
International Journal of
Reproductive Biomedicine
Thu, Jun 11, 2026
[Archive]
Volume 24, Issue 2 (February 2026)
IJRM 2026, 24(2): 89-100 |
Back to browse issues page
Ethics code: IR.TUMS.IKHC.REC.1403.124
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khazardoust S, Zamanpour Z, Aliasgharpoor M, Shafaat M A, Hamidi Madani Z, Ghalandari M. Evaluating the diagnostic efficacy of cervical length and angles in predicting delivery mode: A cross-sectional study. IJRM 2026; 24 (2) :89-100
URL: http://ijrm.ir/article-1-3581-en.html
URL: http://ijrm.ir/article-1-3581-en.html
Soghra Khazardoust1 

 , Zeinab Zamanpour2 , Maryam Aliasgharpoor3 , Mohammad Ali Shafaat4 , Zahra Hamidi Madani *5 , Maryam Ghalandari6
, Zeinab Zamanpour2 , Maryam Aliasgharpoor3 , Mohammad Ali Shafaat4 , Zahra Hamidi Madani *5 , Maryam Ghalandari6
, Zeinab Zamanpour2 , Maryam Aliasgharpoor3 , Mohammad Ali Shafaat4 , Zahra Hamidi Madani *5 , Maryam Ghalandari6
1- Department of Obstetrics and Gynecology, Maternal, Fetal and Neonatal Research Center, Family Health Research Institute, Imam Khomeini Hospital Complex, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
2- Department of Obstetrics and Gynecology, School of Medicine, Jundishapour University of Medical Sciences, Ahvaz, Iran.
3- Vali-E-Asr Reproductive Health Research Center, Family Health Research Institute, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Obstetrics and Gynecology, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5- Department of Obstetrics and Gynecology, Reproductive Health Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran. ,Zahra_hamidi@gums.ac.ir; Tannaz.hamid1369@gmail.com
6- Vice-Chancellorship of Research and Technology, Guilan University of Medical Sciences, Rasht, Iran.
2- Department of Obstetrics and Gynecology, School of Medicine, Jundishapour University of Medical Sciences, Ahvaz, Iran.
3- Vali-E-Asr Reproductive Health Research Center, Family Health Research Institute, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
4- Department of Obstetrics and Gynecology, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
5- Department of Obstetrics and Gynecology, Reproductive Health Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran. ,
6- Vice-Chancellorship of Research and Technology, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 1069 kb]
(303 Downloads)
| Abstract (HTML) (468 Views)
Full-Text: (48 Views)
1. Introduction
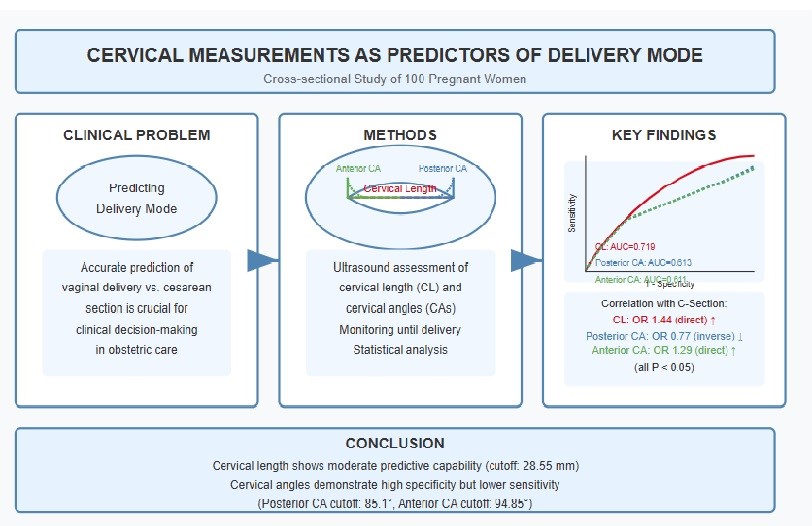
Labor or delivery can occur via vaginal delivery or cesarean section, each with distinct implications for maternal and neonatal health. Vaginal delivery is generally preferred due to its association with lower maternal morbidity and shorter recovery times; it is considered safest when the newborn is full-term (1). However, certain conditions, such as a low-lying placenta, can complicate vaginal delivery, though studies indicate that successful vaginal births can still occur in these cases with appropriate monitoring (2). In contrast, cesarean sections are often performed when vaginal delivery poses risks, such as fetal distress or abnormal positioning; however, they carry higher risks of complications like infection and longer recovery periods (3, 4). Research has also highlighted that infants delivered vaginally benefit from exposure to maternal microbiota, which may play a crucial role in their immune system development, whereas cesarean section infants may experience altered gut flora (4). Ultimately, the choice between vaginal delivery and cesarean should be made collaboratively between the expectant mother and her healthcare provider, considering individual circumstances and potential risks (3, 5).
Accurate forecasting of labor progression and prompt decision-making regarding delivery methods can significantly enhance pregnancy outcomes while also minimizing unnecessary time and resources spent on vaginal deliveries (6). Cervical length (CL) is a critical parameter in predicting labor outcomes, particularly in the context of labor induction. Previous studies have demonstrated that shorter CLs are associated with higher rates of successful vaginal delivery and lower cesarean section rates. For instance, a prospective study found that CL measurement of < 30 mm significantly correlated with successful labor induction, highlighting its predictive value over traditional methods such as the Bishop score, which has limitations in diverse patient populations (7). Furthermore, the systematic review indicated that CL had a pooled sensitivity of 67% and specificity of 70% for predicting successful induction outcomes, making it a reliable indicator for clinicians (8).
In addition to CL, the assessment of cervical angles (CA), specifically the posterior and anterior CAs, has emerged as an important factor in predicting labor outcomes. The posterior CA has shown promise in enhancing the predictive accuracy of labor induction outcomes. A study reported that posterior CA measurements had a higher diagnostic performance compared to traditional scoring systems (9). These findings suggest that incorporating both CL and CA into clinical practice may provide a more comprehensive assessment of labor readiness and improve decision-making regarding labor induction strategies. Overall, utilizing these sonographic measures can lead to better maternal and neonatal outcomes during labor (10).
Overall, the ability to accurately predict labor outcomes is crucial for optimizing maternal and neonatal health, particularly in high-risk pregnancies. This study aimed to assess the predictive value of CL and various CAs, including the uterocervical angle, in determining labor outcomes in terms of delivery mode, specifically, whether labor would result in a cesarean section or a vaginal birth. By analyzing the correlations between these cervical metrics and delivery mode, the study aimed to establish cutoffs for CL and angles that optimize predictive accuracy.
Ultimately, this research aimed to enhance clinical decision-making regarding labor management by identifying reliable indicators for cesarean section risk.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study was conducted on 100 pregnant women who underwent ultrasound assessments to measure CL and CA at Imam Khomeini hospital, Tehran, Iran, from June to December 2024.
