
International Journal of
Reproductive Biomedicine
Fri, Jun 12, 2026
[Archive]
Volume 23, Issue 7 (July 2025)
IJRM 2025, 23(7): 577-586 |
Back to browse issues page


Ethics code: IR.MUMS.NURSE.REC.1403.015
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abdollahi Senu N, Salari R, Ghavami V, Mirzakhani K. The effect of inhalation aromatherapy with lemon balm essential oil on perceived stress in infertile women undergoing in vitro fertilization: An RCT. IJRM 2025; 23 (7) :577-586
URL: http://ijrm.ir/article-1-3537-en.html
URL: http://ijrm.ir/article-1-3537-en.html



1- Student Research Committee, Mashhad University of Medical Sciences, Mashhad, Iran.
2- Department of Pharmaceutical Sciences in Persian Medicine, School of Persian and Complementary Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Midwifery, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran. ,Mirzakhanikb@gmail.com
2- Department of Pharmaceutical Sciences in Persian Medicine, School of Persian and Complementary Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3- Social Determinants of Health Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Biostatistics, School of Health, Mashhad University of Medical Sciences, Mashhad, Iran.
4- Nursing and Midwifery Care Research Center, Mashhad University of Medical Sciences, Mashhad, Iran. & Department of Midwifery, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran. ,
Full-Text [PDF 449 kb]
(817 Downloads)
| Abstract (HTML) (925 Views)
Full-Text: (130 Views)
- Introduction
Infertility is a biological, psychological, and social disorder that has a significant impact on various aspects of couples' lives (1). According to the report of the World Health Organization, almost 17.5% of the adult population experience infertility (2). According to the latest studies conducted at the national conference on infertility prevalence in Iran, the overall prevalence in Iranian couples was found to be 20.3% (3). Infertility is associated with physical, economic, psychological, and social stresses that affect a person's life. In Iran, the overall prevalence of psychological disorders in infertile couples is between 25 and 60% (4).
In recent years, in vitro fertilization (IVF) has been developed in the treatment of infertility (5). IVF treatment is a painful and stressful process (6).
Stress is defined as both an external adverse condition and a disruption of normal functioning, shaped by event perception and coping self-assessment. Chronic stress involves persistent threats to social roles and leads to mental and physical health issues, reduced productivity, lower quality of life, and higher medical costs (7, 8). In a study by Woods and colleagues, they highlight infertility-related stress as including identity crisis, social isolation, stigma, sexual and financial pressures, which may cause treatment dropout, marital stress, anxiety, depression, and decreased quality of life (9).
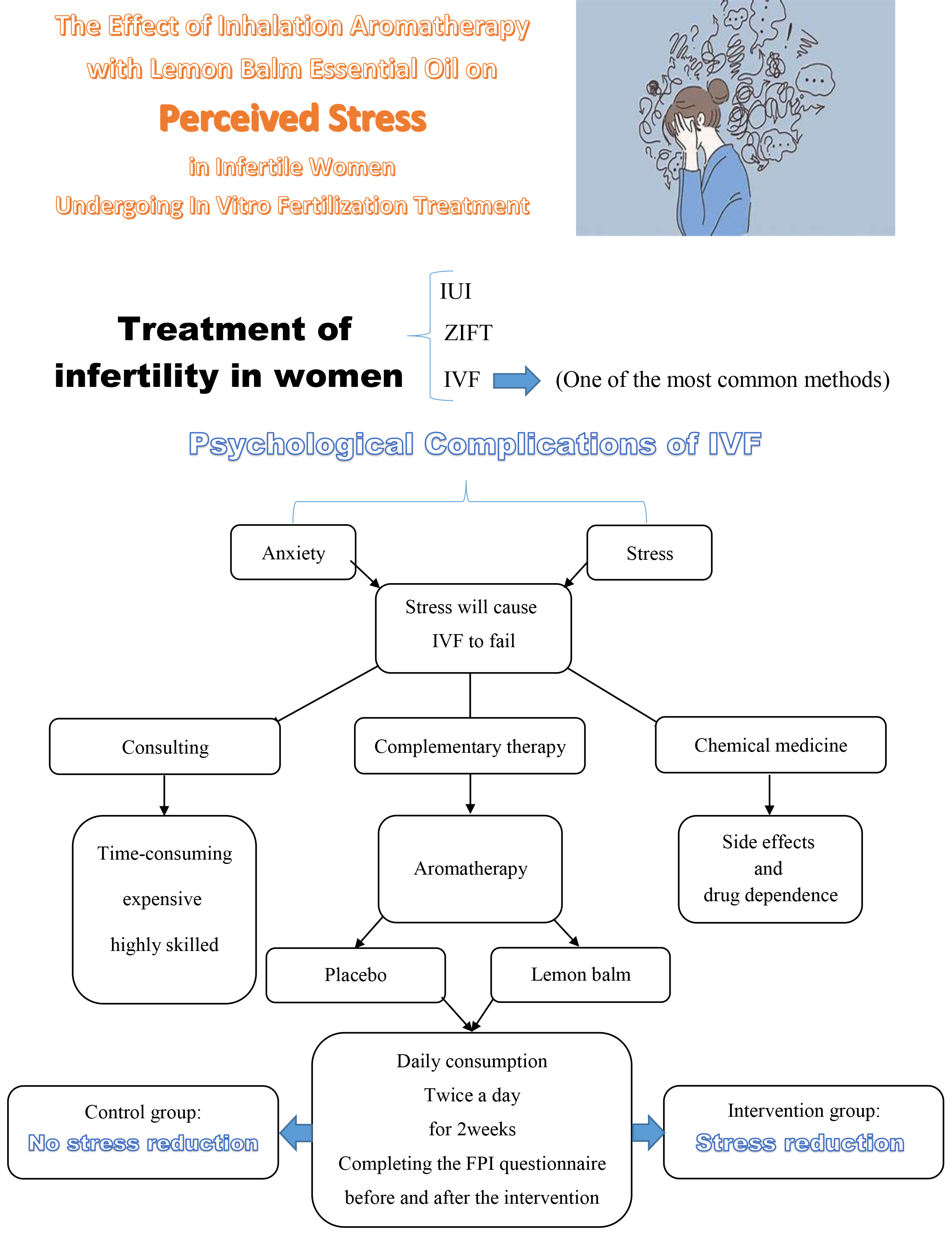
Stress is highly prevalent among infertile women, especially those undergoing assisted reproductive treatments like IVF (10). Alongside medical care, addressing psychological aspects is crucial, as stress management can improve treatment response and IVF success (11, 12). Non-pharmacological approaches, particularly complementary medicine, are preferred due to their affordability, ease, non-invasiveness, and minimal side effects (13). The use of complementary and herbal therapies is increasingly accepted in healthcare, focusing on reducing negative emotions (14). Aromatherapy, a rapidly growing complementary therapy using plant-derived essential oils, is applied for physical, mental, and spiritual well-being (15, 16).
