
International Journal of
Reproductive Biomedicine
Tue, Aug 4, 2026
[Archive]
Volume 24, Issue 3 (March 2026)
IJRM 2026, 24(3): 231-244 |
Back to browse issues page


Ethics code: IR.BUMS.REC.1401.247
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezghi S, Hazari V, Dastjerdi R, Salehiniya H. Evaluation of coping mechanisms and depression, anxiety, and stress in women with infertility: A cross-sectional study. IJRM 2026; 24 (3) :231-244
URL: http://ijrm.ir/article-1-3385-en.html
URL: http://ijrm.ir/article-1-3385-en.html



1- Department of Obstetrics and Gynecology, Faculty of Medicine, Birjand University of Medical Sciences, Birjand, Iran.
2- Department of Obstetrics and Gynecology, School of Medicine, Rooyesh Infertility Center, Cellular and Molecular Research Center, Birjand University of Medical Sciences, Birjand, Iran. & Department of Obstetrics and Gynecology, School of Medicine, Clinical Research Development Unit (CRDU), Valiasr Hospital, Birjand University of Medical Sciences, Birjand, Iran. ,dr.vhazari@gmail.com; vajihehazari@bums.ac.ir
3- Department of General Courses, School of Medicine, Cardiovascular Diseases Research Center, Birjand University of Medical Sciences, Birjand, Iran.
4- Department of Epidemiology and Biostatistics, School of Health, Social Determinants of Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
2- Department of Obstetrics and Gynecology, School of Medicine, Rooyesh Infertility Center, Cellular and Molecular Research Center, Birjand University of Medical Sciences, Birjand, Iran. & Department of Obstetrics and Gynecology, School of Medicine, Clinical Research Development Unit (CRDU), Valiasr Hospital, Birjand University of Medical Sciences, Birjand, Iran. ,
3- Department of General Courses, School of Medicine, Cardiovascular Diseases Research Center, Birjand University of Medical Sciences, Birjand, Iran.
4- Department of Epidemiology and Biostatistics, School of Health, Social Determinants of Health Research Center, Birjand University of Medical Sciences, Birjand, Iran.
Full-Text [PDF 430 kb]
(306 Downloads)
| Abstract (HTML) (463 Views)

4. Discussion
In the present study which the relationship between the score of using coping mechanisms in women with infertility and the prevalence of psychological symptoms in them was investigated, the most common causes of infertility were unknown and followed by ovarian problems, male, uterine, and tubal factors. According to a study in 2019, 46.6% of infertility causes were attributed to female factors, with polycystic ovary syndrome reported as the most common ovarian cause of infertility (46%) (20). Contrary to the findings of the current study, in a study by Mazzilli et al. male factors were involved in half of the infertile couples (21).
Based on the results of the current study, approximately 32% of individuals had primary infertility, while secondary infertility was present in 68% of individuals. In a study in 2019, the prevalence of primary infertility was 57.5% compared to 42.5% for secondary infertility (20). Additionally, other studies in Iran have shown that the occurrence of primary infertility was higher than that of secondary infertility (22). Consistent with the findings of the current study, it was shown that 59% of women in the study were diagnosed with secondary infertility (23). The higher prevalence of primary infertility observed in developing countries has been attributed to a higher incidence of sexually transmitted infections, inadequate treatment of such infections, complications of unsafe abortions, and maternal sepsis (24).
According to the findings of the current study, approximately 55-60% of the women enrolled in the study exhibited some level of depression, anxiety, and stress. In this regard, a study found that there is a correlation between stress, quality of life, and reproductive functions in women in intimate relationships. This vicious cycle suggests that infertility is associated with stress, and stress is associated with quality of life, indicating a meaningful relationship between infertility, stress, and quality of life (25).
The results of the current study showed that individuals who employed problem-focused coping strategies in dealing with problems experienced lower levels of depression, anxiety, and stress. Since this coping style leads to the resolution or fundamental improvement of issues and problems, it demonstrates its positive effects in the long term and results in a reduction in the levels of depression, anxiety, and stress in women with infertility (26). Therefore, it is recommended to focus on social support structures and problem-focused coping strategies in the management of stress related to infertility. Contrary to the findings of the present study, it was shown that no significant difference existed between infertility distress and problem-focused coping styles (27).
In our study, women who employed an emotion-focused coping style experienced higher levels of depression and anxiety but lower levels of stress. Hence, this factor may have had an impact on the results obtained. In the current study, no significant relationship was observed between an avoidance coping style and the levels of depression, anxiety, and stress. It can be pointed out that individuals using emotion-focused coping tend to have lower levels of stress because they are not taking action but rather trying to soothe themselves and reduce their distress. However, as this coping style does not lead to fundamental problem-solving, in the long term, these individuals may experience higher levels of depression and anxiety (28). According to a study in Shiraz, unlike the findings of the present study, they demonstrated that women with infertility using an avoidance coping style experienced lower levels of infertility distress (29).
Generally, coping ability in women with infertility is related to personal resources such as mental well-being and having good skills to deal with the issue. Coping is also positively influenced by the ability to adapt to a childless life, including comforting thoughts, doing things that bring relief and orienting thinking toward the future (30).
In this study, household income showed a significant positive association with depression and stress scores among women with infertility. In contrast, prior researches in low- and middle-income countries links lower household income to greater psychological burden. This is typically explained by high treatment costs (e.g., in vitro fertilization), limited access to quality care, and additional socioeconomic stressors that amplify the emotional impact of infertility. Systematic reviews and cross-sectional studies often find that higher-income women experience lower depression and stress levels due to better affordability of treatment and greater access to support (31-35). However, the current finding aligns with a minority of studies reporting elevated distress among higher socioeconomic groups. Possible explanations include pursuit of more intensive and prolonged treatments, leading to greater emotional investment, repeated cycle failures, and intensified feelings of failure (36). Additionally, conflicts between demanding careers and treatment demands may increase work-life interference, guilt, and stress from delayed professional goals. In some cultural contexts, infertility may evoke stronger stigma or self-blame in affluent groups, where childbearing is tied to social identity and success (37).
4.1. Strengths and Limitations
A: The nature of the study (cross-sectional), which limits the examination of causal relationships. B: Investigated a single center. C: Not investigating variables such as length of marriage and duration of treatment.
5. Conclusion
Based on the study results, approximately half of the participants experienced some level of disturbance in the areas of depression, anxiety, and stress. The emotion -focused strategy showed a higher correlation in predicting depression, stress, and anxiety in women with infertility. Therefore, it seems implementing coping mechanisms is effective in controlling psychological symptoms in women with infertility. Implementation of longitudinal and multicenter studies with controlling factors such as length of marriage, type of infertility and duration of treatment for investigating long- and short-term solutions are necessary.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
S. Rezghi, V. Hazari, R. Dastjerdi, and H. Salehiniya had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: R. Dastjerdi. Acquisition, analysis, or interpretation of data: S. Rezghi, V. Hazari, R. Dastjerdi, H. Salehiniya. Drafting of the manuscript: S. Rezghi, V. Hazari. Critical revision of the manuscript for important intellectual content: S. Rezghi, V. Hazari, R. Dastjerdi, H. Salehiniya. Statistical analysis: H. Salehiniya. Supervision: V. Hazari.