Demographic data were collected through a structured checklist, and each participant underwent an ultrasound to measure CL, posterior CA, and anterior CA.
The participants were followed until the induction of labor (IOL) (without interference by researchers in the labor process, such as induction and necessary interventions), with delivery mode recorded as either successful vaginal delivery or cesarean section. After the completion of data collection, the women who had a successful vaginal delivery were allocated to the vaginal delivery group (n = 85), and the women who underwent a cesarean section were assigned to the cesarean section group (n = 15). Following data collection, statistical tests were employed to compare the results between the 2 groups, and the diagnostic value of cervical measurements was assessed by calculating accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) to predict delivery mode.
This comprehensive approach aimed to elucidate the significance of cervical parameters in determining labor outcomes.
2.2. Inclusion and exclusion criteria
The inclusion criteria comprised women aged between 18 and 45 yr referred to Imam Khomein hospital, Tehran, Iran, who were nulliparous women, with singleton fetus, no history of previous cervical surgeries, cephalic presentation, and term labor (gestational age ≥ 37 wk) at the time of the assessment.
Pregnant women with confirmed fetal abnormalities, a Bishop score > 8, antepartum bleeding, cephalopelvic disproportion, pathological obesity (body mass index > 40 kg/m²), macrosomic fetuses, and those undergoing elective cesarean section due to maternal or fetal reasons were excluded from the study. The inclusion and exclusion criteria were checked before the beginning of the study by an interview with mothers, clinical documents, and ultrasound assessment.
2.3. Data collection
Data for this study were systematically gathered using a multifaceted approach that integrated direct observation, structured interviews with mothers, and detailed ultrasound assessments. Demographic variables, including maternal age and other relevant background characteristics, were primarily obtained through interviews with the mothers and corroborated with information from clinical records.
Ultrasound examinations were conducted on all participating mothers upon reaching at least the 37th wk of gestation, defined as term pregnancy, during which a range of clinical parameters were measured. These included the location of the placenta, fetal presentation and position, estimated gestational age and fetal weight, as well as specific anatomical measurements such as CL and the anterior and posterior CAs, which are pertinent to evaluating readiness for labor and potential delivery mode. Following these initial assessments, the mothers were prospectively monitored through the remainder of their pregnancies. During this follow-up period, comprehensive data were recorded, encompassing the method of labor induction (if performed), gestational age and weight of the infant at birth, the duration of both induction and labor, and the ultimate mode of delivery, categorized as either vaginal birth or cesarean section.
2.4. CAs measurement
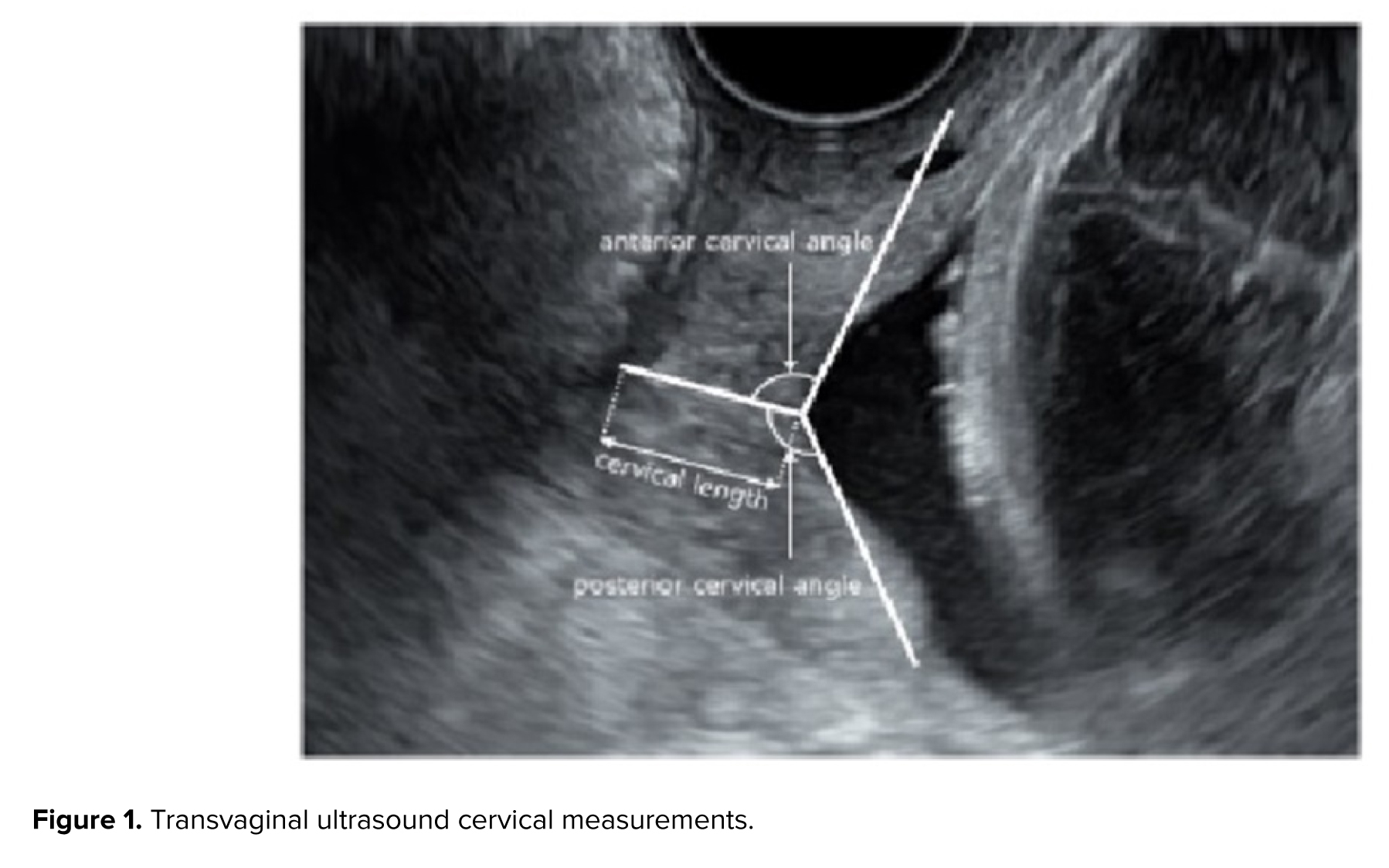
Ultrasound examinations were performed by an experienced sonographer using a Philips Affinity 50 ultrasound machine equipped with a 5-9 MHz transvaginal probe. Women were placed in the supine position with hips flexed and abducted, knees flexed, and with an empty bladder. The vaginal transducer was covered with a single-use sterile vinyl sheath. Care was taken to ensure that the ultrasound images included both the internal and external cervical os (the opening of the cervix) as well as the outermost part of the fetal presenting part. The CL was measured as the distance between the internal and external cervical os. The anterior and posterior CA were calculated by drawing 2 lines converging at the internal cervical os. Specifically, the posterior CA was defined as the angle between an imaginary line crossing the cervical canal and another tangential to the posterior uterine wall at its junction with the internal os, assessed in the sagittal plane at the level of the internal os. Presence of funneling was also recorded (Figure 1).
