID] [PMCID]
8. Lamichhane DK, Leem J-H, Park M, Kim JA, Kim HC, Kim JH, et al. Increased prevalence of some birth defects in Korea, 2009-2010. BMC Pregnancy Childbirth 2016; 16: 61-71. [DOI:10.1186/s12884-016-0841-z] [PMID] [PMCID]
9. Stevenson RE, Hall JG. Human malformations and related anomalies. 2th Ed. England: Oxford University Press; 2015. [DOI:10.1093/med/9780199386031.001.0001]
10. International Classification of Diseases (ICD). World Health Organization. 2021. Available at: https://www.who.int/standards/classifications/classification-of-diseases.
11. Ekwochi U, Asinobi IN, Osuorah DCI, Ndu IK, Ifediora C, Amadi OF, et al. Pattern of congenital anomalies in newborn: A 4-year surveillance of newborns delivered in a tertiary healthcare facility in the south-east Nigeria. J Trop Pediatr 2018; 64: 304-311. [DOI:10.1093/tropej/fmx067] [PMID]
12. Abebe S, Gebru G, Amenu D, Mekonnen Z, Dube L. Risk factors associated with congenital anomalies among newborns in southwestern Ethiopia: A case-control study. PloS One 2021; 16: e0245915. [DOI:10.1371/journal.pone.0245915] [PMID] [PMCID]
13. World Health Organization. World health statistics. Switzerland: World Health Organization Press; 2015.
14. Cohen E, Horváth-Puhó E, Ray JG, Pedersen L, Adler N, Ording AG, et al. Association between the birth of an infant with major congenital anomalies and subsequent risk of mortality in their mothers. JAMA 2016; 316: 2515-2524. [DOI:10.1001/jama.2016.18425] [PMID]
15. Guimarães ALS, Barbosa CC, de Oliveira CM, Maia LTdS, de Bonfim CV. Relationship of databases of live births and infant deaths for analysis of congenital malformations. Rev Bras Saúde Mater Infant 2019; 19: 917-924. [DOI:10.1590/1806-93042019000400010]
16. Cosme HW, Lima LS, Barbosa LG. Prevalence of congenital anomalies and their associated factors in newborns in the city of São Paulo from 2010 to 2014. Rev Paul Pediatr 2017; 35: 33-38. [DOI:10.1590/1984-0462/;2017;35;1;00002] [PMID] [PMCID]
17. Nezami A, Heidari G, Tarhani F, Kariminia M. Prevalence of congenital heart disease among children in Khorramabad (West of Iran). Cardiovasc Haematol Disord Drug Targets 2021; 21: 61-65. [DOI:10.2174/1871529X20999201231205746] [PMID]
18. Liu Y, Chen S, Zühlke L, Black GC, Choy M-K, Li N, et al. Global birth prevalence of congenital heart defects 1970-2017: Updated systematic review and meta-analysis of 260 studies. Int J Epidemiol 2019; 48: 455-463. [DOI:10.1093/ije/dyz009] [PMID] [PMCID]
19. Amini-Rarani M, Vahedi S, Borjali M, Nosratabadi M. Socioeconomic inequality in congenital heart diseases in Iran. Int J Equity Health 2021; 20: 251. [DOI:10.1186/s12939-021-01591-3] [PMID] [PMCID]
20. Derakhshan R, Raeisi N, Sadeghi T. Prevalence of congenital heart disease and related factors among children admitted to the pediatric cardiac center in Rafsanjan, Southeastern Iran. Novelty Clin Med 2022; 1: 121-126.
21. Salari N, Darvishi N, Heydari M, Bokaee Sh, Darvishi F, Mohammadi M. Global prevalence of cleft palate, cleft lip and cleft palate and lip: A comprehensive systematic review and meta-analysis. J Stomatol Oral Maxillofac Surg 2022; 123: 110-120. [DOI:10.1016/j.jormas.2021.05.008] [PMID]
22. Hays T, Thompson MV, Bateman DA, Sahni R, Tolia VN, Clark RH, et al. The prevalence and clinical significance of congenital anomalies of the kidney and urinary tract in preterm infants. JAMA Netw Open 2022; 5: e2231626. [DOI:10.1001/jamanetworkopen.2022.31626] [PMID] [PMCID]
23. ElAwady H, AlGameel A, Ragab T, Hassan N. Congenital anomalies in neonates in Fayoum Governorate, Egypt. East Mediterr Health J 2021; 27: 790-797. [DOI:10.26719/emhj.21.033] [PMID]
24. Oniya O, Neves K, Ahmed B, Konje JC. A review of the reproductive consequences of consanguinity. Eur J Obstet Gynecol Reprod Biol 2019; 232: 87-96. [DOI:10.1016/j.ejogrb.2018.10.042] [PMID]
25. Reis LC, Murillo Vizcardo LE, Maia Coutinho F, Fadi Geha Y, Da Silva Júnior WF, Arante T, et al. Consanguinity and genetic diseases in Brazil: An overview. Int J Med Rev 2023; 10: 435-446.
26. Hosseini-Chavoshi M, Abbasi-Shavazi MJ, Bittles AH. Consanguineous marriage, reproductive behaviour and postnatal mortality in contemporary Iran. Hum Hered 2014; 77: 16-25. [DOI:10.1159/000358403] [PMID]
27. Kaviany N, Sedehi M, Golalipour E, Aryaie M, Golalipour MJ. Birth defects and parental consanguinity in the north of Iran. BJMMR 2016; 16: 1-7. [DOI:10.9734/BJMMR/2016/26374] [PMID]
28. Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, et al. Williams obstetrics. 24th Ed. New York: McGraw-Hill Education/Medical; 2014.
29. Zaganjor I, Sekkarie A, Tsang BL, Williams J, Razzaghi H, Mulinare J, et al. Describing the prevalence of neural tube defects worldwide: A systematic literature review. PloS One 2016; 11: e0151586. [DOI:10.1371/journal.pone.0151586] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