Acknowledgements
This study was not financially supported. We did not use artificial intelligence in writing this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Full-Text: (46 Views)
1. Introduction
Infertility is a distressing and unexpected experience which is defined as the failure to achieve pregnancy after 1 yr of regular unprotected sexual intercourse (1). It is classified into primary infertility (never having a biological child) and secondary infertility (inability to conceive after a previous pregnancy). Globally, there are 48.5 million infertile couples, while in Iran, the average prevalence is 7.88% (2). The causes include sperm dysfunction, ovulation disorders, tubal damage due to infection, endometriosis, sexual dysfunction, cervical mucus abnormalities, uterine abnormalities, and unknown factors (3).
Individuals experiencing infertility may face psychological challenges such as anxiety, feelings of inadequacy, anger, depression, jealousy, decreased self-esteem, obsessive thoughts, and personality disorders (4). Particularly in traditional societies, women may face more significant familial, social, economic, and personal challenges than men (5). It is reported that infertile women have twice higher prevalence of psychiatric disorders compared to fertile women, and approximately 32% are at risk of mental health problems (6).
Stress is an inevitable aspect of human life and occurs when the psychological pressure placed on an individual exceeds their ability to cope with appropriate coping strategies. It serves as a warning signal for preparing the body for a suitable and effective response characterized by heightened focus, strength, and alertness (7). Anxiety is a feeling of unease and fear in the presence or absence of a stressful situation (8). Depression is characterized by low mood, feelings of worthlessness, and a decrease in pleasure and enthusiasm for enjoyable activities. It is more common among women experiencing infertility compared to the general population (9) and can reduced sexual pleasure, diminished self-confidence, feelings of rejection, and decreased intimacy within the marital relationship (10). An analysis conducted in 2015 demonstrated a significant reduction in anxiety levels with improved fertility rates (11). Therefore, disregarding the emotional disorders and other undesirable consequences of infertility can hurt the treatment of infertile couples (4, 12).
In contrast, social support can contribute to the improvement of mental health and protect individuals against stress-related challenges, leading to a reduction in stress and anxiety (13). Individuals' reactions to stressful situations depend on the coping strategies they employ, which can be problem-focused, emotion-focused, or avoidance-based (14). It has been reported that most individuals tend to use emotion-focused coping strategies in stressful situations to alleviate their stress temporarily (15).
Therefore, given the high prevalence of infertility and the importance of reducing its psychological consequences (and also considering that no study has been conducted so far on the use of effective strategies to control psychological symptoms in women with infertility in eastern Iran) this study aimed to investigate the relationship between the score of using coping mechanisms in women with infertility referring to the infertility treatment center of Birjand University of Medical Sciences, Birjand, Iran and the prevalence of psychological symptoms in them.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study was conducted on 386 women with infertility who were referred to Rooyesh Infertility Center, Birjand, Iran, from October 2022 to March 2023.
2.2. Eligibility criteria
The inclusion criteria included women aged between 18 and 42 yr, who were diagnosed with infertility.
Exclusion criteria included individuals with a diagnosed psychological disorder (depression, anxiety, and stress) or a history of psychiatric medication related to investigated disorders used for these conditions, those with incomplete file information, and parents who were legal guardians of foster children.
2.3. Data collection
The participants who entered the study completed 3 questionnaires: a demographic information questionnaire, an Endler and Parker coping with stressful situations questionnaire, and the depression, anxiety, and stress scale (DASS-21) questionnaire (16).
The demographic information questionnaire includes the following items: age, educational level of the woman, educational level of the spouse, employment status, and income level. Cause of infertility, duration of infertility, presence of endometriosis, and type of infertility (primary or secondary).
The second questionnaire was the coping with stressful situations questionnaire, which was developed by Endler and Parker in 1990 to assess different coping styles in stressful situations. It was designed in 3 forms: problem-focused coping style, emotion-focused coping style, and avoidance coping style.
Cronbach's alpha for each of them was 0.86, 0.84, and 0.80. It consists of 48 questions, and each question was rated on a 5-point Likert scale ranging from "never" (1) to "very often" (5). It should be noted that the dominant coping style of each individual was determined based on their scores in each of the 3 dimensions of coping styles. The total score range was between 48 and 240 (17).
To measure the level of psychological symptoms, DASS-21 was used. Cronbach's alpha coefficient for each subscale (anxiety, depression, and stress) was 0.77, 0.79, and 0.78. Each of the DASS subscales consists of 7 questions. Each question was scored on a scale of 0 (not true of me at all) to 3 (very true of me), and the final score for each subscale was obtained by summing the scores of the corresponding questions. According to the manual, the resulting ratings are classified as: “normal, mild, moderate, severe, or extremely severe”.
The total score range varies from 0-63. The DASS-21 was administered to 1070 Iranians. Internal reliabilities for the 3 DASS subscales ranged from +0.77 to +0.79. The validity of DASS was measured using factor analysis and criterion validity. The correlation between the depression subscale and the Beck depression inventory scale was +0.70. Between the anxiety subscale and Zung anxiety inventory was +0.67, and between the stress subscale and perceived stress inventory was +0.49. All correlations were significant (16).
2.4. Sample size
Based on the results of the study by Yousefi Sharami et al. (18), and considering the prevalence of depression in women with infertility as 15%, the prevalence of anxiety as 30%, an α = 0.05 and d = 0.05, and using the Cochran formula. In addition, based on the study by Koraei et al. (19), considering a standard deviation (SD) = 10 for coping strategies, an α = 0.05 and d = 1, and using then = z 2 s 2 d 2
Given that there is only one infertility treatment center in Birjand, patients were selected through an available sampling method based on inclusion and exclusion criteria.
2.5. Ethical Considerations
This study was approved by the ethics committee of Birjand University of Medical Sciences, Birjand, Iran (Code: IR.BUMS.REC.1401.247). Informed written consent was obtained from each participant.
2.6. Statistical Analysis
The data were entered into the Statistical Package for the Social Sciences, version 17.0, SPSS Inc., Chicago, Illinois, USA (SPSS) after collection. Mean, SD and frequency distribution tables were used to describe the data. After confirming the normality of the data by the Kolmogorov-Smirnov test, independent t test, analysis of variance (ANOVA), Pearson correlation coefficient, and linear regression test were used to examine the relationship between variables. A significance level of < 0.05 was considered.