2.5. Outcomes
The study primarily aimed to investigate the relationship between cervical measurement parameters, specifically the CL and the dimensions of its posterior and anterior angles, and the final delivery mode, distinguishing between vaginal delivery and cesarean section. Additionally, the secondary outcome focused on identifying a cutoff point for these cervical parameters while evaluating their diagnostic value in predicting delivery mode.
2.6. Sample size
The sample size was calculated using the standard formula for prevalence estimation in cross-sectional studies, assuming a conservative prevalence (p) of 70% (α = 0.7) to maximize the required sample size and a margin of error (d) of 9% (d = 0.09). The calculation yielded:
This was rounded to 100 participants to account for potential attrition and ensure sufficient statistical power for evaluating the diagnostic efficacy of CL and CAs.
2.7. Ethical Considerations
This study was approved by the Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.IKHC.REC.1403.124). The research was conducted under the tenets of the Declaration of Helsinki. Informed written consent was obtained from all study participants.
2.8. Statistical Analysis
The Statistical Package for the Social Sciences (SPSS), version 17.0, SPSS Inc., Chicago, Illinois, USA was used for conducting the statistical analysis. The normality of quantitative variables was assessed using the Kolmogorov-Smirnov test, while differences between groups were examined with the independent t test for quantitative data and Fisher's exact test for qualitative variables.
Univariate and multivariate logistic regression analyses were employed to predict delivery mode, calculating odds ratios (ORs) with 95% confidence intervals (CIs). The optimal cut-off values for CL, posterior CA, and anterior CA were determined through receiver operating characteristic (ROC) curve analysis, utilizing the area under the ROC curve (AUC) to compare each parameter's predictive effectiveness. Additionally, diagnostic accuracy metrics such as sensitivity, specificity, PPV, NPV, and overall accuracy were computed for CL and both angles. P < 0.05 was considered statistically significant.
3. Results
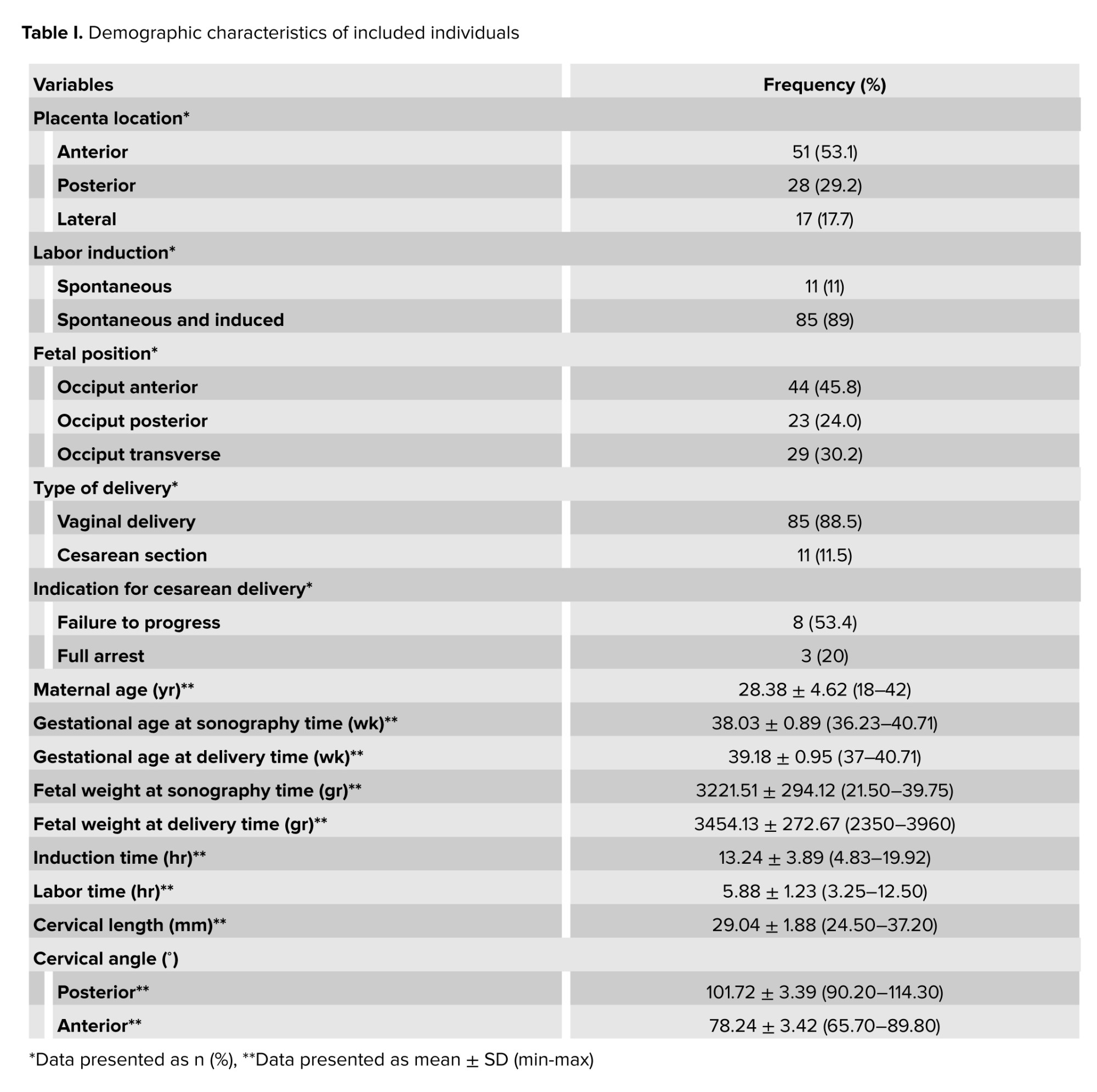
In this cross-sectional study, a total of 100 eligible participants were included in the study, with 4 exclusions during the initial stage. The participants comprised nulliparous pregnant women at 37 wk or later who had visited Imam Khomeini hospital, Tehran, Iran. Among them, 11 individuals underwent cesarean sections (failure to progress during labor was the most commonly observed reason), while 85 individuals had successful vaginal deliveries. The results indicated that the anterior was the most common regarding placenta location. Among labor induction methods, a combination of spontaneous and induced was the most common. Fetal positioning was classified into occiput anterior, posterior, and transverse orientations, with the occiput anterior predominant. Delivery was commonly done through the vaginal route, with a smaller proportion resulting in cesarean sections. Average maternal age were the ones in their late twenties, while gestational ages at both sonography and delivery times were typically near full term. Fetal weights at both sonography and delivery times reflect a range of healthy weights. The mean induction time was longer than half a day, alongside labor duration, which is relatively brief. Additionally, cervical measurements such as length and angles are documented, indicating a range of anatomical variations during the delivery process (Table I).
