
International Journal of
Reproductive Biomedicine
Mon, Jul 13, 2026
[Archive]
Volume 23, Issue 8 (August 2025)
IJRM 2025, 23(8): 613-626 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rakhshani Moghaddam F, Razavi M. Association between matrix metalloproteinase-9 polymorphism and the risk of preeclampsia: Evidence from an updated meta-analysis. IJRM 2025; 23 (8) :613-626
URL: http://ijrm.ir/article-1-3475-en.html
URL: http://ijrm.ir/article-1-3475-en.html



1- Department of Obstetrics and Gynecology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran.
2- Department of Obstetrics and Gynecology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran. & Health Promotion Research Center, Zahedan University of Medical Sciences, Zahedan, Iran. ,dr.razavi351@gmail.com; dr.razavi@zaums.ac.ir
2- Department of Obstetrics and Gynecology, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran. & Health Promotion Research Center, Zahedan University of Medical Sciences, Zahedan, Iran. ,
Full-Text [PDF 1530 kb]
(763 Downloads)
| Abstract (HTML) (873 Views)
Full-Text: (129 Views)
1. Introduction
Preeclampsia (PE) is a prevalent form of hypertension disorder of pregnancy (HDP) that happens after 20 wk of gestation. In clinical terms, augmented hypertension (systolic and diastolic blood pressure ≥ 140/90 mmHg) accompanied by proteinuria (≥ 300 mg within 24 hr) are diagnostic criteria for PE (1, 2). PE is blamed for the maternal and fetal mortality and morbidity, with the incidence ranging from 2-8% worldwide (3).
Several mechanisms have been implicated in the development of PE, including incomplete placental development and inadequate trophoblast invasion, oxidative stress, endothelial cell dysfunction, placental ischemia, and immune maladaptation (4, 5). Furthermore, genetic factors are supposed to have an important function in the etiology of PE (6-8). However, despite the numerous investigations regarding the etiology and pathogenesis of PE, the precise mechanisms are still undetermined (9).
Matrix metalloproteinase (MMPs) are known as extracellular proteinases and in such physiological and pathological mechanisms, including embryogenesis, implantation, formation of the placenta, tumor transformation, and neoangiogenesis, exert a significant function (10-13). Many cell types, such as immune cells, structural connective tissue cells, epithelial barrier cells, and phagocytic cells, are responsible for the secretion of MMPs (10). In PE cases, trophoblastic invasion might be influenced by altered MMP levels, which may further contribute to endothelial dysfunction through engaging with augmented oxidative stress and inflammatory mediators (14, 15).
MMP-9, also known as gelatinase B, is an important type of MMP family, which is mainly produced by monocytes, neutrophils, and vascular endothelial cells (16). Based on previous studies, in the serum of PE women, MMP-9 levels were increased (17, 18), and this finding was also observed in the umbilical cord plasma of newborns in mothers affected with PE (19). Several polymorphisms have been recognized in the MMP-9 gene, in which the MMP-9-1562 C>T (rs3918242) polymorphism is well studied in different disorders (20-23). This single-nucleotide polymorphism (SNP) is situated in the promoter region of the MMP-9 gene and is correlated with higher protein levels and higher transcriptional activity of MMP-9 (24). The MMP-9 genetic variations may lead to modifications in both protein structure and expression level (25).
Several studies investigated the effect of MMP-9-1562 polymorphism on PE in different countries including the Netherlands (26), United Kingdom (27), Brazil (28-31), Iran (32, 33), China (25), Poland (34), Egypt (14, 35), and Tunisia (24). Moreover, several meta-analyses have also been performed on this issue (36-39).
However, based on the last meta-analysis, a number of case-control studies have been added, therefore authors aimed to conduct an updated meta-analysis regarding the role MMP-9-1562 polymorphism on PE susceptibility to access a comprehensive result.
2. Materials and Methods
2.1. Eligibility criteria
The inclusion criteria were defined based on the population, intervention, comparison, outcome, and study design framework to ensure a systematic and transparent approach. The population included pregnant women diagnosed with PE, while the intervention focused on the presence of the MMP-9-1562 polymorphism. The comparison group consisted of pregnant women without PE serving as controls. The primary outcome was the association between the MMP-9-1562 polymorphism and the risk of PE, assessed through odds ratios (ORs) with 95% confidence intervals (CIs). Only case-control studies reporting genotype frequencies in both cases and controls were considered eligible for inclusion.
Studies were included if they provided sufficient data to calculate or extract an OR along with its 95% CI. Exclusion criteria comprised animal studies, meta-analyses, conference papers, letters to the editor, reviews, studies with incomplete genotype and allele data, and duplicate publications. 2 authors independently screened and extracted relevant data, including the first author’s name, publication year, country, and ethnicity of participants, polymerase chain reaction (PCR) method, number of cases and controls, and genotype distribution in both groups.
The methodological quality of each included case-control study was assessed using a modified version of the Newcastle-Ottawa Scale, specifically adapted for genetic association studies. This tool evaluates studies based on 3 broad domains: selection of study groups, comparability of groups, and ascertainment of exposure. Each study could be awarded a maximum of 9 stars across 8 criteria: adequate definition and representativeness of cases, selection and definition of controls, control for confounding variables (e.g., maternal age, body mass index), exposure assessment, consistency in genotyping methods between groups, and response rate.
Studies that received 6 or more stars were categorized as moderate-to-high quality, while those scoring below 6 stars were considered low quality. All studies included in the final meta-analysis achieved a quality score of 8 or higher, indicating acceptable to high methodological rigor.
2.2. Information sources
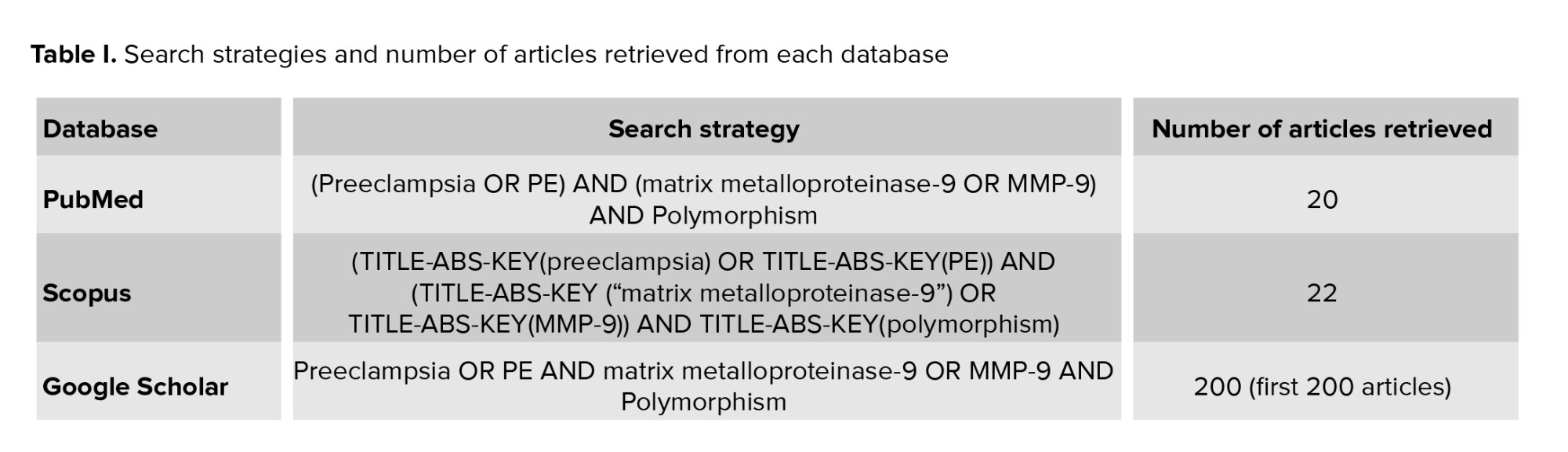
To perform the current meta-analysis study, databases such as Scopus, PubMed, and Google Scholar, with a focus on the correlation between MMP-9 and the risk of PE, were screened by 2 authors independently. The search keywords were ‘Preeclampsia OR PE’ and ‘matrix metalloproteinase-9 OR MMP-9’, and ‘Polymorphism’. As mentioned in table I, the number of articles retrieved in PubMed, Scopus, and Google Scholar were 20, 22, and 200 in each database, respectively. Authors also manually screened references cited in the retrieved studies to find additional eligible studies.