3. Results
3.1. Description of participants' initial characteristics
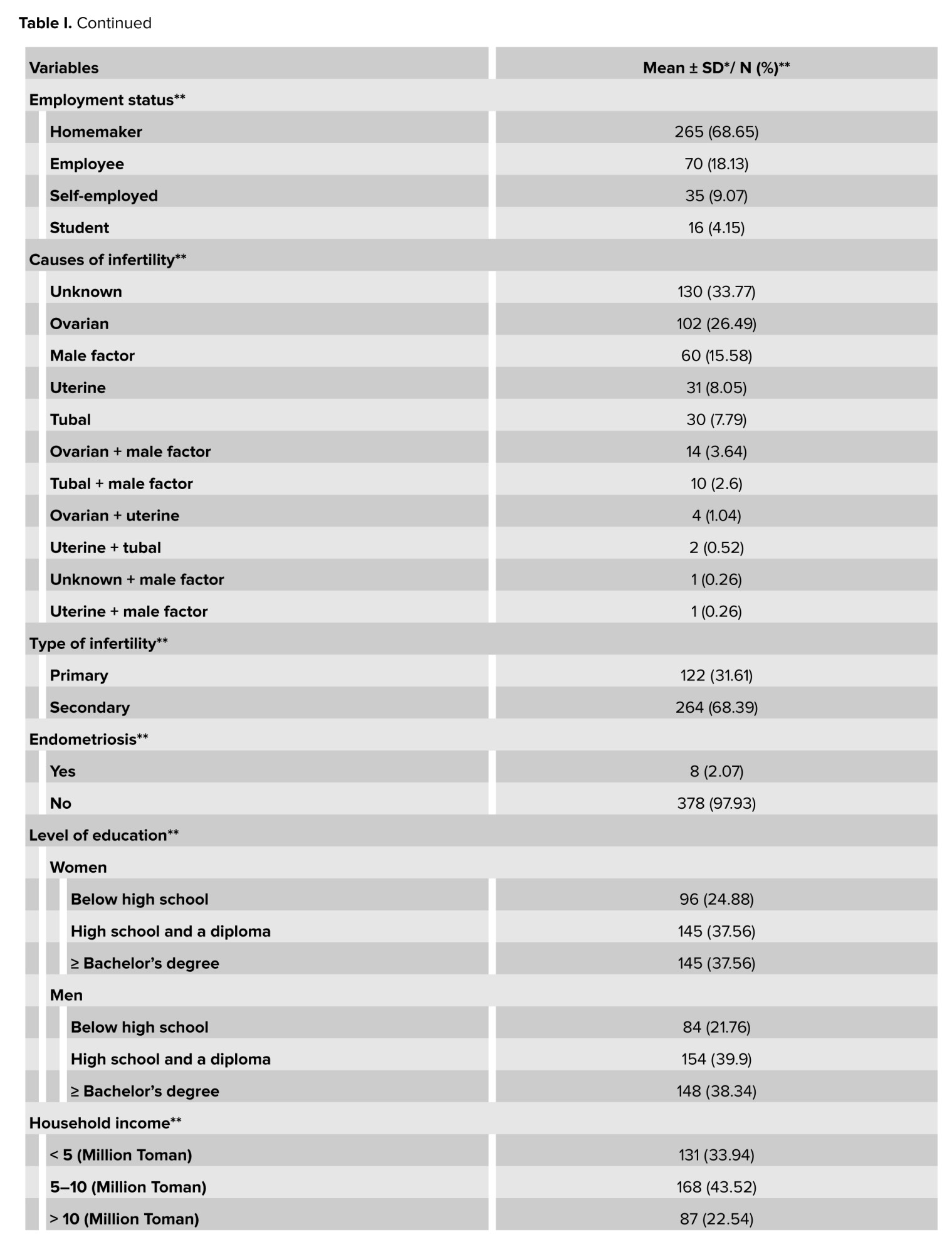
The participants had a mean age of 30.11 ± 5.92 yr and a mean infertility duration of 4.63 ± 3.59 yr. The majority were homemakers (68.65%), presented with primary infertility (31.61%), and had unexplained infertility (33.77%), while endometriosis was identified in 2.07% of cases. Educational attainment was relatively high, with only 24.88% of women and 21.76% of men having less than a high school education. Most households (43.52%) reported a monthly income of 5-10 million Iranian Toman (Table I).
3.2. Determining the mean scores of psychological symptoms in women with infertility
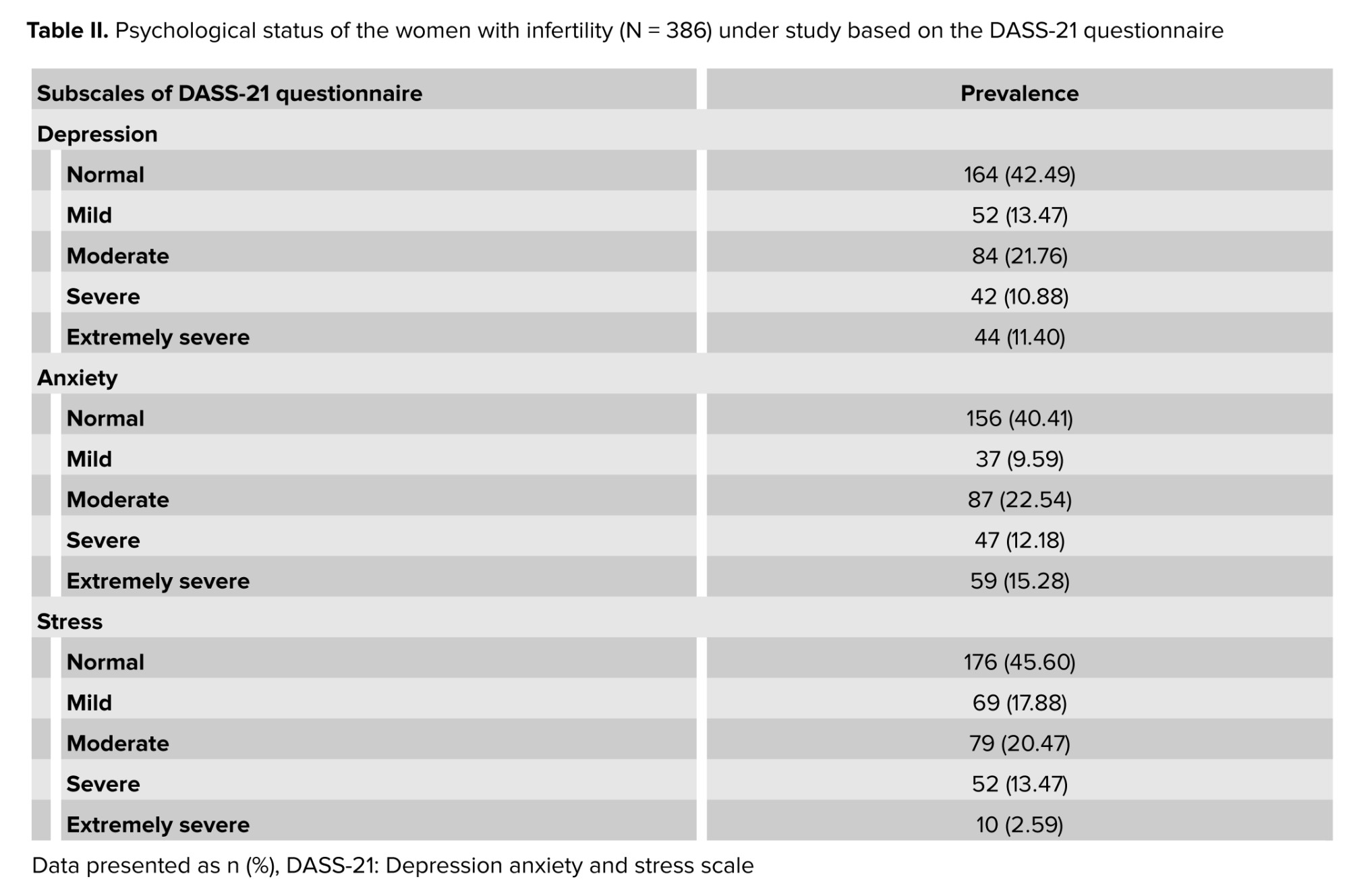
The study findings revealed that 52.51% of participants experienced some level of depression, with 22.28% classified as having severe or extremely severe depression. Additionally, 59.59% of the women surveyed reported experiencing some degree of anxiety, while 27.46% had severe or extremely severe anxiety. Furthermore, 54.40% of participants indicated they were stressed, with 16.06% suffering from severe or extremely severe stress (Table II).