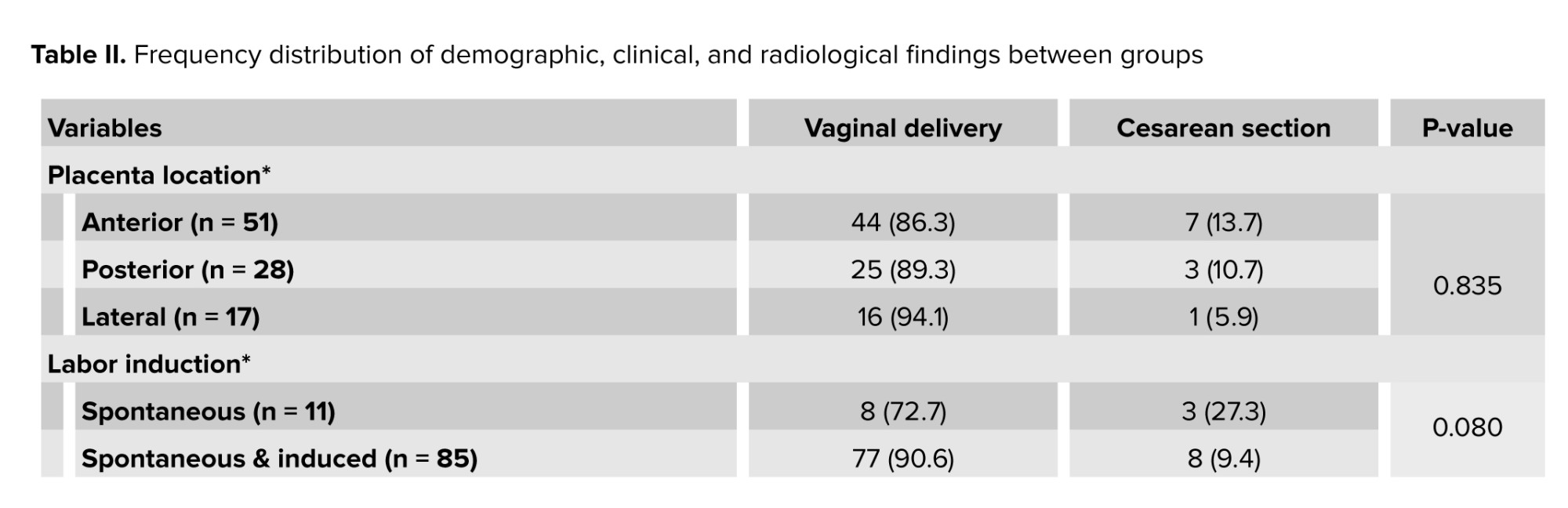
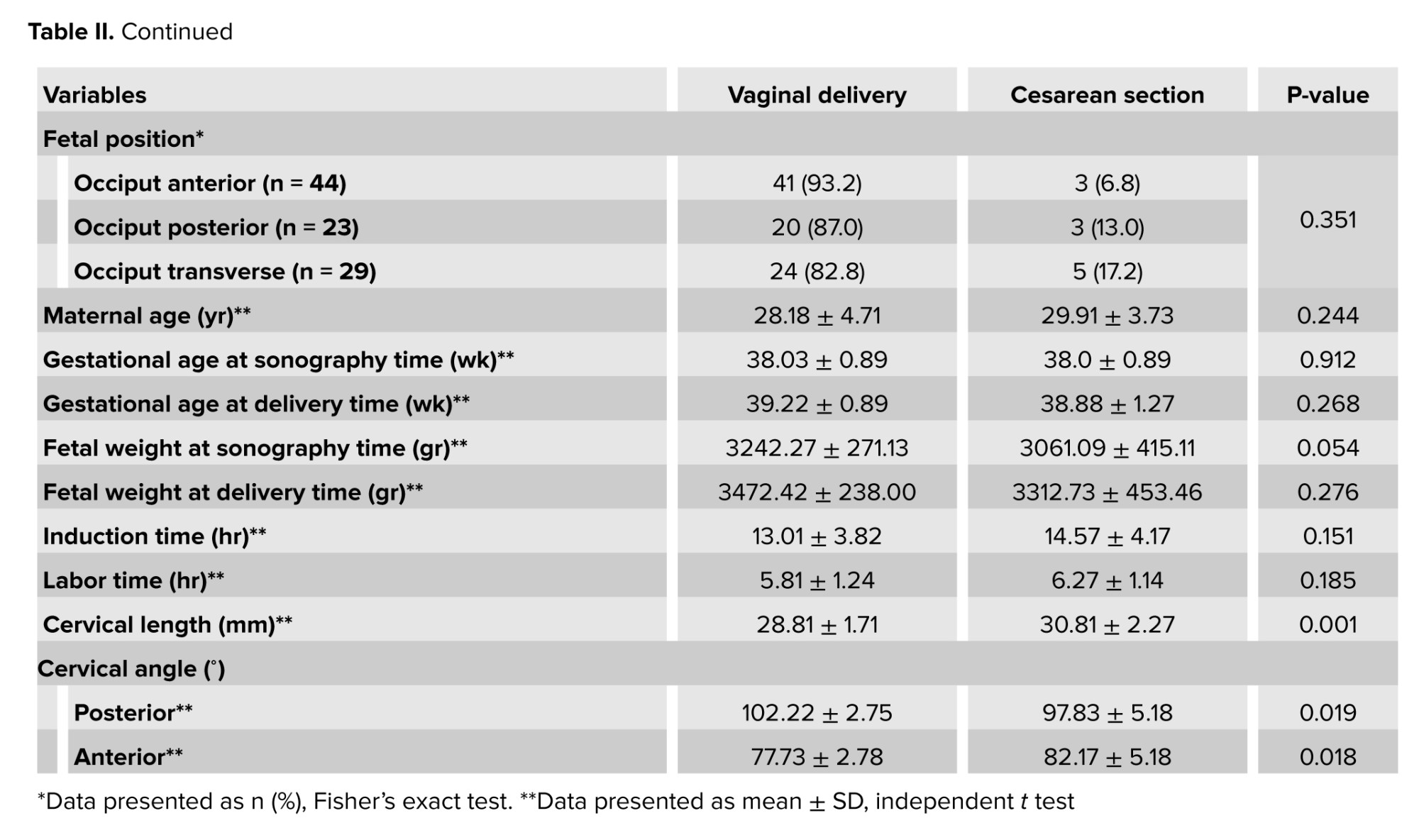
The results indicated that the frequency distribution of demographic and clinical characteristics among the studied samples, including maternal age, placental location, methods of labor induction, fetal position during delivery, gestational age, fetal weight, and the duration of labor and induction, did not show statistically significant differences between the 2 groups of mothers who underwent vaginal delivery and those who had cesarean sections. However, a statistically significant difference was observed in the average CL and the measurements of posterior and anterior CAs between the 2 groups. Specifically, the length and anterior angle of the cervix were significantly smaller in mothers who experienced vaginal delivery compared to those who underwent cesarean sections, while the posterior angle measurement was notably greater in this group (Table II).