2.3. Statistical Analysis
The MetaGenyo web tool (40) was employed for data analysis. The deviation from Hardy-Weinberg equilibrium (HWE) in control individuals was determined by applying the Chi-square test. To measure the strength of association, the OR and CI were calculated under several genetic models: allelic, heterozygous, and homozygous codominant, dominant, overdominant, and recessive models. Heterogeneity among the included studies was assessed using the I² statistic, with values over 50% indicating substantial heterogeneity. However, given the clinical and methodological diversity across the included studies, such as differences in study populations, ethnicities, and settings, random-effects model was applied for all meta-analyses regardless of the level of heterogeneity. This approach accounts for both within-study and between-study variability and is considered more appropriate when pooling data from heterogeneous sources. Based on ethnicity, subgroup analysis was conducted. The Egger's test was employed to estimate publication bias. Finally, in order to assess the potential impact of each investigation on the overall outcome, a sensitive analysis by sequentially deleting each study was conducted.
To assess the overall certainty of evidence in this meta-analysis, we applied the grading of recommendations, assessment, development, and evaluation framework. This approach evaluates the quality of evidence based on factors such as risk of bias, inconsistency, indirectness, imprecision, and publication bias. The assessment was performed for each genetic model, considering study design limitations, heterogeneity across studies, and the robustness of pooled effect estimates.
3. Results
3.1. Characteristics of studies and meta-analysis results
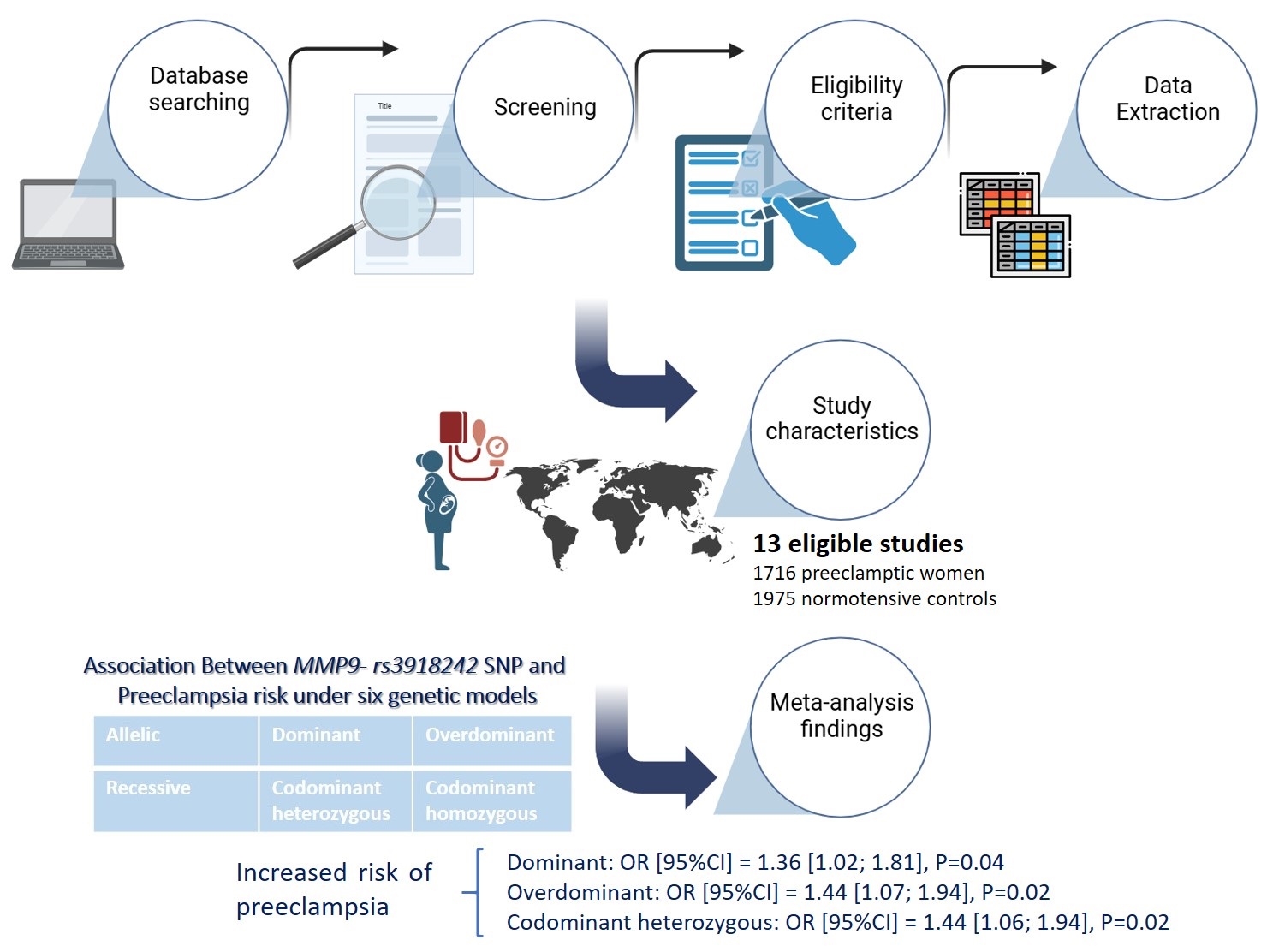
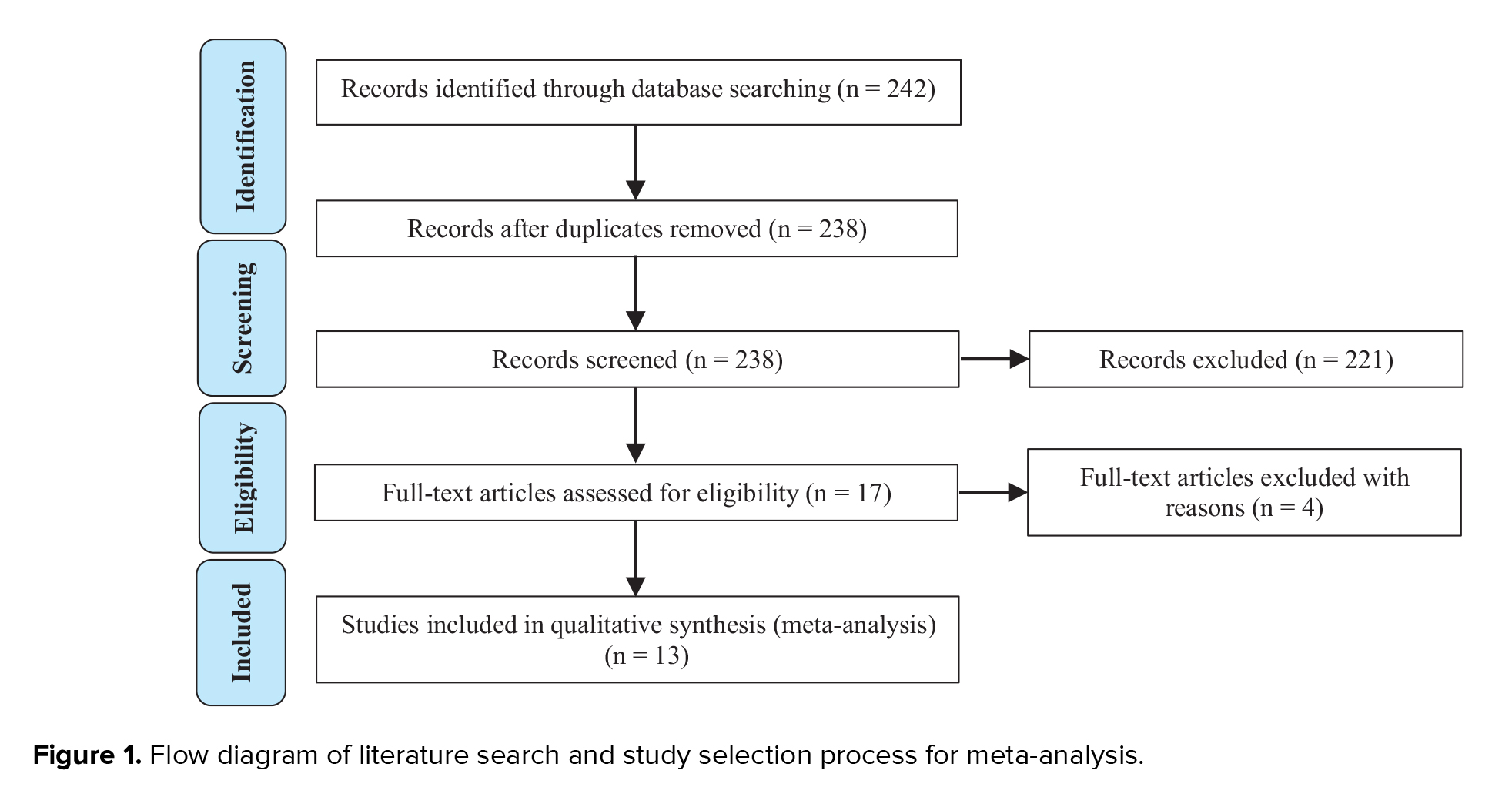
After conducting a literature search in PubMed, Scopus, and Google Scholar databases, we identified 13 eligible studies, containing 1716 preeclamptic women and 1975 normotensive controls (Figure 1). The detailed characteristics of selected studies are reported in table II.