3.3. Determining the mean scores of coping strategies in women with infertility
The participants' coping strategies, as assessed by the coping with stressful situations questionnaire, yielded mean scores of 46.83 ± 11.36 for problem-focused coping, 40.11 ± 11.29 for emotion-focused coping, and 41.49 ± 9.56 for avoidance coping. These findings indicate that the majority of participants predominantly employed problem-focused strategies when dealing with stressful situations.
3.4. Determining the mean scores of psychological symptoms and coping strategies in women with infertility based on demographic variables
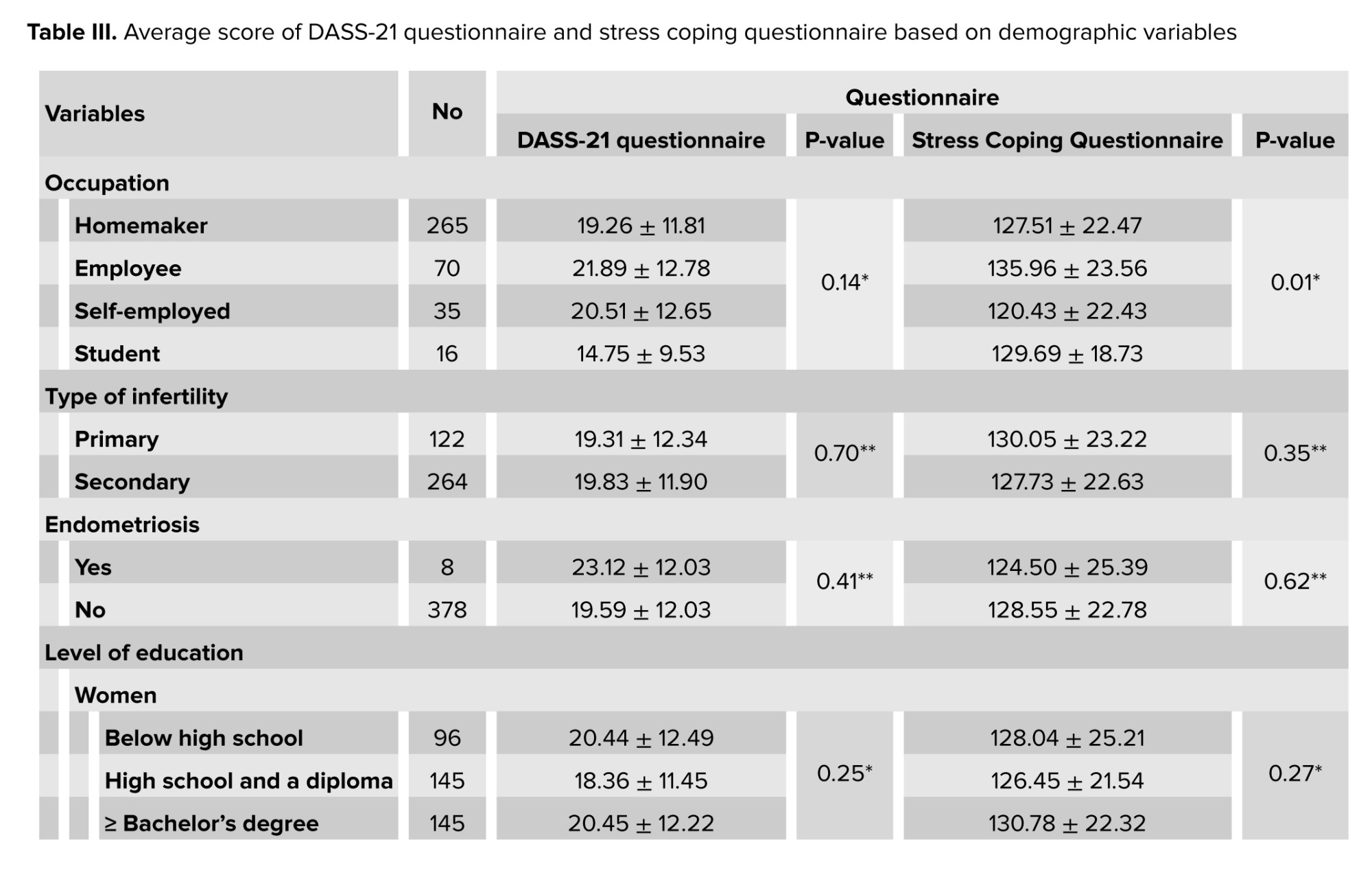
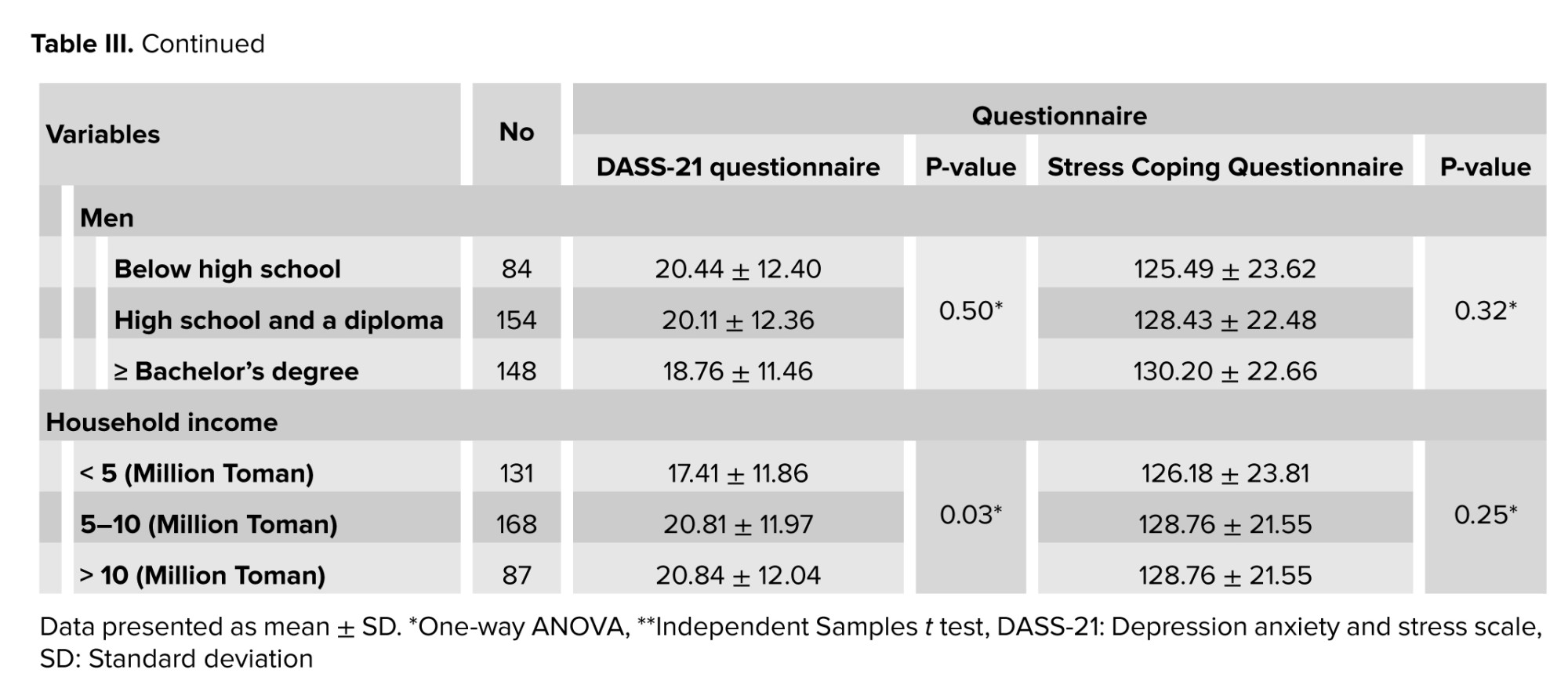
One-way ANOVA revealed no significant differences in DASS-21 scores across occupation (p = 0.14), type of infertility (p = 0.14), women's educational level (p = 0.25), or men's educational level (p = 0.50). However, household income significantly influenced DASS-21 scores (p = 0.03), with the lowest scores observed in households earning ≤ 5 million Toman monthly. Independent samples t tests indicated no significant association between DASS-21 scores and the presence of endometriosis (p = 0.41) or type of infertility (p = 0.70) (Table III). Therefore, in the studied population, factors such as job, type of infertility, women's education level, type of endometriosis and type of infertility had no effect on stress, anxiety and depression in infertile women. But household income affected the stress, anxiety and depression level; in the household with lower income, the infertile women endured more stress, anxiety and depression.
The one-way ANOVA revealed a significant effect of occupation on coping with stressful situations scores (p = 0.01), with employees exhibiting the highest mean score (135.96 ± 23.56). No significant associations were found for other demographic variables, including women's educational level (p = 0.27), men's educational level (p = 0.32), and household income (p = 0.35). Additionally, independent samples t tests indicated no significant differences in coping scores based on the presence of endometriosis (p = 0.62) or type of infertility (p = 0.27) (Table III).
3.5. Determining the correlation between coping strategies and psychological indicators in women with infertility
The results showed that there was a significant linear weak negative correlation between problem-focused and depression (r = -0.20, p < 0.001), anxiety (r = -0.14, p = 0.01), and stress (r = -0.20, p < 0.001). These results indicate that in women studied, those who have used problem-solving method as coping strategies to manage their infertility challenges have a better mental health. There was a significant linear moderate positive correlation between emotion-focused and depression (r = 0.56, p < 0.001) and anxiety (r = 0.54, p < 0.001). These results show those who have used emotion-focused strategies have a higher depression. However, there was a significant linear moderate negative correlation between emotion-focused and stress (r = -0.61, p < 0.001). These results indicate that in women studied, those who have used emotion-focused method experienced lower stress. Avoidant and depression (r = -0.04, p = 0.45), anxiety (r = 0.05, p = 0.34), and stress (r = -0.04, p = 0.47) did not show significant linear correlation and didn’t affect the mental health in studied women.
3.6. Determining the relation between coping strategies and psychological indicators in women with infertility based on linear regression test (backward method)