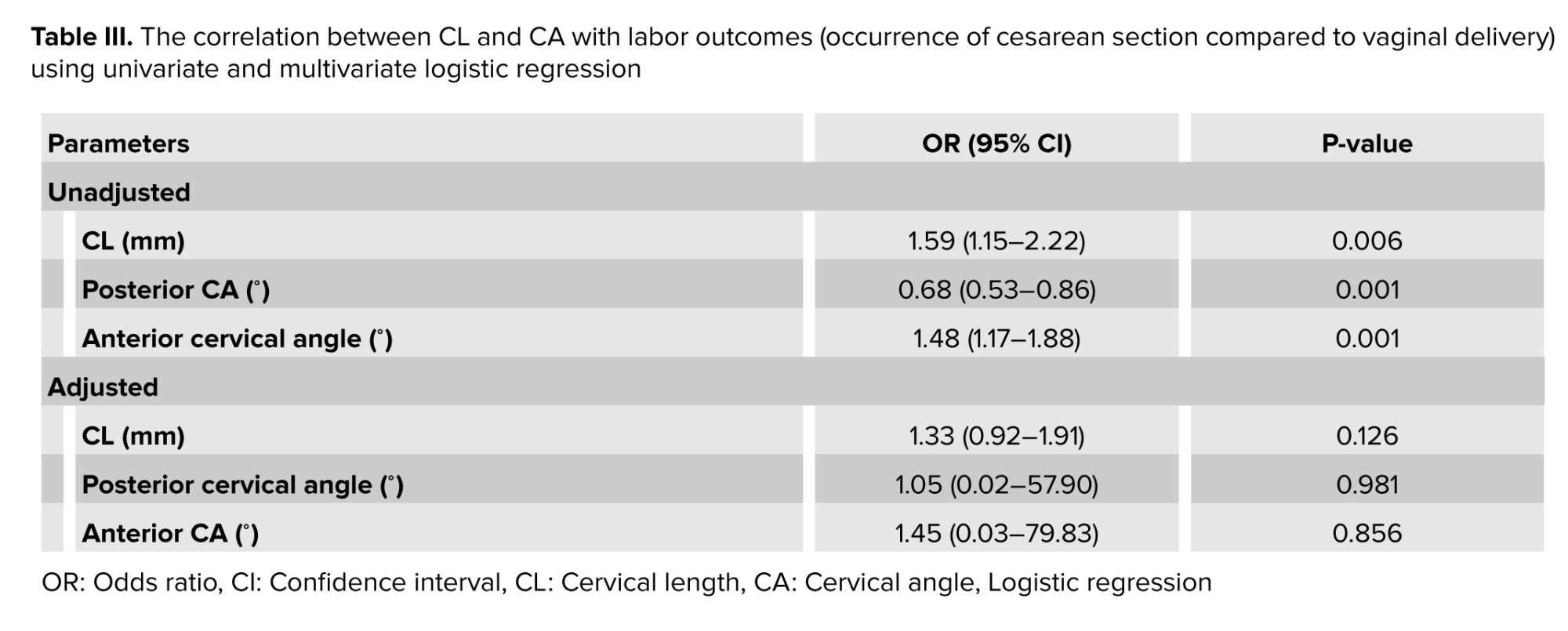
In the analysis of diagnostic parameters related to successful labor delivery, both univariate and multivariate regression models were employed to assess the influence of CL and CAs. The unadjusted model indicated that CL was positively associated with a cesarean section with an OR of 1.59, indicating that an increase of each millimeter of CL may increase the 59% likelihood of cesarean section; while the posterior CA showed a negative association, suggesting that an increase in this angle may decrease the 32% likelihood of cesarean section occurrence.
Conversely, the anterior CA demonstrated a positive correlation with the occurrence of cesarean section, with an OR of 1.48, indicating that an increase of each degree of anterior CA may increase the likelihood of cesarean section by 48%. In the adjusted model, CL maintained a positive association, although it was not statistically significant. The posterior CA did not show a significant relationship in this model, while the anterior CA continued to indicate a positive association without statistical significance (Table III).
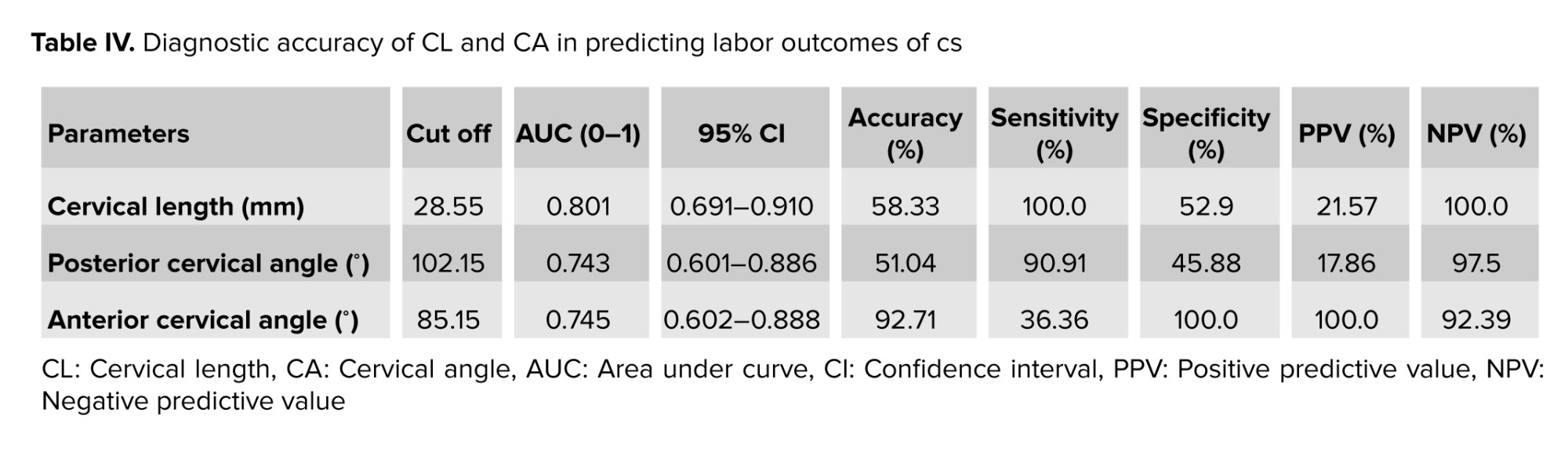
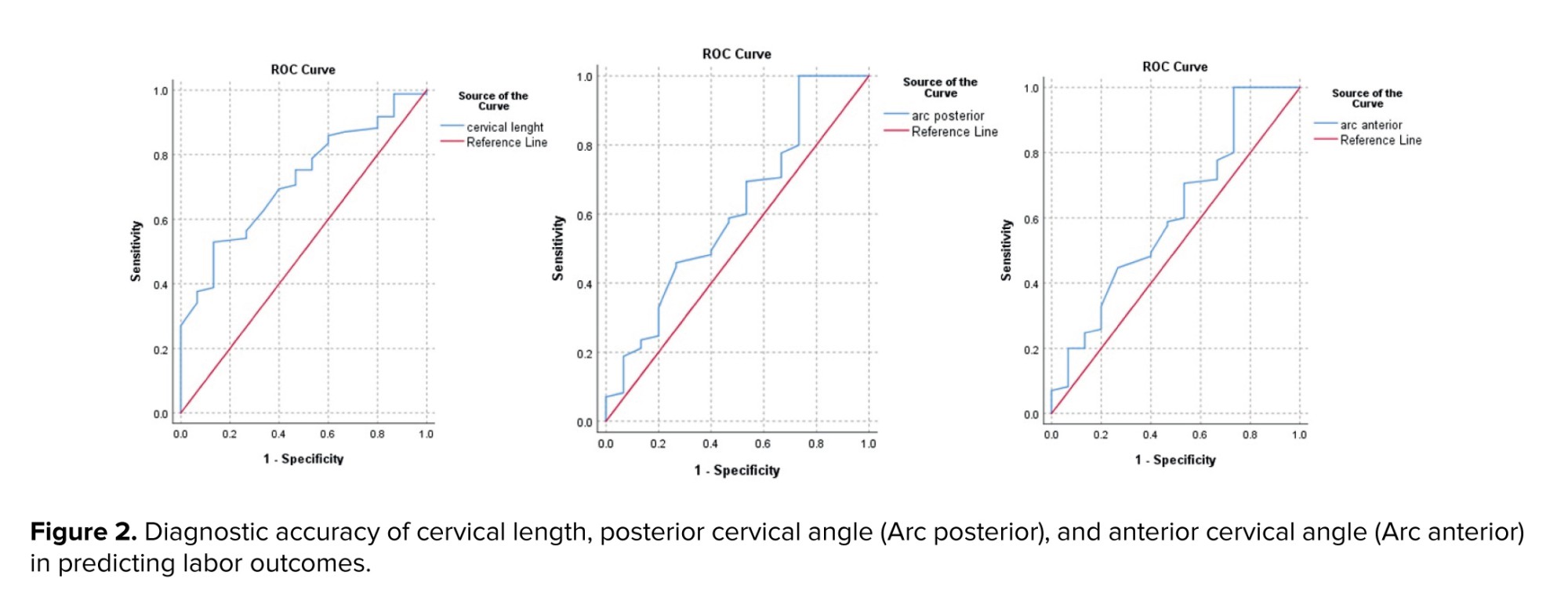
The diagnostic accuracy of CL and CA in predicting labor outcomes can be summarized as follows: for CL, when measured at a cutoff of 28.55 mm, demonstrated a moderate ability to distinguish between successful and unsuccessful labor outcomes, with high sensitivity and NPV, but only fair specificity. In comparison, assessing the posterior CA at its optimal cutoff of 102.1° provided strong sensitivity and NPV, although its specificity was lower. The anterior CA performed at a cutoff of 85.15°, achieving high specificity and predictive value, but with limited sensitivity (Table IV and Figure 2).
4. Discussion
In this study, the assessment of CL and angles demonstrated significant relationships with labor outcomes. Specifically, CL and the anterior CA showed a direct significant correlation, while the posterior CA exhibited a significant inverse correlation with the likelihood of cesarean sections. The diagnostic accuracy metrics reveal that CL possesses moderate predictive capability for labor outcomes. The posterior demonstrated high sensitivity whereas the anterior CA had high specificity but lower sensitivity levels.
In this study, a cutoff value of 28.55 mm for CL was identified as a significant predictor of labor outcomes. The analysis revealed an accuracy of 58.3%, with a sensitivity of 100.0% and a specificity of 52.9%.