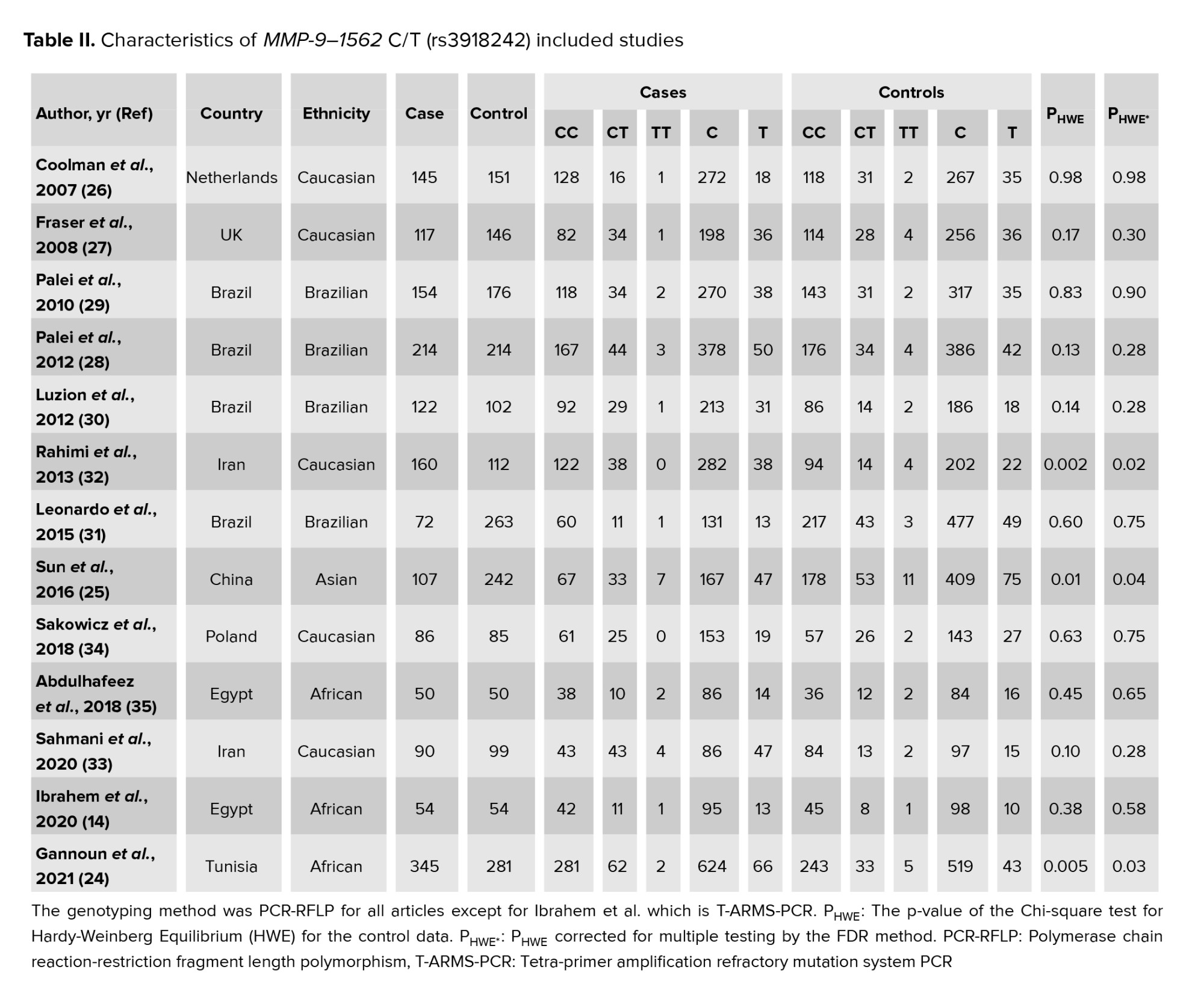
All 13 case-control studies included in this meta-analysis demonstrated moderate-to-high methodological quality, with total quality scores ranging from 8-9 out of a maximum of 9. Most studies clearly defined cases and controls, used representative samples, and applied reliable and consistent genotyping methods across groups. Additionally, several studies appropriately controlled important confounding factors such as maternal age, body mass index, or comorbidities. Based on these quality assessments, all studies were included in the meta-analysis, as they met acceptable methodological standards. The meta-analysis results are given in table III.
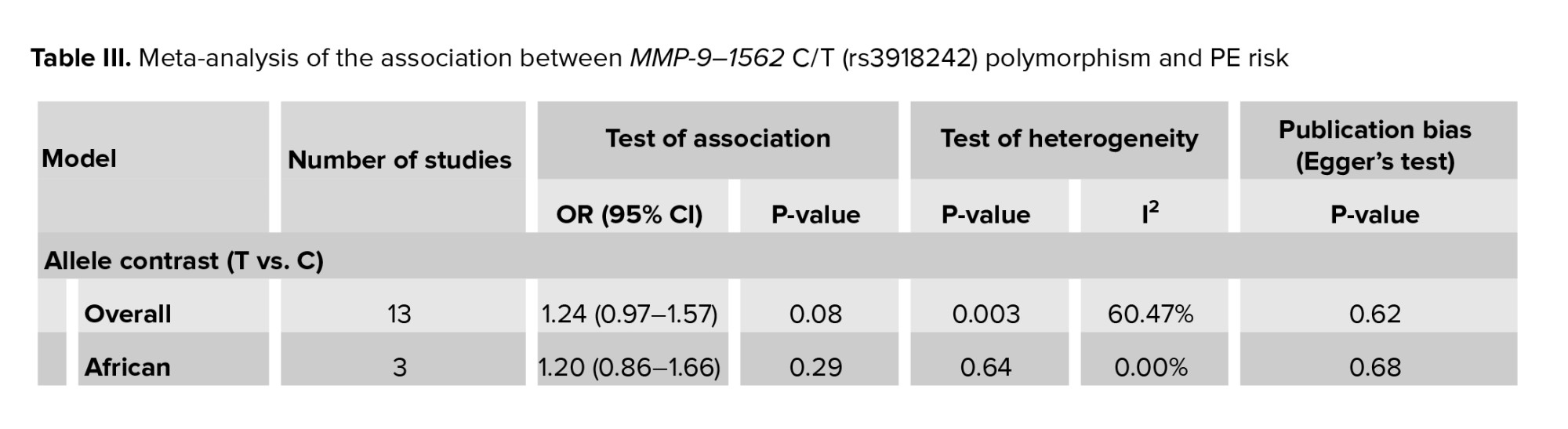
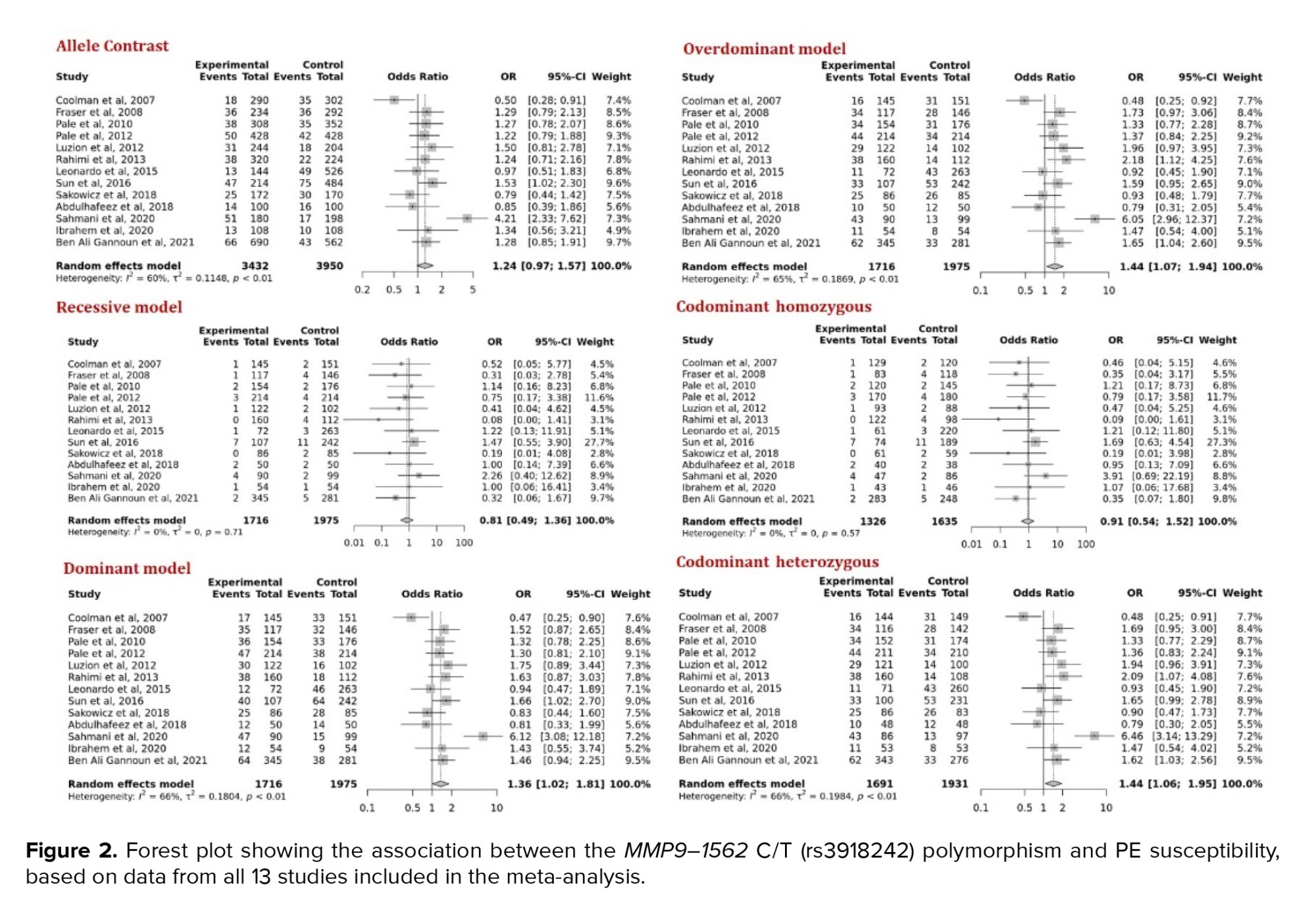
The test of association was conducted to evaluate the role of MMP-9- rs3918242 on susceptibility to PE in 13 studies under 6 genetic models, which depict that this variant was correlated with an increased risk of PE in dominant (OR [95% CI] = 1.36 [1.02; 1.81], p = 0.04), overdominant (OR [95% CI] = 1.44 [1.07; 1.94], p = 0.02), and codominant heterozygous (OR [95% CI] = 1.44 [1.06; 1.94], p = 0.02) models (Figure 2).