As presented in table IV, based on the results of the linear regression test, problem-focused and emotion-focused aspects of coping strategies were identified as factors affecting psychological indicators (p < 0.05) and anxiety score (p < 0.05). Also, problem-focused, emotion-focused, and avoidant aspects of coping strategies and household income were identified as factors affecting depression score (p < 0.05) and stress score (p < 0.05) in women with infertility. Multiple linear regression analysis (backward method) revealed that the following factors were significantly associated with the DASS-21 total score and its subscales among women with infertility:
Infertility is a distressing and unexpected experience which is defined as the failure to achieve pregnancy after 1 yr of regular unprotected sexual intercourse (1). It is classified into primary infertility (never having a biological child) and secondary infertility (inability to conceive after a previous pregnancy). Globally, there are 48.5 million infertile couples, while in Iran, the average prevalence is 7.88% (2). The causes include sperm dysfunction, ovulation disorders, tubal damage due to infection, endometriosis, sexual dysfunction, cervical mucus abnormalities, uterine abnormalities, and unknown factors (3).
Individuals experiencing infertility may face psychological challenges such as anxiety, feelings of inadequacy, anger, depression, jealousy, decreased self-esteem, obsessive thoughts, and personality disorders (4). Particularly in traditional societies, women may face more significant familial, social, economic, and personal challenges than men (5). It is reported that infertile women have twice higher prevalence of psychiatric disorders compared to fertile women, and approximately 32% are at risk of mental health problems (6).
Stress is an inevitable aspect of human life and occurs when the psychological pressure placed on an individual exceeds their ability to cope with appropriate coping strategies. It serves as a warning signal for preparing the body for a suitable and effective response characterized by heightened focus, strength, and alertness (7). Anxiety is a feeling of unease and fear in the presence or absence of a stressful situation (8). Depression is characterized by low mood, feelings of worthlessness, and a decrease in pleasure and enthusiasm for enjoyable activities. It is more common among women experiencing infertility compared to the general population (9) and can reduced sexual pleasure, diminished self-confidence, feelings of rejection, and decreased intimacy within the marital relationship (10). An analysis conducted in 2015 demonstrated a significant reduction in anxiety levels with improved fertility rates (11). Therefore, disregarding the emotional disorders and other undesirable consequences of infertility can hurt the treatment of infertile couples (4, 12).
In contrast, social support can contribute to the improvement of mental health and protect individuals against stress-related challenges, leading to a reduction in stress and anxiety (13). Individuals' reactions to stressful situations depend on the coping strategies they employ, which can be problem-focused, emotion-focused, or avoidance-based (14). It has been reported that most individuals tend to use emotion-focused coping strategies in stressful situations to alleviate their stress temporarily (15).
Therefore, given the high prevalence of infertility and the importance of reducing its psychological consequences (and also considering that no study has been conducted so far on the use of effective strategies to control psychological symptoms in women with infertility in eastern Iran) this study aimed to investigate the relationship between the score of using coping mechanisms in women with infertility referring to the infertility treatment center of Birjand University of Medical Sciences, Birjand, Iran and the prevalence of psychological symptoms in them.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study was conducted on 386 women with infertility who were referred to Rooyesh Infertility Center, Birjand, Iran, from October 2022 to March 2023.