These metrics suggest that while the cutoff is relatively effective in identifying those at risk of cesarean section, it may also yield a considerable number of false positives. Similar to our study, a previous study indicated that a CL of 21 mm has shown 72.2% sensitivity and 79.1% specificity for cesarean delivery, while a CL of 22 mm indicated 66.6% sensitivity for labor induction (11). Also, in line with our study, a systematic review indicated that CL has moderate effectiveness in predicting successful IOL with pooled sensitivity and specificity of 67% and 70%, respectively (8). A diagnostic study demonstrated that CL yielded a sensitivity of 91.84% and a specificity of 80.95% in predicting the success of labor induction (12). A meta-analysis study revealed a significant association between CL and the prediction of successful labor induction, indicating that it is a strong predictor of labor outcomes (13). Overall, while the current study's findings contribute valuable insights into the predictive capabilities of CL, the moderate accuracy and specificity indicate that further research is needed to refine these metrics and enhance their clinical applicability in predicting labor outcomes effectively.
In this study, the posterior CA was evaluated as a predictor of labor outcomes, with a cutoff value established at 102.15°. The analysis revealed an AUC of 0.743, indicating moderate discriminative ability. Furthermore, the posterior CA demonstrated an accuracy of 51%, alongside a sensitivity of 90.91% and a specificity of 45.88%.
These metrics suggest that while the cutoff is relatively effective in identifying those at risk of cesarean section, it may also yield a considerable number of false positives.
In a study, the sensitivity and specificity of 91.84 and 90.48, at a cut-point of 99.5° in predicting labor induction success was reported for posterior CA, and they stated that posterior CA has been identified as a reliable measure for predicting successful IOL, with higher sensitivity compared to CL alone (12). A study found that the area under the ROC curve for predicting vaginal delivery based on the posterior CA was 0.667, with a cutoff value of 96.5°, and this predicting value was significant (14). In a study, the authors stated that measuring the CL and posterior CA offers a more objective and accurate prediction of successful labor induction than the Bishop score, owing to the strong correlation between successful induction and the posterior CA (15). Overall, while the posterior CA shows a promising outcome as a predictive tool, its limitations in sensitivity warrant further investigation to enhance its clinical applicability and ensure comprehensive risk assessment for labor outcomes.