Using sensitivity analysis to demonstrate the potential influence of each data point on the pooled ORs, our data remained consistently significant in the overdominant and codominant heterozygous.
This analysis indicates that the final pooled ORs were highly stable and no individual study considerably affected the combined ORs. However, this analysis showed that the removal of the Coolman et al. (26) study resulted in a notable change in the pooled OR for both the allele contrast (OR [95% CI] = 1.33 [1.07; 1.65]) and dominant model (OR [95% CI] = 1.48 [1.15; 1.92]).
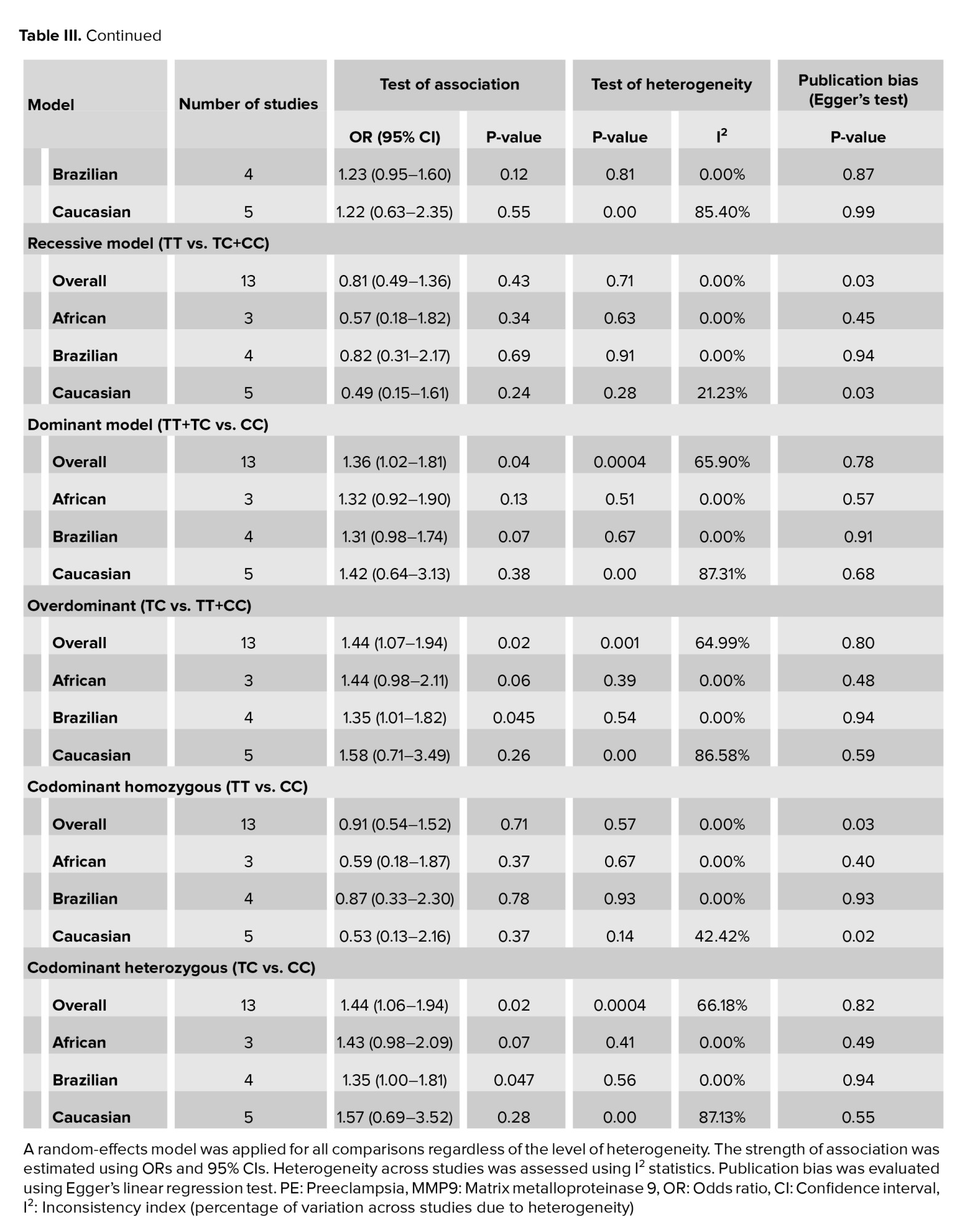
Moreover, the subgroup analysis was performed by ethnicity. The findings showed the link of rs3918242 with increased risk of PE in Brazilian women in overdominant (OR [95% CI] = 1.35 [1.01; 1.82], p = 0.045) and codominant heterozygous (OR [95% CI] = 1.35 [1.00; 1.81], p = 0.047) models. We did not find any association between MMP-9 rs3918242 and the risk of PE in Caucasians and Africans within the studied models.
In further analysis, we only included 10 studies that were in HWE. The forest plots are presented in figure 3.