In complementary medicine, one of the plants used is lemon balm (17), so the Food and Drug Administration has approved its safety and has shown that this plant does not have a mutagenic effect (18). Its antistress effects have been attributed to inhibition of cholinesterase enzyme activity and stimulation of acetylcholine and gamma-aminobutyric acid receptors (19-21).
This plant has been traditionally used to treat disorders such as anxiety and depression, and it also has antioxidant, anti-inflammatory, anti-spasmodic, antimicrobial, neuroprotective, and analgesic effects (17). In capsule form, it has been proposed as a sedative in the treatment of disorders such as stress, anxiety, and depression in individuals undergoing coronary artery bypass surgery, as well as type 2 diabetic individuals (22, 23). However, its effect on infertile women undergoing IVF has not been studied.
The present study aimed to determine the effect of inhaled aromatherapy with lemon balm essential oil on perceived stress in infertile women undergoing IVF treatment.
2. Materials and Methods
In recent years, in vitro fertilization (IVF) has been developed in the treatment of infertility (5). IVF treatment is a painful and stressful process (6).
Stress is defined as both an external adverse condition and a disruption of normal functioning, shaped by event perception and coping self-assessment. Chronic stress involves persistent threats to social roles and leads to mental and physical health issues, reduced productivity, lower quality of life, and higher medical costs (7, 8). In a study by Woods and colleagues, they highlight infertility-related stress as including identity crisis, social isolation, stigma, sexual and financial pressures, which may cause treatment dropout, marital stress, anxiety, depression, and decreased quality of life (9).
Stress is highly prevalent among infertile women, especially those undergoing assisted reproductive treatments like IVF (10). Alongside medical care, addressing psychological aspects is crucial, as stress management can improve treatment response and IVF success (11, 12). Non-pharmacological approaches, particularly complementary medicine, are preferred due to their affordability, ease, non-invasiveness, and minimal side effects (13). The use of complementary and herbal therapies is increasingly accepted in healthcare, focusing on reducing negative emotions (14). Aromatherapy, a rapidly growing complementary therapy using plant-derived essential oils, is applied for physical, mental, and spiritual well-being (15, 16).
In complementary medicine, one of the plants used is lemon balm (17), so the Food and Drug Administration has approved its safety and has shown that this plant does not have a mutagenic effect (18). Its antistress effects have been attributed to inhibition of cholinesterase enzyme activity and stimulation of acetylcholine and gamma-aminobutyric acid receptors (19-21).
This plant has been traditionally used to treat disorders such as anxiety and depression, and it also has antioxidant, anti-inflammatory, anti-spasmodic, antimicrobial, neuroprotective, and analgesic effects (17). In capsule form, it has been proposed as a sedative in the treatment of disorders such as stress, anxiety, and depression in individuals undergoing coronary artery bypass surgery, as well as type 2 diabetic individuals (22, 23). However, its effect on infertile women undergoing IVF has not been studied.