In this study, a cutoff of 85.15° of anterior CA (uterocervical) showed an accuracy of 92.7%, a sensitivity of 36.4%, and a specificity of 100% in predicting cesarean section. In a study, the authors found that a utero CA ≥ 98.86° predicts preterm birth with 91% sensitivity and 75.5% specificity, outperforming CL in this context (16). Overall, while the high specificity of the current study's results is notable, the low sensitivity indicates that while the anterior CA can reliably rule out cesarean delivery when it exceeds the cutoff, it may not effectively predict successful vaginal deliveries, suggesting a need for further investigation into supplementary predictive measures or combined approaches for improved clinical outcomes.
In conclusion, while cervical measurements are valuable in predicting labor outcomes, their effectiveness can vary significantly based on specific contextual factors, including the timing of assessment, the gestational age of the patient, and the unique characteristics of the population being studied. For instance, CL measurements may be more predictive in certain stages of pregnancy or among populations with specific risk factors for preterm labor. Additionally, variations in measurement techniques and the clinician's experience can influence the reliability of these assessments. To enhance predictive accuracy, further research could explore the integration of cervical measures with other clinical indicators, such as maternal demographics, obstetric history, and real-time fetal monitoring data. This multifaceted approach could lead to the development of more comprehensive models that not only improve prediction rates for labor outcomes but also facilitate personalized care strategies tailored to individual patient profiles. By combining cervical assessments with additional clinical parameters, healthcare providers may be better equipped to make informed decisions regarding labor management and intervention strategies, ultimately improving maternal and neonatal outcomes.
4.1. Strengths and Limitations
This study has several limitations; firstly, the sample size of 100 participants may limit the generalizability of the findings, as a larger cohort could provide more robust data and enhance statistical power. Secondly, the study's exclusion criteria, which omitted women with certain complications such as fetal anomalies and pre-labor bleeding, may introduce selection bias, potentially affecting the applicability of the results to broader populations. Additionally, inaccuracies inherent in angle measurements via ultrasound, such as operator dependency, varying fetal and maternal positioning, and equipment limitations, could affect the precision and reliability of the CAs assessments, potentially impacting the diagnostic efficacy reported. Furthermore, the study's observational design does not allow for causal inferences regarding the relationship between cervical metrics and labor outcomes, limiting the ability to definitively establish predictive cutoffs for cesarean section risk. Finally, a significant limitation of this study is the considerable class imbalance, with only 15 out of 100 participants undergoing cesarean sections (of these 15 cases, 4 underwent cesarean section due to fetal distress or meconium-stained amniotic fluid and were not included in the study analysis). This uneven distribution may bias predictive metrics and analytical results, as classification models and statistical analyses often favor the majority group and may inadequately capture the characteristics or predictive factors of the minority class. These factors should be considered when interpreting the results and warrant further validation with larger samples and standardized measurement protocols.
5. Conclusion
The study’s findings indicate that CL and CA measurements exhibit meaningful yet heterogeneous associations with cesarean delivery risk, suggesting that these ultrasound-derived parameters may contribute to a more nuanced understanding of labor progression. While the observed patterns highlight the potential predictive value of these metrics, particularly the differential sensitivity and specificity demonstrated across CL, posterior CA, and anterior CA, they also underscore important methodological constraints. The limited sample size and the inherent variability in CA measurement techniques introduce uncertainty that warrants cautious interpretation. To establish the clinical reliability and applicability of these parameters, future research should prioritize larger, well‑designed studies employing standardized measurement protocols and rigorous analytical approaches, thereby enabling a more definitive assessment of the role of cervical metrics in labor management and cesarean risk stratification.
Data Availability
The data collected for this study are available upon reasonable request to the corresponding author.
Author Contributions
All authors met the 4 criteria for authorship contribution based on recommendations of the International Committee of Medical Journal Editors. S. Khazardoust: Conceptualization, data curation, writing (review and editing of original draft), supervision. Z. Zamanpour: Visualization, investigation, writing (review and editing of original draft). M. Aliasgharpoor: Conceptualization, methodology, formal analysis, writing (review and editing of original draft). M.A. Shafaat: Conceptualization, data curation, writing (review and editing of original draft). Z. Hamidi Madani: Conceptualization, data curation, project management, writing (review and editing of original draft). M. Ghalandari: Conceptualization, validation, writing (review and editing of original draft).
Acknowledgments
We extend our heartfelt appreciation to the participants, medical personnel, and administrative staff at Imam Khomeini hospital, Tehran, Iran for their exceptional support and collaboration throughout this study. Their commitment and cooperation were instrumental in facilitating our research, and we are truly grateful for their invaluable contributions. Tehran University of Medical Sciences, Tehran, Iran, financially supported this study (grant number: 71457). During the preparation of this work, the authors utilized artificial intelligence (Perplexity.ai) to refine grammar points and language style in writing. Subsequently, the authors thoroughly reviewed and edited the content as necessary, taking full responsibility for the publication’s content.
Conflict of Interest
The authors declare that there is no conflict of interest.
Labor or delivery can occur via vaginal delivery or cesarean section, each with distinct implications for maternal and neonatal health. Vaginal delivery is generally preferred due to its association with lower maternal morbidity and shorter recovery times; it is considered safest when the newborn is full-term (1). However, certain conditions, such as a low-lying placenta, can complicate vaginal delivery, though studies indicate that successful vaginal births can still occur in these cases with appropriate monitoring (2). In contrast, cesarean sections are often performed when vaginal delivery poses risks, such as fetal distress or abnormal positioning; however, they carry higher risks of complications like infection and longer recovery periods (3, 4). Research has also highlighted that infants delivered vaginally benefit from exposure to maternal microbiota, which may play a crucial role in their immune system development, whereas cesarean section infants may experience altered gut flora (4). Ultimately, the choice between vaginal delivery and cesarean should be made collaboratively between the expectant mother and her healthcare provider, considering individual circumstances and potential risks (3, 5).
Accurate forecasting of labor progression and prompt decision-making regarding delivery methods can significantly enhance pregnancy outcomes while also minimizing unnecessary time and resources spent on vaginal deliveries (6). Cervical length (CL) is a critical parameter in predicting labor outcomes, particularly in the context of labor induction. Previous studies have demonstrated that shorter CLs are associated with higher rates of successful vaginal delivery and lower cesarean section rates. For instance, a prospective study found that CL measurement of < 30 mm significantly correlated with successful labor induction, highlighting its predictive value over traditional methods such as the Bishop score, which has limitations in diverse patient populations (7). Furthermore, the systematic review indicated that CL had a pooled sensitivity of 67% and specificity of 70% for predicting successful induction outcomes, making it a reliable indicator for clinicians (8).
In addition to CL, the assessment of cervical angles (CA), specifically the posterior and anterior CAs, has emerged as an important factor in predicting labor outcomes. The posterior CA has shown promise in enhancing the predictive accuracy of labor induction outcomes. A study reported that posterior CA measurements had a higher diagnostic performance compared to traditional scoring systems (9). These findings suggest that incorporating both CL and CA into clinical practice may provide a more comprehensive assessment of labor readiness and improve decision-making regarding labor induction strategies. Overall, utilizing these sonographic measures can lead to better maternal and neonatal outcomes during labor (10).