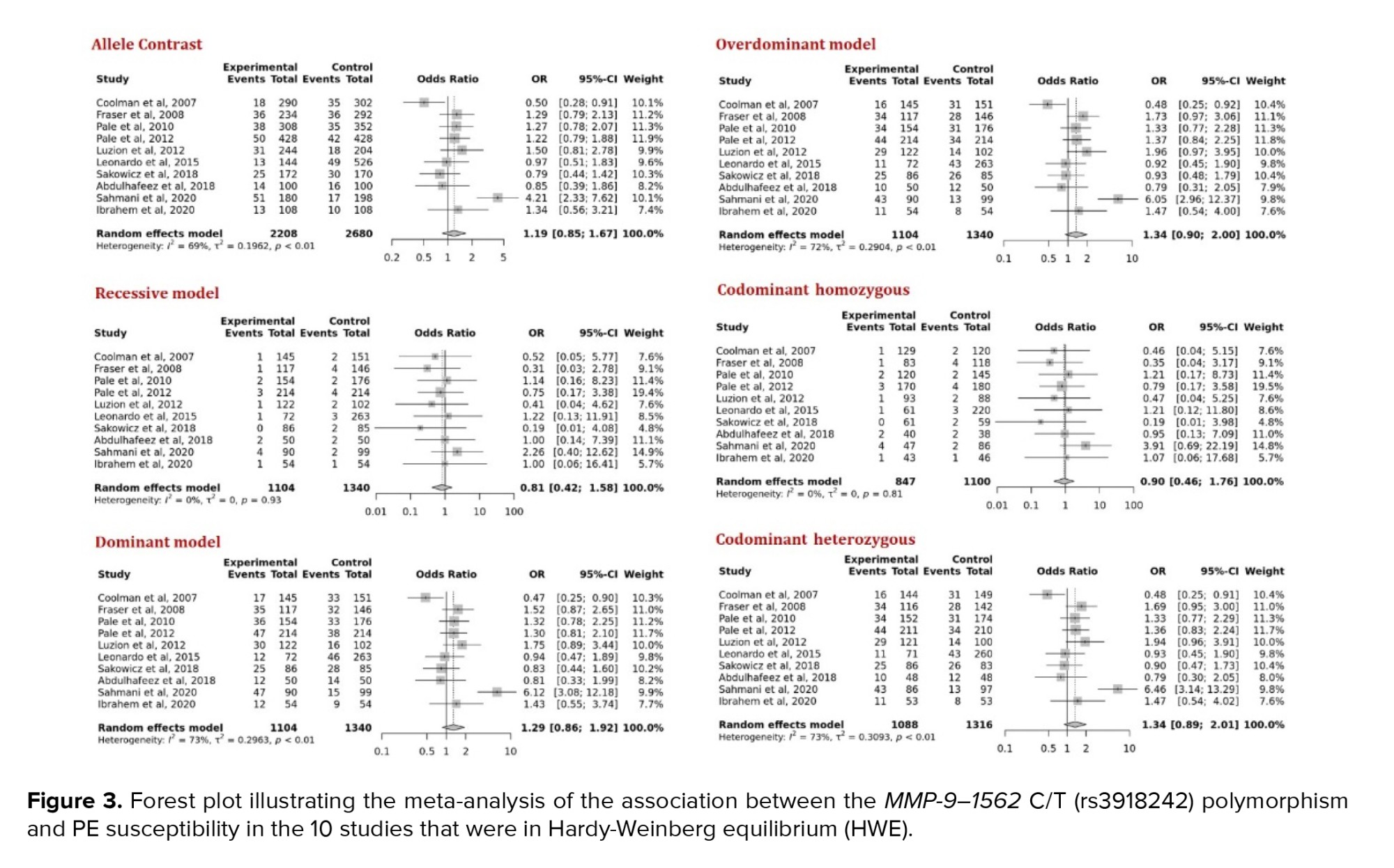
The results revealed no remarkable association between rs3918242 and PE risk under any genetic models (Table III).
Sensitivity analysis showed that by omitting Coolman et al. (26) study, the pooled OR can significantly affect the results in overdominant (OR [95% CI] = 1.51 [1.05; 2.18]) and codominant heterozygous (OR [95% CI] = 1.51 [1.03; 2.20]) models.
Stratified analysis by ethnicity did not exhibit a significant relationship between this SNP and PE in Caucasians and Africans, while the association was detected between rs3918242 genotypes and increased risk of PE in overdominant and codominant heterozygous models among Brazilians.
3.2. Heterogeneity and publication bias
As presented in table III, heterogeneity was observed between studies in allelic, dominant, overdominant, and codominant heterozygous genetic models. No heterogeneity was observed among African and Brazilian ethnicities after stratified analysis, while heterogeneity remained in Caucasians in 4 genetic models, as mentioned for the overall meta-analysis.
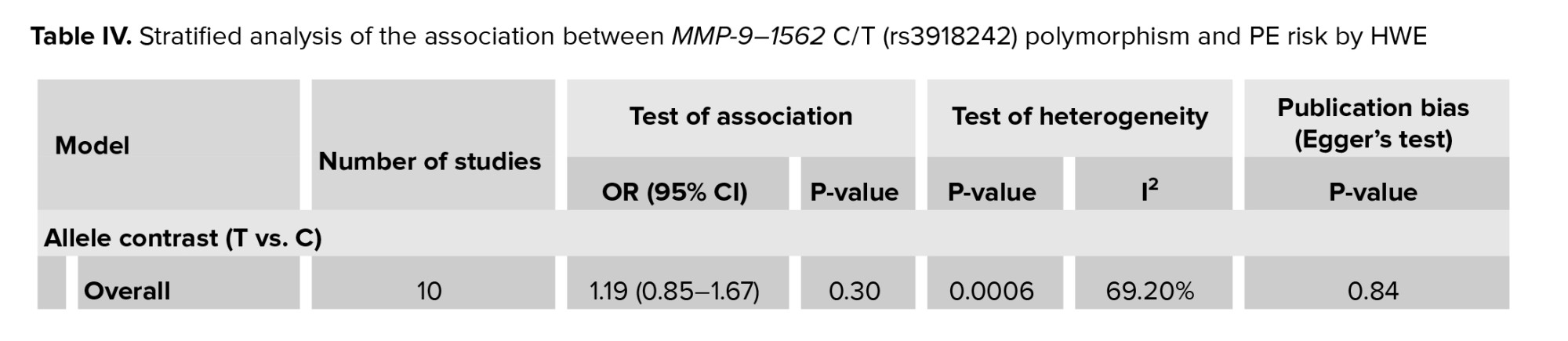
According to the data in table IV, the heterogeneity results did not change after excluding 3 studies with departure from HWE.
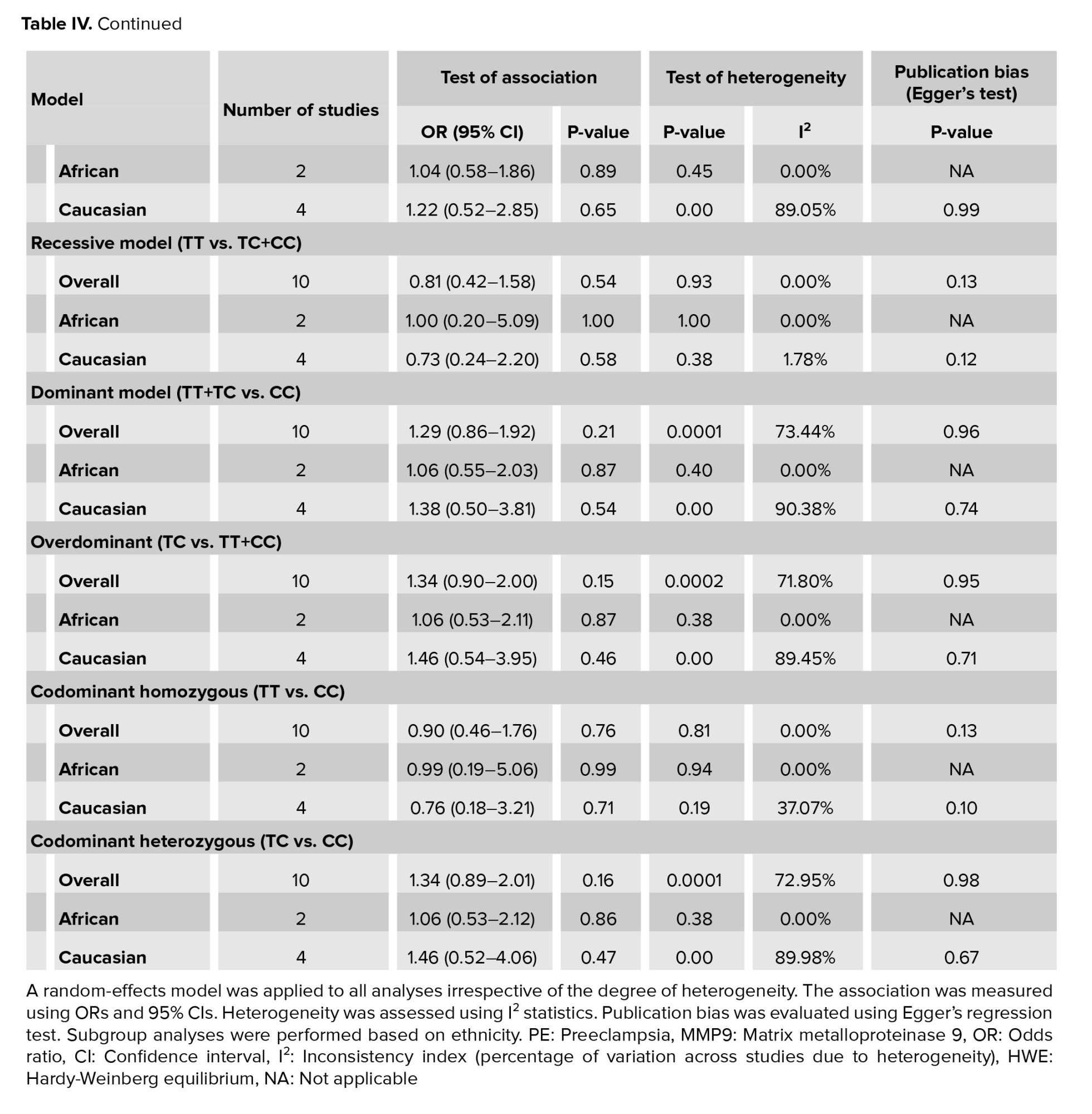
The significant publication bias for overall studies and Caucasian ethnicity in recessive and codominant homozygous was detected by Egger's test, while no publication bias was observed for African and Brazilian ethnicities in 6 comparison models (Table II). The publication bias was not demonstrated in overall and subgroup studies after excluding the studies with HWE disturbance (Table IV).