The present study aimed to determine the effect of inhaled aromatherapy with lemon balm essential oil on perceived stress in infertile women undergoing IVF treatment.
2. Materials and Methods
2.1. Sample collection
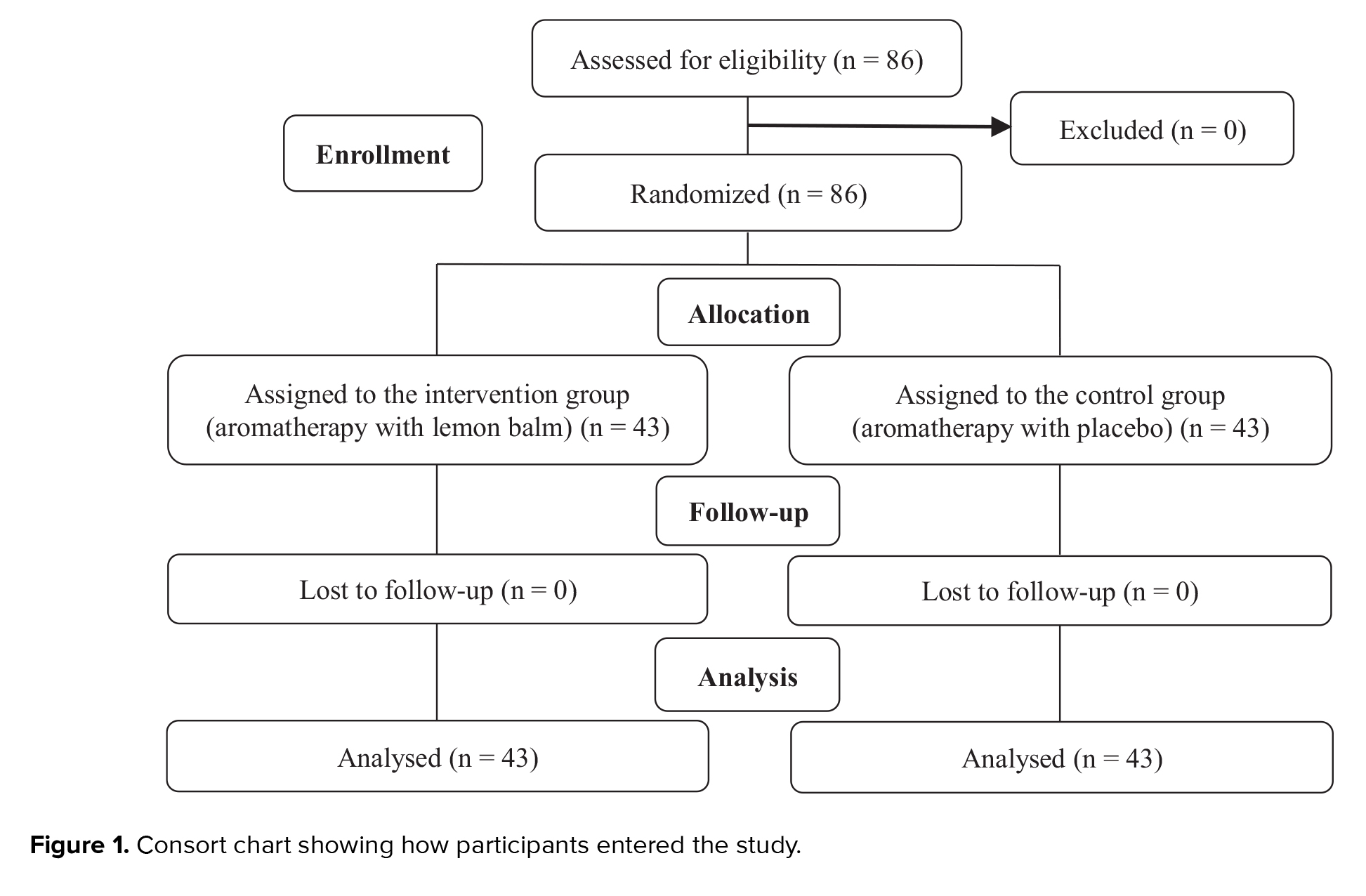
The present study was designed as a randomized clinical trial with a pretest-posttest method with an intervention and control group, which is taken from a study that will be published later, on 86 infertile women undergoing IVF treatment referring to the Milad Infertility Center, Imam Reza hospital in Mashhad, Iran. Sampling lasted from July-October 2024.
2.2. Sample size
The present study was designed as a randomized clinical trial with a pretest-posttest method with an intervention and control group, which is taken from a study that will be published later, on 86 infertile women undergoing IVF treatment referring to the Milad Infertility Center, Imam Reza hospital in Mashhad, Iran. Sampling lasted from July-October 2024.
2.2. Sample size
The sample size was calculated using the following formula at a significance level of 0.05, a power of 80%, the number of times the response variables were measured before and after the intervention, and a correlation of 0.5 (Figure 1). Finally, the final sample size was calculated as 43 people in each group.
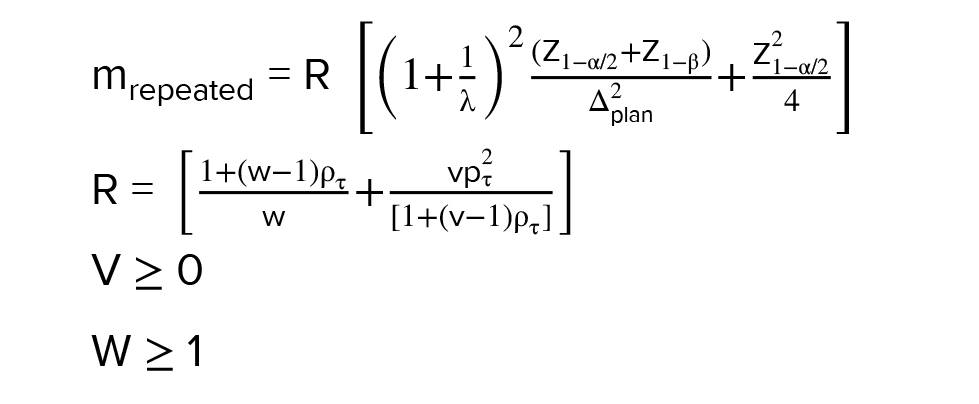
λ: Ratio of sample size in group 2 to group one
v: Number of measurements before intervention
w: Number of measurements after intervention
PT: Correlation coefficient between repeated measurements
Δplan: Standardized expected effect size
2.3. Sample collections and research groups
λ: Ratio of sample size in group 2 to group one
v: Number of measurements before intervention
w: Number of measurements after intervention
PT: Correlation coefficient between repeated measurements
Δplan: Standardized expected effect size
2.3. Sample collections and research groups
Inclusion criteria included having a history of infertility, being treated by IVF, no history of psychological problems (no history of hospitalization in a mental hospital and no use of psychiatric medications), no smell problems (based on the self-declaration of the research unit), not using sedatives, narcotics, or benzodiazepines, no physical illness, no experience of any unfortunate events in the past 6 months, and using a type of ovulation stimulation therapy with gonadotropins. Exclusion criteria included unwillingness to continue cooperation in research, allergy to lemon balm, failure to perform inhalation aromatherapy for 2 consecutive days (4 sessions), refusal to continue infertility treatment, unfortunate events (death of loved ones, accidents, natural disasters, bankruptcy during intervention), and change in health status that requires other treatments.
2.4. Randomization
2.4. Randomization
To assign individuals to intervention and control groups, a permutation block method with blocks of size 4 was used. For this purpose, the site www.sealedenvelope.com was used. The site listed 22 blocks randomly. This method continued until all individuals were assigned to 2 groups.