2.2. Eligibility criteria
The inclusion criteria included women aged between 18 and 42 yr, who were diagnosed with infertility.
Exclusion criteria included individuals with a diagnosed psychological disorder (depression, anxiety, and stress) or a history of psychiatric medication related to investigated disorders used for these conditions, those with incomplete file information, and parents who were legal guardians of foster children.
2.3. Data collection
The participants who entered the study completed 3 questionnaires: a demographic information questionnaire, an Endler and Parker coping with stressful situations questionnaire, and the depression, anxiety, and stress scale (DASS-21) questionnaire (16).
The demographic information questionnaire includes the following items: age, educational level of the woman, educational level of the spouse, employment status, and income level. Cause of infertility, duration of infertility, presence of endometriosis, and type of infertility (primary or secondary).
The second questionnaire was the coping with stressful situations questionnaire, which was developed by Endler and Parker in 1990 to assess different coping styles in stressful situations. It was designed in 3 forms: problem-focused coping style, emotion-focused coping style, and avoidance coping style.
Cronbach's alpha for each of them was 0.86, 0.84, and 0.80. It consists of 48 questions, and each question was rated on a 5-point Likert scale ranging from "never" (1) to "very often" (5). It should be noted that the dominant coping style of each individual was determined based on their scores in each of the 3 dimensions of coping styles. The total score range was between 48 and 240 (17).
To measure the level of psychological symptoms, DASS-21 was used. Cronbach's alpha coefficient for each subscale (anxiety, depression, and stress) was 0.77, 0.79, and 0.78. Each of the DASS subscales consists of 7 questions. Each question was scored on a scale of 0 (not true of me at all) to 3 (very true of me), and the final score for each subscale was obtained by summing the scores of the corresponding questions. According to the manual, the resulting ratings are classified as: “normal, mild, moderate, severe, or extremely severe”.
The total score range varies from 0-63. The DASS-21 was administered to 1070 Iranians. Internal reliabilities for the 3 DASS subscales ranged from +0.77 to +0.79. The validity of DASS was measured using factor analysis and criterion validity. The correlation between the depression subscale and the Beck depression inventory scale was +0.70. Between the anxiety subscale and Zung anxiety inventory was +0.67, and between the stress subscale and perceived stress inventory was +0.49. All correlations were significant (16).
2.4. Sample size
Based on the results of the study by Yousefi Sharami et al. (18), and considering the prevalence of depression in women with infertility as 15%, the prevalence of anxiety as 30%, an α = 0.05 and d = 0.05, and using the Cochran formula. In addition, based on the study by Koraei et al. (19), considering a standard deviation (SD) = 10 for coping strategies, an α = 0.05 and d = 1, and using the
Given that there is only one infertility treatment center in Birjand, patients were selected through an available sampling method based on inclusion and exclusion criteria.
2.5. Ethical Considerations
This study was approved by the ethics committee of Birjand University of Medical Sciences, Birjand, Iran (Code: IR.BUMS.REC.1401.247). Informed written consent was obtained from each participant.
2.6. Statistical Analysis
The data were entered into the Statistical Package for the Social Sciences, version 17.0, SPSS Inc., Chicago, Illinois, USA (SPSS) after collection. Mean, SD and frequency distribution tables were used to describe the data. After confirming the normality of the data by the Kolmogorov-Smirnov test, independent t test, analysis of variance (ANOVA), Pearson correlation coefficient, and linear regression test were used to examine the relationship between variables. A significance level of < 0.05 was considered.
3. Results
3.1. Description of participants' initial characteristics
The participants had a mean age of 30.11 ± 5.92 yr and a mean infertility duration of 4.63 ± 3.59 yr. The majority were homemakers (68.65%), presented with primary infertility (31.61%), and had unexplained infertility (33.77%), while endometriosis was identified in 2.07% of cases. Educational attainment was relatively high, with only 24.88% of women and 21.76% of men having less than a high school education. Most households (43.52%) reported a monthly income of 5-10 million Iranian Toman (Table I).
3.2. Determining the mean scores of psychological symptoms in women with infertility
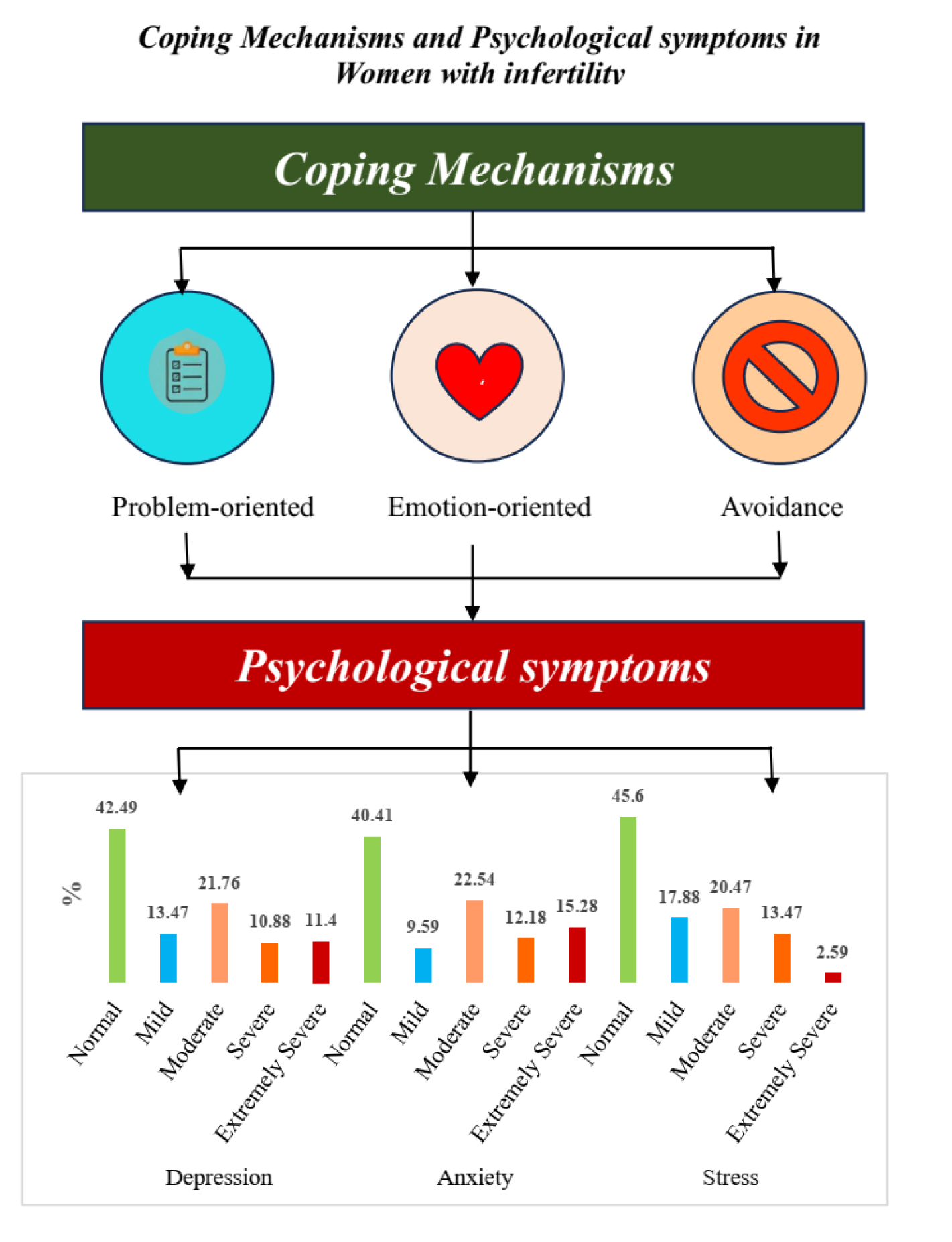
The study findings revealed that 52.51% of participants experienced some level of depression, with 22.28% classified as having severe or extremely severe depression. Additionally, 59.59% of the women surveyed reported experiencing some degree of anxiety, while 27.46% had severe or extremely severe anxiety. Furthermore, 54.40% of participants indicated they were stressed, with 16.06% suffering from severe or extremely severe stress (Table II).