To further evaluate the strength of evidence supporting the association between MMP-9 rs3918242 polymorphism and PE risk, we conducted a grading of recommendations, development, and evaluation assessment. The overall certainty of evidence ranged from low to moderate, with moderate-quality evidence supporting associations in the dominant (OR = 1.36, 95% CI = [1.02; 1.81], p = 0.04), overdominant (OR = 1.44, 95% CI = [1.07; 1.94], p = 0.02), and codominant heterozygous (OR = 1.44, 95% CI = [1.06; 1.94], p = 0.02) models. However, substantial heterogeneity was detected in some comparisons (I² > 60%), particularly among Caucasian populations, which may impact the reliability of pooled estimates. No significant association was observed in recessive or codominant homozygous models, and potential publication bias was detected in recessive and codominant homozygous comparisons. These findings suggest a possible genetic effect of MMP-9 rs3918242 on PE susceptibility, particularly in specific genetic models and subpopulations.
4. Discussion
In the current meta-analysis study, once we included all 13 published studies and found an association between MMP-9-rs3918242 polymorphism and a multiplied risk of PE through the pooled-ORs of 13 studies, including 1716 preeclamptic women and 1975 normotensive controls. Our analysis within 6 comparison models covering allelic, dominant, overdominant, recessive, codominant heterozygous, and codominant homozygous genetic models demonstrated the effect of rs3918242 on increased risk of PE in dominant, overdominant, and codominant heterozygous. Although after subgroup analysis by ethnicity, this association was observed in the Brazilian ethnicity in both overdominant and codominant heterozygotes.
Evidence has shown that genetic variants might contribute to PE development (41-43). An accumulating number of studies have examined the association between MMP-9 gene variation and PE risk. However, the results were inconsistent. Therefore, the importance of meta-analysis studies is vivid in combining the results of multiple case-control studies to clarify the conclusion.
The first meta-analysis regarding the association between MMP-9 1562 C>T (rs3918242) polymorphism and PE risk was reported in 2014 (36). 5 studies (712 cases and 766 controls) in the meta-analysis were included, and no association was found between the rs3918242 variant and risk of PE (26-30). One study was excluded from the statistical analysis due to the deviation from the HWE (32). In the next similar meta-analysis study, the total of 6 publications involving 871 cases and 845 controls were included in the analysis, and the lack of association between the rs3918242 SNP and PE susceptibility was reported (37). The subgroup analysis by ethnicity, including 3 studies of Palei et al. (28, 29) as well as Luizon et al. (30), exhibited no significant link between rs3918242 polymorphism and PE among Brazilian women.
In 2018, a systematic review and meta-analysis were published of the MMPs gene variant in diseases that impact fertility and pregnancy-related complications (38). Their quantitative calculation for rs3918242 in PE involved only 4 studies (488 cases and 736 controls) (26, 27, 29, 31). 2 studies were excluded due to deviation from HWE (25, 32), and 2 studies because they were conducted by the same authors (28, 30). The results revealed that the correlation between rs3918242 and PE was not statistically significant under any genetic model.
Recently, a meta-analysis was conducted to assess the role of rs3918242 on susceptibility to hypertensive disorders of pregnancy, which include gestational hypertension, PE, eclampsia, superimposed PE, and chronic hypertension during pregnancy (39). The meta-analysis included 8 published reports, comprising 1300 HDP cases and 1612 normotensive subjects. The authors observed that rs3918242 raised the risk of HDP in dominant and allelic models. Moreover, subgroup analyses of 6 studies (25, 27, 28, 30-32), showed that rs3918242 escalated the risk of PE in both dominant and allelic models (OR [95% CI] = 1.48 [1.18-1.86], p = 0.001; 1.32 [1.08-1.62], p = 0.007; respectively). They excluded the Coolman et al. (26) study to reduce the heterogeneity.
Subsequently, we repeated the analysis after excluding 3 studies, which deviated from HWE (24, 25, 32). The pooled ORs of the remaining data displayed no correlation between MMP-9-rs3918242 and PE development. However, subgroup analysis showed an elevated risk of PE in Brazilian ethnicity in overdominant and codominant heterozygous models.
Deviations from HWE in case-control studies can be due to a variety of factors, including selection bias, mutation, population stratification, genotyping/sampling errors, biological factors, and non-random mating. These deviations need to be carefully accounted for and addressed in the analysis to ensure the validity of the study results. Therefore, in the current meta-analysis, we carried out the analysis both before and after excluding data from studies with deviations from HWE. Although this exclusion parameter indicated that departure from HWE did not affect the estimation of effect sizes and heterogeneity, it influenced the publication bias in the overall analysis. Moreover, we conducted sensitivity analyses to assess the robustness of the meta-analysis results, and we checked the potential impact of each included study on the overall findings. Based on the sensitivity analysis, we observed that none of the individual reports had a significant impact on the overall pooled ORs. Based on the sensitivity analysis, we observed that omitting the Coolman et al. (26) study had a significant impact on the overall pooled ORs.
Although this meta-analysis presents a comprehensive view regarding the association between MMP-9-rs3918242 and PE development, it has several limitations: within our research, heterogeneity was evident across various genetic models, possibly influenced by environmental factors, lifestyle choices, and the criteria used for participant selection, particularly within the control group. Due to the insufficient data on enrolled study subjects, we were unable to precisely evaluate the risk of PE following adjustments for variables such as age, lifestyle, family history, and environmental factors, among others, which could potentially impact the overall conclusions. Given the limited number of case-control studies included in our meta-analysis, the findings should be interpreted with precaution. In order to illuminate the exact connection between MMP-9-rs3918242 and the risk of PE, it is essential to control the confounding factors with a larger sample size.
5. Conclusion
This updated meta-analysis reveals a potential link between the MMP-9 -1562 C/T (rs3918242) polymorphism and an increased risk of PE, particularly under specific genetic models and in certain ethnic groups such as Brazilians. These findings contribute to a better understanding of the genetic underpinnings of PE, a complex and serious pregnancy complication with global health implications. By synthesizing data from diverse populations and highlighting areas of significant association, this study emphasizes the importance of considering genetic risk factors in the context of maternal health. While limitations such as heterogeneity and unmeasured confounders exist, the results support the need for future large-scale, ethnically diverse, and mechanistically focused studies to clarify these associations and explore their clinical relevance. Overall, this work adds to the growing body of knowledge that may ultimately guide more personalized approaches in predicting, preventing, and managing PE.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
F. Rakhshani Moghaddam: Revising the work critically for important intellectual content; M. Razavi: Analysis of data for the work and final approval of the version to be published.