2.5. Intervention and blinding
2.5. Intervention and blinding
For the intervention, lemon balm essential oil was first prepared. Thus, the lemon balm plant was purchased from trusted centers of the Faculty of Iranian and Complementary Medicine. The plant was confirmed by a botanist at the Ferdowsi University of Mashhad Medicinal Plants Research Institute and its barium code was announced. The plant was soaked in a sweet almond oil base for 4-5 days using the traditional method, then strained. To ensure that the oil was saturated with essential oil, the fresh plant was soaked in the resulting oil for a second time for 4-5 days. Finally, it was filtered and standardized by gas chromatography. The placebo was just odorless sweet almond oil, which was readily available in the market. The research participants were asked to apply the final product, 5-7 drops, twice a day (morning and night) for 2 wk on the face at the beginning of the IVF hormone therapy cycle. To leave the mask on the face for 20-30 min each time while resting and in a calm state, and to inhale it. In the control group, subjects were also given a placebo. The placebo was odorless sweet almond oil (Kian Gostar Toseeh Parsian Co., Iran). The drug and placebo were coded confidentially by the pharmacist. The codes were kept confidential until the end of the study and the time of data analysis. The color and shape of the drug and placebo packages were completely similar, and their contents were unknown to the researcher and the research participants.
2.6. Outcome measures
2.6. Outcome measures
The outcome of this study was perceived stress in infertile women undergoing IVF treatment. Individuals were selected based on the research participant's checklist. To assess the level of perceived stress, the demographic information questionnaire and the fertility problem questionnaire (FPI) (8) were completed by the research participants in the intervention and control groups before initiating hormone therapy (before the beginning of the intervention). 2 wk later, at the end of the hormone therapy cycle (end of the intervention), the FPI and the satisfaction questionnaire with the intervention were completed by the research participants. During the intervention, complications checklist was provided to the research participants. The first researcher completed the questionnaires. She followed up on the use of aromatherapy or the occurrence of complications in the research participants via daily phone calls and Eitaa messaging. It should be noted that all questionnaires were provided to the participants in person by the researcher (First author).
2.7. Variables
2.7. Variables
In this study, both intervention and control groups were evaluated in terms of demographic variables, including age, the duration of infertility treatment, the number of intra uterine insemination (IUI) cycles, employment status, income level, insurance status, number of pregnancies, number of live births, number of miscarriages, having another child with your spouse, number of IVF cycles and were homogeneous in both groups. Also, the variable of perceived stress was evaluated in infertile women undergoing IVF treatment. The FPI is a 46-question instrument designed by Newton in 1999 and consists of 5 subtests: social issues, sexual concerns, relationship concerns, childless lifestyle, and need to be a parent. The responses are scored on a 6-point Likert scale from strongly disagree to strongly agree. A high score on this questionnaire indicates high stress in infertility. The minimum possible score is 46, and the maximum is 276. A score between 46 and 92 indicates low levels of infertility stress. A score between 92 and 184 indicates moderate levels of infertility stress. A score above 184 indicates high levels of infertility stress.