3.3. Determining the mean scores of coping strategies in women with infertility
The participants' coping strategies, as assessed by the coping with stressful situations questionnaire, yielded mean scores of 46.83 ± 11.36 for problem-focused coping, 40.11 ± 11.29 for emotion-focused coping, and 41.49 ± 9.56 for avoidance coping. These findings indicate that the majority of participants predominantly employed problem-focused strategies when dealing with stressful situations.
3.4. Determining the mean scores of psychological symptoms and coping strategies in women with infertility based on demographic variables
One-way ANOVA revealed no significant differences in DASS-21 scores across occupation (p = 0.14), type of infertility (p = 0.14), women's educational level (p = 0.25), or men's educational level (p = 0.50). However, household income significantly influenced DASS-21 scores (p = 0.03), with the lowest scores observed in households earning ≤ 5 million Toman monthly. Independent samples t tests indicated no significant association between DASS-21 scores and the presence of endometriosis (p = 0.41) or type of infertility (p = 0.70) (Table III). Therefore, in the studied population, factors such as job, type of infertility, women's education level, type of endometriosis and type of infertility had no effect on stress, anxiety and depression in infertile women. But household income affected the stress, anxiety and depression level; in the household with lower income, the infertile women endured more stress, anxiety and depression.
The one-way ANOVA revealed a significant effect of occupation on coping with stressful situations scores (p = 0.01), with employees exhibiting the highest mean score (135.96 ± 23.56). No significant associations were found for other demographic variables, including women's educational level (p = 0.27), men's educational level (p = 0.32), and household income (p = 0.35). Additionally, independent samples t tests indicated no significant differences in coping scores based on the presence of endometriosis (p = 0.62) or type of infertility (p = 0.27) (Table III).
3.5. Determining the correlation between coping strategies and psychological indicators in women with infertility
The results showed that there was a significant linear weak negative correlation between problem-focused and depression (r = -0.20, p < 0.001), anxiety (r = -0.14, p = 0.01), and stress (r = -0.20, p < 0.001). These results indicate that in women studied, those who have used problem-solving method as coping strategies to manage their infertility challenges have a better mental health. There was a significant linear moderate positive correlation between emotion-focused and depression (r = 0.56, p < 0.001) and anxiety (r = 0.54, p < 0.001). These results show those who have used emotion-focused strategies have a higher depression. However, there was a significant linear moderate negative correlation between emotion-focused and stress (r = -0.61, p < 0.001). These results indicate that in women studied, those who have used emotion-focused method experienced lower stress. Avoidant and depression (r = -0.04, p = 0.45), anxiety (r = 0.05, p = 0.34), and stress (r = -0.04, p = 0.47) did not show significant linear correlation and didn’t affect the mental health in studied women.
3.6. Determining the relation between coping strategies and psychological indicators in women with infertility based on linear regression test (backward method)
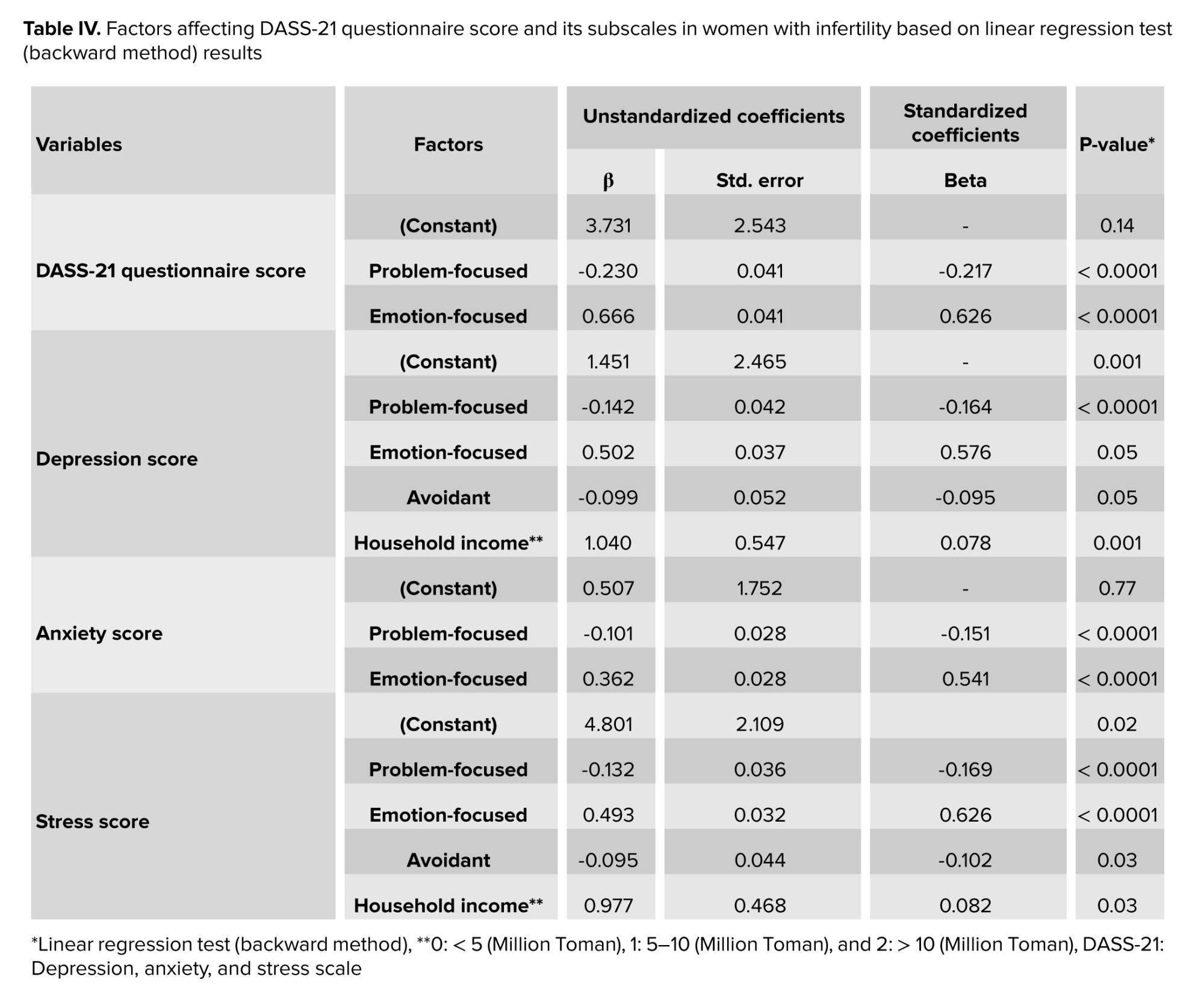
As presented in table IV, based on the results of the linear regression test, problem-focused and emotion-focused aspects of coping strategies were identified as factors affecting psychological indicators (p < 0.05) and anxiety score (p < 0.05). Also, problem-focused, emotion-focused, and avoidant aspects of coping strategies and household income were identified as factors affecting depression score (p < 0.05) and stress score (p < 0.05) in women with infertility. Multiple linear regression analysis (backward method) revealed that the following factors were significantly associated with the DASS-21 total score and its subscales among women with infertility:
- For the total DASS-21 score: problem-focused coping (p < 0.0001) and emotion-focused coping (p < 0.0001) were identified as significant predictors.