Acknowledgments
This study was not financially supported. An artificial intelligence tool, OpenAI's ChatGPT (GPT-4), was used to assist in the grammar check of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Preeclampsia (PE) is a prevalent form of hypertension disorder of pregnancy (HDP) that happens after 20 wk of gestation. In clinical terms, augmented hypertension (systolic and diastolic blood pressure ≥ 140/90 mmHg) accompanied by proteinuria (≥ 300 mg within 24 hr) are diagnostic criteria for PE (1, 2). PE is blamed for the maternal and fetal mortality and morbidity, with the incidence ranging from 2-8% worldwide (3).
Several mechanisms have been implicated in the development of PE, including incomplete placental development and inadequate trophoblast invasion, oxidative stress, endothelial cell dysfunction, placental ischemia, and immune maladaptation (4, 5). Furthermore, genetic factors are supposed to have an important function in the etiology of PE (6-8). However, despite the numerous investigations regarding the etiology and pathogenesis of PE, the precise mechanisms are still undetermined (9).
Matrix metalloproteinase (MMPs) are known as extracellular proteinases and in such physiological and pathological mechanisms, including embryogenesis, implantation, formation of the placenta, tumor transformation, and neoangiogenesis, exert a significant function (10-13). Many cell types, such as immune cells, structural connective tissue cells, epithelial barrier cells, and phagocytic cells, are responsible for the secretion of MMPs (10). In PE cases, trophoblastic invasion might be influenced by altered MMP levels, which may further contribute to endothelial dysfunction through engaging with augmented oxidative stress and inflammatory mediators (14, 15).
MMP-9, also known as gelatinase B, is an important type of MMP family, which is mainly produced by monocytes, neutrophils, and vascular endothelial cells (16). Based on previous studies, in the serum of PE women, MMP-9 levels were increased (17, 18), and this finding was also observed in the umbilical cord plasma of newborns in mothers affected with PE (19). Several polymorphisms have been recognized in the MMP-9 gene, in which the MMP-9-1562 C>T (rs3918242) polymorphism is well studied in different disorders (20-23). This single-nucleotide polymorphism (SNP) is situated in the promoter region of the MMP-9 gene and is correlated with higher protein levels and higher transcriptional activity of MMP-9 (24). The MMP-9 genetic variations may lead to modifications in both protein structure and expression level (25).
Several studies investigated the effect of MMP-9-1562 polymorphism on PE in different countries including the Netherlands (26), United Kingdom (27), Brazil (28-31), Iran (32, 33), China (25), Poland (34), Egypt (14, 35), and Tunisia (24). Moreover, several meta-analyses have also been performed on this issue (36-39).
However, based on the last meta-analysis, a number of case-control studies have been added, therefore authors aimed to conduct an updated meta-analysis regarding the role MMP-9-1562 polymorphism on PE susceptibility to access a comprehensive result.
2. Materials and Methods
2.1. Eligibility criteria
The inclusion criteria were defined based on the population, intervention, comparison, outcome, and study design framework to ensure a systematic and transparent approach. The population included pregnant women diagnosed with PE, while the intervention focused on the presence of the MMP-9-1562 polymorphism. The comparison group consisted of pregnant women without PE serving as controls. The primary outcome was the association between the MMP-9-1562 polymorphism and the risk of PE, assessed through odds ratios (ORs) with 95% confidence intervals (CIs). Only case-control studies reporting genotype frequencies in both cases and controls were considered eligible for inclusion.
Studies were included if they provided sufficient data to calculate or extract an OR along with its 95% CI. Exclusion criteria comprised animal studies, meta-analyses, conference papers, letters to the editor, reviews, studies with incomplete genotype and allele data, and duplicate publications. 2 authors independently screened and extracted relevant data, including the first author’s name, publication year, country, and ethnicity of participants, polymerase chain reaction (PCR) method, number of cases and controls, and genotype distribution in both groups.
The methodological quality of each included case-control study was assessed using a modified version of the Newcastle-Ottawa Scale, specifically adapted for genetic association studies. This tool evaluates studies based on 3 broad domains: selection of study groups, comparability of groups, and ascertainment of exposure. Each study could be awarded a maximum of 9 stars across 8 criteria: adequate definition and representativeness of cases, selection and definition of controls, control for confounding variables (e.g., maternal age, body mass index), exposure assessment, consistency in genotyping methods between groups, and response rate.
Studies that received 6 or more stars were categorized as moderate-to-high quality, while those scoring below 6 stars were considered low quality. All studies included in the final meta-analysis achieved a quality score of 8 or higher, indicating acceptable to high methodological rigor.
2.2. Information sources
To perform the current meta-analysis study, databases such as Scopus, PubMed, and Google Scholar, with a focus on the correlation between MMP-9 and the risk of PE, were screened by 2 authors independently. The search keywords were ‘Preeclampsia OR PE’ and ‘matrix metalloproteinase-9 OR MMP-9’, and ‘Polymorphism’. As mentioned in table I, the number of articles retrieved in PubMed, Scopus, and Google Scholar were 20, 22, and 200 in each database, respectively. Authors also manually screened references cited in the retrieved studies to find additional eligible studies.
2.3. Statistical Analysis
The MetaGenyo web tool (40) was employed for data analysis. The deviation from Hardy-Weinberg equilibrium (HWE) in control individuals was determined by applying the Chi-square test. To measure the strength of association, the OR and CI were calculated under several genetic models: allelic, heterozygous, and homozygous codominant, dominant, overdominant, and recessive models. Heterogeneity among the included studies was assessed using the I² statistic, with values over 50% indicating substantial heterogeneity. However, given the clinical and methodological diversity across the included studies, such as differences in study populations, ethnicities, and settings, random-effects model was applied for all meta-analyses regardless of the level of heterogeneity. This approach accounts for both within-study and between-study variability and is considered more appropriate when pooling data from heterogeneous sources. Based on ethnicity, subgroup analysis was conducted. The Egger's test was employed to estimate publication bias. Finally, in order to assess the potential impact of each investigation on the overall outcome, a sensitive analysis by sequentially deleting each study was conducted.
To assess the overall certainty of evidence in this meta-analysis, we applied the grading of recommendations, assessment, development, and evaluation framework. This approach evaluates the quality of evidence based on factors such as risk of bias, inconsistency, indirectness, imprecision, and publication bias. The assessment was performed for each genetic model, considering study design limitations, heterogeneity across studies, and the robustness of pooled effect estimates.
3. Results
3.1. Characteristics of studies and meta-analysis results
After conducting a literature search in PubMed, Scopus, and Google Scholar databases, we identified 13 eligible studies, containing 1716 preeclamptic women and 1975 normotensive controls (Figure 1). The detailed characteristics of selected studies are reported in table II.
All 13 case-control studies included in this meta-analysis demonstrated moderate-to-high methodological quality, with total quality scores ranging from 8-9 out of a maximum of 9. Most studies clearly defined cases and controls, used representative samples, and applied reliable and consistent genotyping methods across groups. Additionally, several studies appropriately controlled important confounding factors such as maternal age, body mass index, or comorbidities. Based on these quality assessments, all studies were included in the meta-analysis, as they met acceptable methodological standards. The meta-analysis results are given in table III.
The test of association was conducted to evaluate the role of MMP-9- rs3918242 on susceptibility to PE in 13 studies under 6 genetic models, which depict that this variant was correlated with an increased risk of PE in dominant (OR [95% CI] = 1.36 [1.02; 1.81], p = 0.04), overdominant (OR [95% CI] = 1.44 [1.07; 1.94], p = 0.02), and codominant heterozygous (OR [95% CI] = 1.44 [1.06; 1.94], p = 0.02) models (Figure 2).
Using sensitivity analysis to demonstrate the potential influence of each data point on the pooled ORs, our data remained consistently significant in the overdominant and codominant heterozygous.
This analysis indicates that the final pooled ORs were highly stable and no individual study considerably affected the combined ORs. However, this analysis showed that the removal of the Coolman et al. (26) study resulted in a notable change in the pooled OR for both the allele contrast (OR [95% CI] = 1.33 [1.07; 1.65]) and dominant model (OR [95% CI] = 1.48 [1.15; 1.92]).