2.8. Ethical Considerations
2.8. Ethical Considerations
The study was approved by the ethics committee of Mashhad University of Medical Sciences, Mashhad, Iran (Code: IR.MUMS.NURSE.REC.1403.015). The method was then registered on the Iranian Clinical Trials website (Code: IRCT20240514061798N1, on June 06, 2024, updated on February 27, 2025). Then, a letter of introduction from the Vice President for Research of Mashhad University of Medical Sciences, Mashhad, Iran was presented to the head of the Milad Infertility Center, Mashhad, Iran. Then, complete and comprehensive explanations were presented to the head nurse of the Milad Center and the participants about the objectives of the research. Written informed consent was obtained from all participants. They were assured that their participation in the research was voluntary, that they could withdraw from the study at any time, and that it would not interfere with their treatment, in addition to ensuring that it would remain confidential.
2.9. Statistical Analysis
2.9. Statistical Analysis
After data collection, the information was compared and analyzed using Statistical Package for the Social Sciences software (version 26) using statistical analyses at a significance level of 0.05 between the 2 groups. The distribution of quantitative study variables between the 2 groups was compared using an independent t test (if the data distribution was normal) or Mann-Whitney (if the data distribution was not normal). To examine response variables over time, paired t test (if data distribution is normal) and Wilcoxon test (if data is not normal) were used. To investigate the effect of the intervention while controlling pre-intervention measures and other independent variables, the analysis of the covariance model was used.
3. Results
3. Results
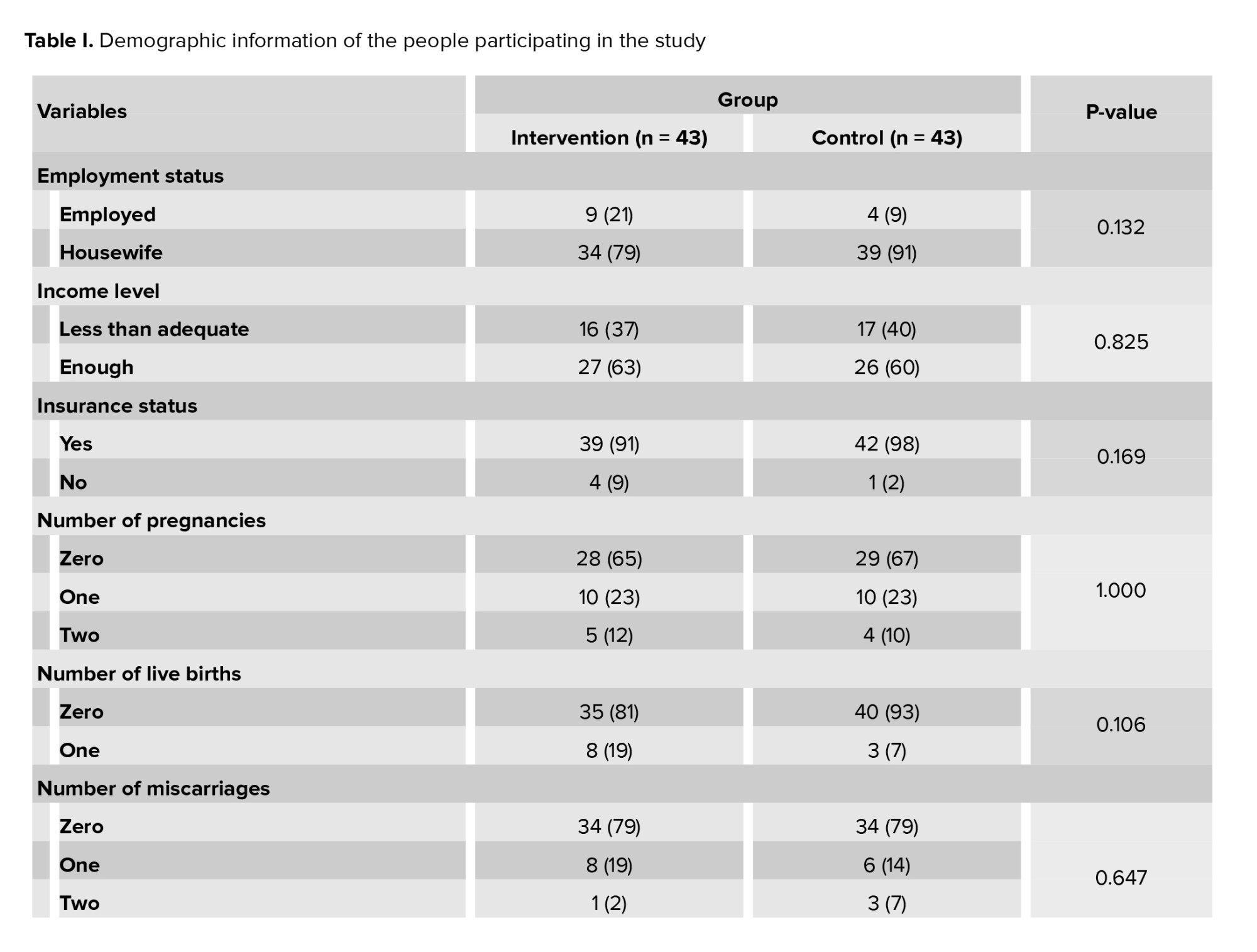
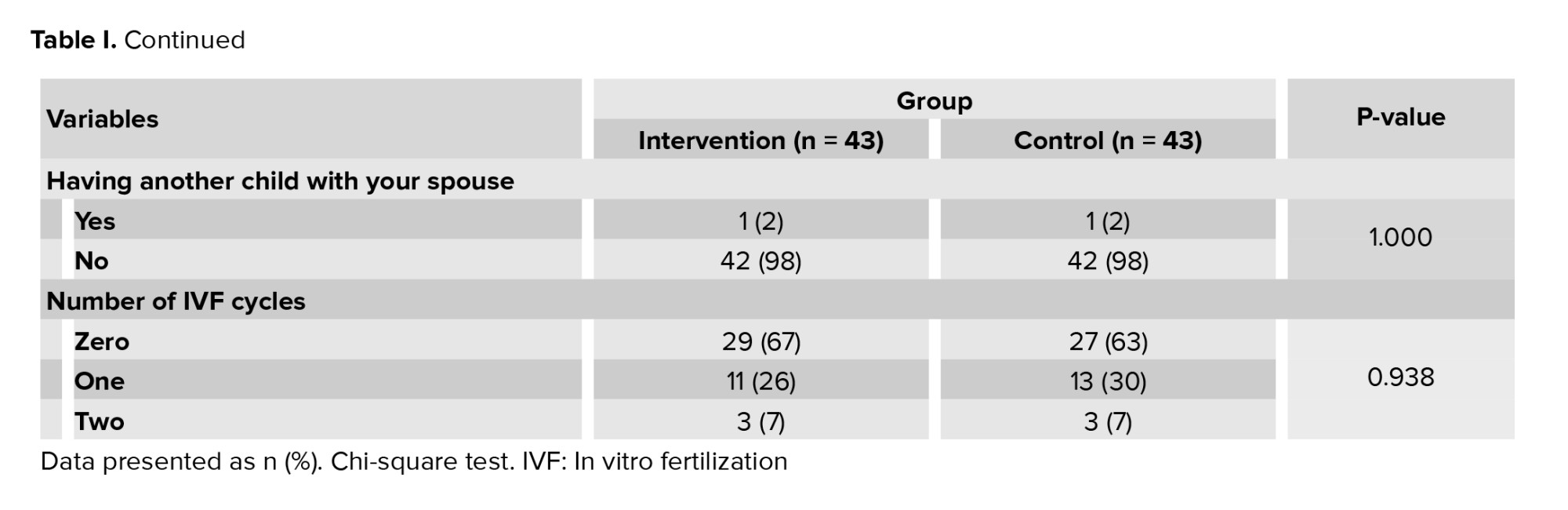
In total, 86 people who had the inclusion criteria participated in this study (Figure 1). The mean age of women in the intervention and control groups was 32.7 ± 6.5 and 33 ± 5.3 yr. The duration of infertility treatment in the intervention and control groups was 4.5 ± 3.7 and 3.8 ± 2.1 yr. Also, the number of IUI cycles in the intervention and control groups was 0.9 ± 0.9 and 1.1 ± 1. According to the independent t test, no statistically significant difference was observed in the age distribution (p = 0.829), and according to the Mann-Whitney test, the duration of infertility treatment (p = 0.879) and the number of IUIs (p = 0.51) in both intervention and control groups and the 2 groups were homogeneous with each other. Other demographic information, including employment status (p = 0.132), income level (p = 0.825), insurance status (p = 0.169), number of pregnancies (p = 1.000), number of live births (p = 0.106), number of miscarriages (p = 0.647), having another child with the spouse (p = 1.000) and number of IVF cycles (p = 0.938), did not show any significant statistical difference between the 2 intervention and control groups based on the Chi-square test, and the 2 groups were similar to each other (Table I).