- For the depression subscale: problem-focused coping (p < 0.0001), emotion-focused coping (p = 0.050), avoidant coping (p = 0.050), and household income (p = 0.001) emerged as significant contributing factors.
- The anxiety subscale was significantly influenced by problem-focused coping (p < 0.0001) and emotion-focused coping (p < 0.0001).
- The stress subscale was significantly predicted by problem-focused coping (p < 0.0001), emotion-focused coping (p < 0.0001), avoidant coping (p = 0.033), and household income (p = 0.038).
- Overall, emotion-focused coping strategies exhibited the strongest positive and significant association with higher scores on depression, anxiety, stress, and the total DASS-21. In contrast, problem-focused coping was consistently associated with lower scores across all subscales and the total score. Household income also demonstrated a significant positive relationship with depression and stress scores.
4. Discussion
In the present study which the relationship between the score of using coping mechanisms in women with infertility and the prevalence of psychological symptoms in them was investigated, the most common causes of infertility were unknown and followed by ovarian problems, male, uterine, and tubal factors. According to a study in 2019, 46.6% of infertility causes were attributed to female factors, with polycystic ovary syndrome reported as the most common ovarian cause of infertility (46%) (20). Contrary to the findings of the current study, in a study by Mazzilli et al. male factors were involved in half of the infertile couples (21).
Based on the results of the current study, approximately 32% of individuals had primary infertility, while secondary infertility was present in 68% of individuals. In a study in 2019, the prevalence of primary infertility was 57.5% compared to 42.5% for secondary infertility (20). Additionally, other studies in Iran have shown that the occurrence of primary infertility was higher than that of secondary infertility (22). Consistent with the findings of the current study, it was shown that 59% of women in the study were diagnosed with secondary infertility (23). The higher prevalence of primary infertility observed in developing countries has been attributed to a higher incidence of sexually transmitted infections, inadequate treatment of such infections, complications of unsafe abortions, and maternal sepsis (24).
According to the findings of the current study, approximately 55-60% of the women enrolled in the study exhibited some level of depression, anxiety, and stress. In this regard, a study found that there is a correlation between stress, quality of life, and reproductive functions in women in intimate relationships. This vicious cycle suggests that infertility is associated with stress, and stress is associated with quality of life, indicating a meaningful relationship between infertility, stress, and quality of life (25).
The results of the current study showed that individuals who employed problem-focused coping strategies in dealing with problems experienced lower levels of depression, anxiety, and stress. Since this coping style leads to the resolution or fundamental improvement of issues and problems, it demonstrates its positive effects in the long term and results in a reduction in the levels of depression, anxiety, and stress in women with infertility (26). Therefore, it is recommended to focus on social support structures and problem-focused coping strategies in the management of stress related to infertility. Contrary to the findings of the present study, it was shown that no significant difference existed between infertility distress and problem-focused coping styles (27).
In our study, women who employed an emotion-focused coping style experienced higher levels of depression and anxiety but lower levels of stress. Hence, this factor may have had an impact on the results obtained. In the current study, no significant relationship was observed between an avoidance coping style and the levels of depression, anxiety, and stress. It can be pointed out that individuals using emotion-focused coping tend to have lower levels of stress because they are not taking action but rather trying to soothe themselves and reduce their distress. However, as this coping style does not lead to fundamental problem-solving, in the long term, these individuals may experience higher levels of depression and anxiety (28). According to a study in Shiraz, unlike the findings of the present study, they demonstrated that women with infertility using an avoidance coping style experienced lower levels of infertility distress (29).
Generally, coping ability in women with infertility is related to personal resources such as mental well-being and having good skills to deal with the issue. Coping is also positively influenced by the ability to adapt to a childless life, including comforting thoughts, doing things that bring relief and orienting thinking toward the future (30).
In this study, household income showed a significant positive association with depression and stress scores among women with infertility. In contrast, prior researches in low- and middle-income countries links lower household income to greater psychological burden. This is typically explained by high treatment costs (e.g., in vitro fertilization), limited access to quality care, and additional socioeconomic stressors that amplify the emotional impact of infertility. Systematic reviews and cross-sectional studies often find that higher-income women experience lower depression and stress levels due to better affordability of treatment and greater access to support (31-35). However, the current finding aligns with a minority of studies reporting elevated distress among higher socioeconomic groups. Possible explanations include pursuit of more intensive and prolonged treatments, leading to greater emotional investment, repeated cycle failures, and intensified feelings of failure (36). Additionally, conflicts between demanding careers and treatment demands may increase work-life interference, guilt, and stress from delayed professional goals. In some cultural contexts, infertility may evoke stronger stigma or self-blame in affluent groups, where childbearing is tied to social identity and success (37).
4.1. Strengths and Limitations
A: The nature of the study (cross-sectional), which limits the examination of causal relationships. B: Investigated a single center. C: Not investigating variables such as length of marriage and duration of treatment.
5. Conclusion
Based on the study results, approximately half of the participants experienced some level of disturbance in the areas of depression, anxiety, and stress. The emotion -focused strategy showed a higher correlation in predicting depression, stress, and anxiety in women with infertility. Therefore, it seems implementing coping mechanisms is effective in controlling psychological symptoms in women with infertility. Implementation of longitudinal and multicenter studies with controlling factors such as length of marriage, type of infertility and duration of treatment for investigating long- and short-term solutions are necessary.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
S. Rezghi, V. Hazari, R. Dastjerdi, and H. Salehiniya had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: R. Dastjerdi. Acquisition, analysis, or interpretation of data: S. Rezghi, V. Hazari, R. Dastjerdi, H. Salehiniya. Drafting of the manuscript: S. Rezghi, V. Hazari. Critical revision of the manuscript for important intellectual content: S. Rezghi, V. Hazari, R. Dastjerdi, H. Salehiniya. Statistical analysis: H. Salehiniya. Supervision: V. Hazari.
Acknowledgements
This study was not financially supported. We did not use artificial intelligence in writing this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