Moreover, the subgroup analysis was performed by ethnicity. The findings showed the link of rs3918242 with increased risk of PE in Brazilian women in overdominant (OR [95% CI] = 1.35 [1.01; 1.82], p = 0.045) and codominant heterozygous (OR [95% CI] = 1.35 [1.00; 1.81], p = 0.047) models. We did not find any association between MMP-9 rs3918242 and the risk of PE in Caucasians and Africans within the studied models.
In further analysis, we only included 10 studies that were in HWE. The forest plots are presented in figure 3.
The results revealed no remarkable association between rs3918242 and PE risk under any genetic models (Table III).
Sensitivity analysis showed that by omitting Coolman et al. (26) study, the pooled OR can significantly affect the results in overdominant (OR [95% CI] = 1.51 [1.05; 2.18]) and codominant heterozygous (OR [95% CI] = 1.51 [1.03; 2.20]) models.
Stratified analysis by ethnicity did not exhibit a significant relationship between this SNP and PE in Caucasians and Africans, while the association was detected between rs3918242 genotypes and increased risk of PE in overdominant and codominant heterozygous models among Brazilians.
3.2. Heterogeneity and publication bias
As presented in table III, heterogeneity was observed between studies in allelic, dominant, overdominant, and codominant heterozygous genetic models. No heterogeneity was observed among African and Brazilian ethnicities after stratified analysis, while heterogeneity remained in Caucasians in 4 genetic models, as mentioned for the overall meta-analysis.
According to the data in table IV, the heterogeneity results did not change after excluding 3 studies with departure from HWE.
The significant publication bias for overall studies and Caucasian ethnicity in recessive and codominant homozygous was detected by Egger's test, while no publication bias was observed for African and Brazilian ethnicities in 6 comparison models (Table II). The publication bias was not demonstrated in overall and subgroup studies after excluding the studies with HWE disturbance (Table IV).
To further evaluate the strength of evidence supporting the association between MMP-9 rs3918242 polymorphism and PE risk, we conducted a grading of recommendations, development, and evaluation assessment. The overall certainty of evidence ranged from low to moderate, with moderate-quality evidence supporting associations in the dominant (OR = 1.36, 95% CI = [1.02; 1.81], p = 0.04), overdominant (OR = 1.44, 95% CI = [1.07; 1.94], p = 0.02), and codominant heterozygous (OR = 1.44, 95% CI = [1.06; 1.94], p = 0.02) models. However, substantial heterogeneity was detected in some comparisons (I² > 60%), particularly among Caucasian populations, which may impact the reliability of pooled estimates. No significant association was observed in recessive or codominant homozygous models, and potential publication bias was detected in recessive and codominant homozygous comparisons. These findings suggest a possible genetic effect of MMP-9 rs3918242 on PE susceptibility, particularly in specific genetic models and subpopulations.
4. Discussion
In the current meta-analysis study, once we included all 13 published studies and found an association between MMP-9-rs3918242 polymorphism and a multiplied risk of PE through the pooled-ORs of 13 studies, including 1716 preeclamptic women and 1975 normotensive controls. Our analysis within 6 comparison models covering allelic, dominant, overdominant, recessive, codominant heterozygous, and codominant homozygous genetic models demonstrated the effect of rs3918242 on increased risk of PE in dominant, overdominant, and codominant heterozygous. Although after subgroup analysis by ethnicity, this association was observed in the Brazilian ethnicity in both overdominant and codominant heterozygotes.
Evidence has shown that genetic variants might contribute to PE development (41-43). An accumulating number of studies have examined the association between MMP-9 gene variation and PE risk. However, the results were inconsistent. Therefore, the importance of meta-analysis studies is vivid in combining the results of multiple case-control studies to clarify the conclusion.
The first meta-analysis regarding the association between MMP-9 1562 C>T (rs3918242) polymorphism and PE risk was reported in 2014 (36). 5 studies (712 cases and 766 controls) in the meta-analysis were included, and no association was found between the rs3918242 variant and risk of PE (26-30). One study was excluded from the statistical analysis due to the deviation from the HWE (32). In the next similar meta-analysis study, the total of 6 publications involving 871 cases and 845 controls were included in the analysis, and the lack of association between the rs3918242 SNP and PE susceptibility was reported (37). The subgroup analysis by ethnicity, including 3 studies of Palei et al. (28, 29) as well as Luizon et al. (30), exhibited no significant link between rs3918242 polymorphism and PE among Brazilian women.
In 2018, a systematic review and meta-analysis were published of the MMPs gene variant in diseases that impact fertility and pregnancy-related complications (38). Their quantitative calculation for rs3918242 in PE involved only 4 studies (488 cases and 736 controls) (26, 27, 29, 31). 2 studies were excluded due to deviation from HWE (25, 32), and 2 studies because they were conducted by the same authors (28, 30). The results revealed that the correlation between rs3918242 and PE was not statistically significant under any genetic model.
Recently, a meta-analysis was conducted to assess the role of rs3918242 on susceptibility to hypertensive disorders of pregnancy, which include gestational hypertension, PE, eclampsia, superimposed PE, and chronic hypertension during pregnancy (39). The meta-analysis included 8 published reports, comprising 1300 HDP cases and 1612 normotensive subjects. The authors observed that rs3918242 raised the risk of HDP in dominant and allelic models. Moreover, subgroup analyses of 6 studies (25, 27, 28, 30-32), showed that rs3918242 escalated the risk of PE in both dominant and allelic models (OR [95% CI] = 1.48 [1.18-1.86], p = 0.001; 1.32 [1.08-1.62], p = 0.007; respectively). They excluded the Coolman et al. (26) study to reduce the heterogeneity.
Subsequently, we repeated the analysis after excluding 3 studies, which deviated from HWE (24, 25, 32). The pooled ORs of the remaining data displayed no correlation between MMP-9-rs3918242 and PE development. However, subgroup analysis showed an elevated risk of PE in Brazilian ethnicity in overdominant and codominant heterozygous models.
Deviations from HWE in case-control studies can be due to a variety of factors, including selection bias, mutation, population stratification, genotyping/sampling errors, biological factors, and non-random mating. These deviations need to be carefully accounted for and addressed in the analysis to ensure the validity of the study results. Therefore, in the current meta-analysis, we carried out the analysis both before and after excluding data from studies with deviations from HWE. Although this exclusion parameter indicated that departure from HWE did not affect the estimation of effect sizes and heterogeneity, it influenced the publication bias in the overall analysis. Moreover, we conducted sensitivity analyses to assess the robustness of the meta-analysis results, and we checked the potential impact of each included study on the overall findings. Based on the sensitivity analysis, we observed that none of the individual reports had a significant impact on the overall pooled ORs. Based on the sensitivity analysis, we observed that omitting the Coolman et al. (26) study had a significant impact on the overall pooled ORs.
Although this meta-analysis presents a comprehensive view regarding the association between MMP-9-rs3918242 and PE development, it has several limitations: within our research, heterogeneity was evident across various genetic models, possibly influenced by environmental factors, lifestyle choices, and the criteria used for participant selection, particularly within the control group. Due to the insufficient data on enrolled study subjects, we were unable to precisely evaluate the risk of PE following adjustments for variables such as age, lifestyle, family history, and environmental factors, among others, which could potentially impact the overall conclusions. Given the limited number of case-control studies included in our meta-analysis, the findings should be interpreted with precaution. In order to illuminate the exact connection between MMP-9-rs3918242 and the risk of PE, it is essential to control the confounding factors with a larger sample size.
5. Conclusion
This updated meta-analysis reveals a potential link between the MMP-9 -1562 C/T (rs3918242) polymorphism and an increased risk of PE, particularly under specific genetic models and in certain ethnic groups such as Brazilians. These findings contribute to a better understanding of the genetic underpinnings of PE, a complex and serious pregnancy complication with global health implications. By synthesizing data from diverse populations and highlighting areas of significant association, this study emphasizes the importance of considering genetic risk factors in the context of maternal health. While limitations such as heterogeneity and unmeasured confounders exist, the results support the need for future large-scale, ethnically diverse, and mechanistically focused studies to clarify these associations and explore their clinical relevance. Overall, this work adds to the growing body of knowledge that may ultimately guide more personalized approaches in predicting, preventing, and managing PE.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Author Contributions
F. Rakhshani Moghaddam: Revising the work critically for important intellectual content; M. Razavi: Analysis of data for the work and final approval of the version to be published.
Acknowledgments
This study was not financially supported. An artificial intelligence tool, OpenAI's ChatGPT (GPT-4), was used to assist in the grammar check of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Review Article |
Subject:
Reproductive Genetics
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