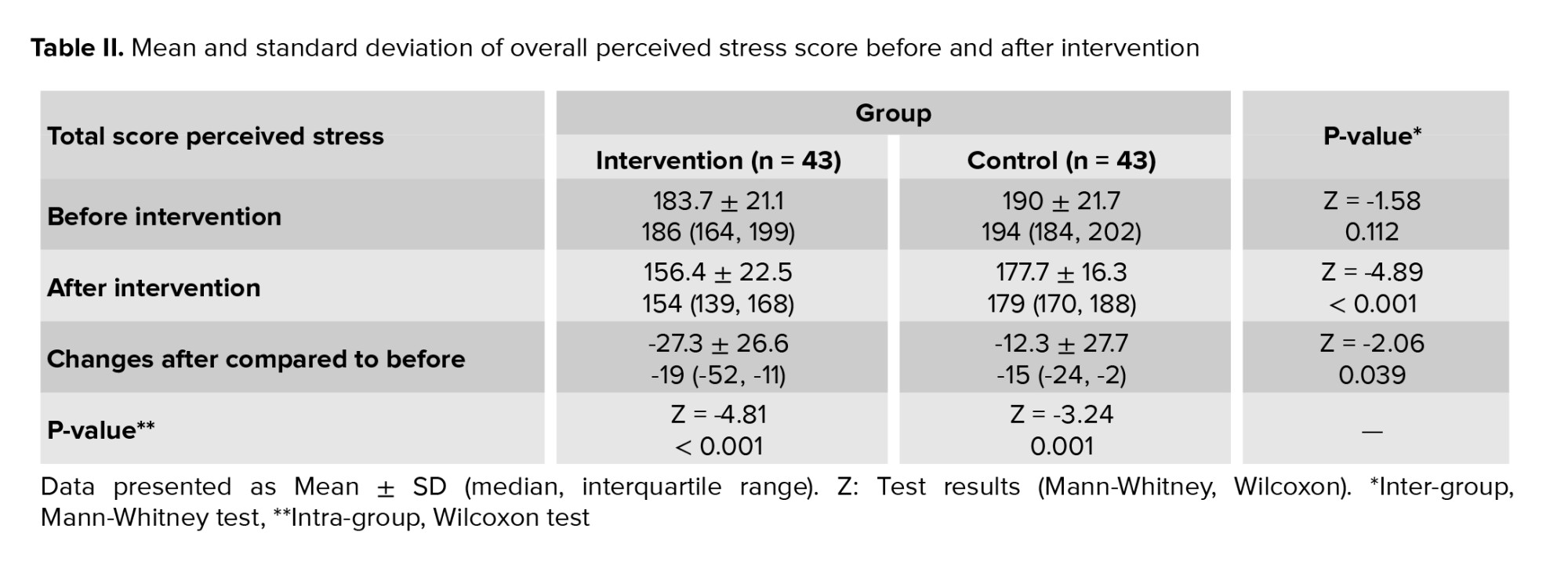
Before the intervention, the mean and standard deviation of the overall stress score of participants in the intervention group was 183.7 ± 21.1, and in the control group, it was 190 ± 21.7. No significant difference was observed in the Mann-Whitney test (p = 0.112). After the intervention, the mean and standard deviation of the total stress score of the participants in the intervention group was 156.4 ± 22.5, and in the control group was 177.7 ± 16.3. The Mann-Whitney test showed this difference to be significant (p < 0.001). The mean total stress score decreased by -27.3 ± 26.6 and -12.3 ± 27.7 in the intervention and control groups, respectively, compared to before the intervention. The Mann-Whitney test showed this difference to be significant (p = 0.039). In the intra-group comparison, the Wilcoxon test results showed that in the intervention group, the mean total stress score after the intervention was lower than the mean before the intervention, and a statistically significant difference was observed (p < 0.001). Also, the result of the Wilcoxon test showed that in the control group, the mean total stress score after the intervention was significantly different from the mean before the intervention (p = 0.001) (Table II).
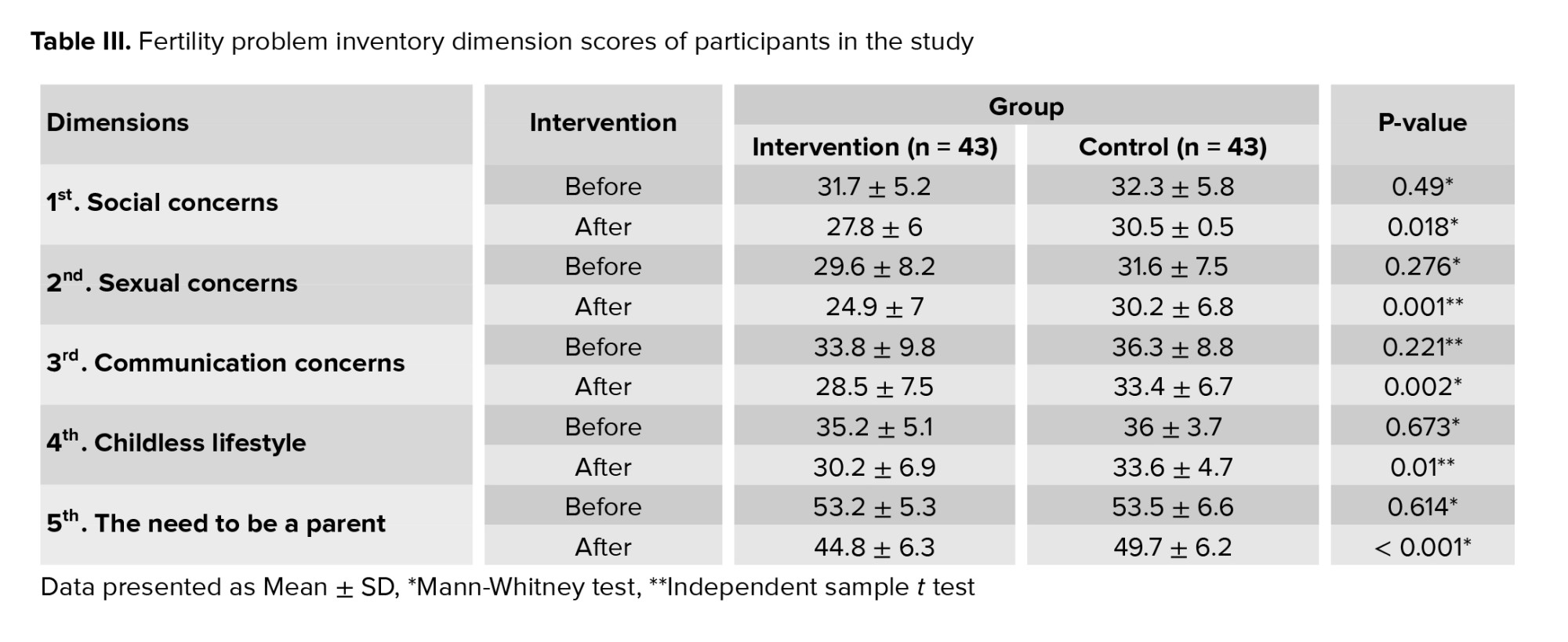
Based on the results obtained, aromatherapy had a significant effect on the dimensions of the FPI after the intervention compared to before the intervention (p < 0.05) (Table III).
4. Discussion
Before the intervention, the mean and standard deviation of the overall stress score of participants in the intervention group was 183.7 ± 21.1, and in the control group, it was 190 ± 21.7. No significant difference was observed in the Mann-Whitney test (p = 0.112). After the intervention, the mean and standard deviation of the total stress score of the participants in the intervention group was 156.4 ± 22.5, and in the control group was 177.7 ± 16.3. The Mann-Whitney test showed this difference to be significant (p < 0.001). The mean total stress score decreased by -27.3 ± 26.6 and -12.3 ± 27.7 in the intervention and control groups, respectively, compared to before the intervention. The Mann-Whitney test showed this difference to be significant (p = 0.039). In the intra-group comparison, the Wilcoxon test results showed that in the intervention group, the mean total stress score after the intervention was lower than the mean before the intervention, and a statistically significant difference was observed (p < 0.001). Also, the result of the Wilcoxon test showed that in the control group, the mean total stress score after the intervention was significantly different from the mean before the intervention (p = 0.001) (Table II).
Based on the results obtained, aromatherapy had a significant effect on the dimensions of the FPI after the intervention compared to before the intervention (p < 0.05) (Table III).
4. Discussion
The present study indicated that before the intervention, the mean stress in infertile women undergoing IVF treatment did not differ significantly between the intervention and control groups. Still, after the intervention, the mean stress in the aromatherapy group with lemon balm essential oil decreased significantly.
One study evaluated the effects of group counseling with a mindfulness‐based program on the specific stress of infertile women, concluding that the difference in the mean total stress score after the intervention was significant between the control and intervention groups (p = 0.001). This study used a group counseling method in which infertile women had to participate in 10 in-person group counseling sessions lasting for 90 min. The stress measurement tool was the Lipp's Stress Symptoms Inventory. This is a stress measurement tool in general, but in the present study, a specific infertility stress tool was used; however, counseling people takes a lot of time and also involves various costs, including travel for the participants (24). Also, counseling requires skills, manpower, and more time and money. Still, aromatherapy does not have limitations of skills, time, money, and travel time, so it is easier to use. The person heals his body and mind by smelling specific essential oils.
Another study evaluated the effects of aromatherapy with rose on the level of anxiety, stress, and depression in mothers of children with cancer, concluded that the average stress score of mothers of children with cancer in the intervention group was different before and after the intervention. In contrast, in the control group, these scores did not differ significantly. Also, a statistically significant difference was observed between the stress scores of mothers of children with cancer in the control and intervention groups after aromatherapy rose (p = 0.001) (25). This study, like the present research, used aromatherapy, and had similar intervention period of 2 wk. Also, in both studies, aromatherapy reduced stress in high-stress situations.
Another study evaluated the effects of aromatherapy with lavender extract on the occupational stress level of operating room personnel, concluded that aromatherapy had a significant effect only on one symptom of occupational stress, which was a feeling of calm in the workplace. No statistically significant difference was observed in the overall level of job stress of personnel between before and after the intervention (26). The reason for the inconsistency of the results of the above study with the present study may be that although both studies used aromatherapy, this study was conducted on shift nurses, and the stressors are different in the 2 societies (26). However, the conditions for aromatherapy to be most effective are to perform it in a calm environment and conditions, which were observed in the present study. However, it was probably not possible for nurses to comply with this point due to their busy work schedule during their shifts. Also, the sample size in this study was 25 people, while in the present research it was 86. The stress measurement tool in this study was standard nursing stress measurement questionnaires, a researcher-made questionnaire, but in the present study, the standard FPI was used.
Aromatherapy is a complementary and alternative therapy (27). Various studies have shown its effects on reducing pregnancy complications, relieving pain, reducing the side effects of cancer treatments, controlling epileptic seizures, and reducing respiratory problems (28-30).
Nowadays, complementary therapies in the healthcare system are highly emphasized, such that they are considered a psychological factor aimed at creating calm in stressful situations. They are a suitable for therapeutic intervention and are inexpensive and non-invasive tools that medical staff can easily implement in the clinic (25).
Typically, the mainstay of stress treatment is the use of chemical medications. However, these medications are not effective for everyone. In addition, it often causes unwanted side effects and increases treatment costs; therefore, using nonpharmacological methods in combination with pharmacological methods reduces stress. Aromatherapy is an accepted intervention because of its simple and low-risk characteristics, and does not require specific time or expensive equipment (25).
Inhaled aromatherapy with lemon balm essential oil may interact with the autonomic nervous system to help relax and reduce stress levels (31).
A study by Caballero-Gallardo et al. highlights the potential benefits of aromatic plants and aromatherapy in enhancing patient well-being. Furthermore, they emphasize the importance of conducting further research to ensure the safety and effectiveness of these treatments (32).
4.1. Strengths and limitations
One of the limitations of this study was the lack of blinding of the research participants due to the presence of an odor in lemon balm essential oil and the absence of an odor in the placebo.
5. Conclusion
One study evaluated the effects of group counseling with a mindfulness‐based program on the specific stress of infertile women, concluding that the difference in the mean total stress score after the intervention was significant between the control and intervention groups (p = 0.001). This study used a group counseling method in which infertile women had to participate in 10 in-person group counseling sessions lasting for 90 min. The stress measurement tool was the Lipp's Stress Symptoms Inventory. This is a stress measurement tool in general, but in the present study, a specific infertility stress tool was used; however, counseling people takes a lot of time and also involves various costs, including travel for the participants (24). Also, counseling requires skills, manpower, and more time and money. Still, aromatherapy does not have limitations of skills, time, money, and travel time, so it is easier to use. The person heals his body and mind by smelling specific essential oils.
Another study evaluated the effects of aromatherapy with rose on the level of anxiety, stress, and depression in mothers of children with cancer, concluded that the average stress score of mothers of children with cancer in the intervention group was different before and after the intervention. In contrast, in the control group, these scores did not differ significantly. Also, a statistically significant difference was observed between the stress scores of mothers of children with cancer in the control and intervention groups after aromatherapy rose (p = 0.001) (25). This study, like the present research, used aromatherapy, and had similar intervention period of 2 wk. Also, in both studies, aromatherapy reduced stress in high-stress situations.
Another study evaluated the effects of aromatherapy with lavender extract on the occupational stress level of operating room personnel, concluded that aromatherapy had a significant effect only on one symptom of occupational stress, which was a feeling of calm in the workplace. No statistically significant difference was observed in the overall level of job stress of personnel between before and after the intervention (26). The reason for the inconsistency of the results of the above study with the present study may be that although both studies used aromatherapy, this study was conducted on shift nurses, and the stressors are different in the 2 societies (26). However, the conditions for aromatherapy to be most effective are to perform it in a calm environment and conditions, which were observed in the present study. However, it was probably not possible for nurses to comply with this point due to their busy work schedule during their shifts. Also, the sample size in this study was 25 people, while in the present research it was 86. The stress measurement tool in this study was standard nursing stress measurement questionnaires, a researcher-made questionnaire, but in the present study, the standard FPI was used.
Aromatherapy is a complementary and alternative therapy (27). Various studies have shown its effects on reducing pregnancy complications, relieving pain, reducing the side effects of cancer treatments, controlling epileptic seizures, and reducing respiratory problems (28-30).
Nowadays, complementary therapies in the healthcare system are highly emphasized, such that they are considered a psychological factor aimed at creating calm in stressful situations. They are a suitable for therapeutic intervention and are inexpensive and non-invasive tools that medical staff can easily implement in the clinic (25).
Typically, the mainstay of stress treatment is the use of chemical medications. However, these medications are not effective for everyone. In addition, it often causes unwanted side effects and increases treatment costs; therefore, using nonpharmacological methods in combination with pharmacological methods reduces stress. Aromatherapy is an accepted intervention because of its simple and low-risk characteristics, and does not require specific time or expensive equipment (25).
Inhaled aromatherapy with lemon balm essential oil may interact with the autonomic nervous system to help relax and reduce stress levels (31).
A study by Caballero-Gallardo et al. highlights the potential benefits of aromatic plants and aromatherapy in enhancing patient well-being. Furthermore, they emphasize the importance of conducting further research to ensure the safety and effectiveness of these treatments (32).
4.1. Strengths and limitations
One of the limitations of this study was the lack of blinding of the research participants due to the presence of an odor in lemon balm essential oil and the absence of an odor in the placebo.
5. Conclusion
Aromatherapy with lemon balm essential oil reduces stress in infertile women undergoing IVF treatment and significantly reduces their stress levels. Stress is one of the factors affecting the results of infertility treatment. It is hoped that the results of this study will be used in related clinical services. The application of the results can help improve the quality of health services, improve the experience of infertile women undergoing treatment, and reduce side effects caused by stress during treatment.
Data Availability
The data from this study are available upon reasonable request from the corresponding author without compromising the confidentiality of participant information.
Author Contributions
K. Mirzakhani and N. Abdollahi Senu designed the study and conducted the research K. Mirzakhani, R. Salari, and V. Ghavami monitored, evaluated, and analyzed the results of the study, and also reviewed the article. All authors approved the final manuscript and take responsibility for the integrity of the data.
Acknowledgments
This article is taken from a master's thesis (Narges Abdollahi Senu) in midwifery, which has been approved and financially supported by the Vice Chancellor for Research and Technology of Mashhad University of Medical Sciences, Mashhad, Iran (research project code: 4021564). The researchers would like to express their gratitude to the Vice Chancellor. They would also like to thank all the participants in this study and the staff of the Milad Infertility Center, Mashhad, Iran. Also, this article does not use artificial intelligence in any part of the process, including translation, editing, or grammar checking.
Conflict of Interest
The authors declare that there is no conflict of interest.
Data Availability
The data from this study are available upon reasonable request from the corresponding author without compromising the confidentiality of participant information.
Author Contributions
K. Mirzakhani and N. Abdollahi Senu designed the study and conducted the research K. Mirzakhani, R. Salari, and V. Ghavami monitored, evaluated, and analyzed the results of the study, and also reviewed the article. All authors approved the final manuscript and take responsibility for the integrity of the data.
Acknowledgments
This article is taken from a master's thesis (Narges Abdollahi Senu) in midwifery, which has been approved and financially supported by the Vice Chancellor for Research and Technology of Mashhad University of Medical Sciences, Mashhad, Iran (research project code: 4021564). The researchers would like to express their gratitude to the Vice Chancellor. They would also like to thank all the participants in this study and the staff of the Milad Infertility Center, Mashhad, Iran. Also, this article does not use artificial intelligence in any part of the process, including translation, editing, or grammar checking.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