Overall, the ability to accurately predict labor outcomes is crucial for optimizing maternal and neonatal health, particularly in high-risk pregnancies. This study aimed to assess the predictive value of CL and various CAs, including the uterocervical angle, in determining labor outcomes in terms of delivery mode, specifically, whether labor would result in a cesarean section or a vaginal birth. By analyzing the correlations between these cervical metrics and delivery mode, the study aimed to establish cutoffs for CL and angles that optimize predictive accuracy.
Ultimately, this research aimed to enhance clinical decision-making regarding labor management by identifying reliable indicators for cesarean section risk.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study was conducted on 100 pregnant women who underwent ultrasound assessments to measure CL and CA at Imam Khomeini hospital, Tehran, Iran, from June to December 2024.
Demographic data were collected through a structured checklist, and each participant underwent an ultrasound to measure CL, posterior CA, and anterior CA.
The participants were followed until the induction of labor (IOL) (without interference by researchers in the labor process, such as induction and necessary interventions), with delivery mode recorded as either successful vaginal delivery or cesarean section. After the completion of data collection, the women who had a successful vaginal delivery were allocated to the vaginal delivery group (n = 85), and the women who underwent a cesarean section were assigned to the cesarean section group (n = 15). Following data collection, statistical tests were employed to compare the results between the 2 groups, and the diagnostic value of cervical measurements was assessed by calculating accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) to predict delivery mode.
This comprehensive approach aimed to elucidate the significance of cervical parameters in determining labor outcomes.
2.2. Inclusion and exclusion criteria
The inclusion criteria comprised women aged between 18 and 45 yr referred to Imam Khomein hospital, Tehran, Iran, who were nulliparous women, with singleton fetus, no history of previous cervical surgeries, cephalic presentation, and term labor (gestational age ≥ 37 wk) at the time of the assessment.
Pregnant women with confirmed fetal abnormalities, a Bishop score > 8, antepartum bleeding, cephalopelvic disproportion, pathological obesity (body mass index > 40 kg/m²), macrosomic fetuses, and those undergoing elective cesarean section due to maternal or fetal reasons were excluded from the study. The inclusion and exclusion criteria were checked before the beginning of the study by an interview with mothers, clinical documents, and ultrasound assessment.
2.3. Data collection
Data for this study were systematically gathered using a multifaceted approach that integrated direct observation, structured interviews with mothers, and detailed ultrasound assessments. Demographic variables, including maternal age and other relevant background characteristics, were primarily obtained through interviews with the mothers and corroborated with information from clinical records.
Ultrasound examinations were conducted on all participating mothers upon reaching at least the 37th wk of gestation, defined as term pregnancy, during which a range of clinical parameters were measured. These included the location of the placenta, fetal presentation and position, estimated gestational age and fetal weight, as well as specific anatomical measurements such as CL and the anterior and posterior CAs, which are pertinent to evaluating readiness for labor and potential delivery mode. Following these initial assessments, the mothers were prospectively monitored through the remainder of their pregnancies. During this follow-up period, comprehensive data were recorded, encompassing the method of labor induction (if performed), gestational age and weight of the infant at birth, the duration of both induction and labor, and the ultimate mode of delivery, categorized as either vaginal birth or cesarean section.
2.4. CAs measurement
Ultrasound examinations were performed by an experienced sonographer using a Philips Affinity 50 ultrasound machine equipped with a 5-9 MHz transvaginal probe. Women were placed in the supine position with hips flexed and abducted, knees flexed, and with an empty bladder. The vaginal transducer was covered with a single-use sterile vinyl sheath. Care was taken to ensure that the ultrasound images included both the internal and external cervical os (the opening of the cervix) as well as the outermost part of the fetal presenting part. The CL was measured as the distance between the internal and external cervical os. The anterior and posterior CA were calculated by drawing 2 lines converging at the internal cervical os. Specifically, the posterior CA was defined as the angle between an imaginary line crossing the cervical canal and another tangential to the posterior uterine wall at its junction with the internal os, assessed in the sagittal plane at the level of the internal os. Presence of funneling was also recorded (Figure 1).
2.5. Outcomes
The study primarily aimed to investigate the relationship between cervical measurement parameters, specifically the CL and the dimensions of its posterior and anterior angles, and the final delivery mode, distinguishing between vaginal delivery and cesarean section. Additionally, the secondary outcome focused on identifying a cutoff point for these cervical parameters while evaluating their diagnostic value in predicting delivery mode.
2.6. Sample size
The sample size was calculated using the standard formula for prevalence estimation in cross-sectional studies, assuming a conservative prevalence (p) of 70% (α = 0.7) to maximize the required sample size and a margin of error (d) of 9% (d = 0.09). The calculation yielded:
This was rounded to 100 participants to account for potential attrition and ensure sufficient statistical power for evaluating the diagnostic efficacy of CL and CAs.
2.7. Ethical Considerations
This study was approved by the Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.IKHC.REC.1403.124). The research was conducted under the tenets of the Declaration of Helsinki. Informed written consent was obtained from all study participants.
2.8. Statistical Analysis
The Statistical Package for the Social Sciences (SPSS), version 17.0, SPSS Inc., Chicago, Illinois, USA was used for conducting the statistical analysis. The normality of quantitative variables was assessed using the Kolmogorov-Smirnov test, while differences between groups were examined with the independent t test for quantitative data and Fisher's exact test for qualitative variables.
Univariate and multivariate logistic regression analyses were employed to predict delivery mode, calculating odds ratios (ORs) with 95% confidence intervals (CIs). The optimal cut-off values for CL, posterior CA, and anterior CA were determined through receiver operating characteristic (ROC) curve analysis, utilizing the area under the ROC curve (AUC) to compare each parameter's predictive effectiveness. Additionally, diagnostic accuracy metrics such as sensitivity, specificity, PPV, NPV, and overall accuracy were computed for CL and both angles. P < 0.05 was considered statistically significant.
3. Results
In this cross-sectional study, a total of 100 eligible participants were included in the study, with 4 exclusions during the initial stage. The participants comprised nulliparous pregnant women at 37 wk or later who had visited Imam Khomeini hospital, Tehran, Iran. Among them, 11 individuals underwent cesarean sections (failure to progress during labor was the most commonly observed reason), while 85 individuals had successful vaginal deliveries. The results indicated that the anterior was the most common regarding placenta location. Among labor induction methods, a combination of spontaneous and induced was the most common. Fetal positioning was classified into occiput anterior, posterior, and transverse orientations, with the occiput anterior predominant. Delivery was commonly done through the vaginal route, with a smaller proportion resulting in cesarean sections. Average maternal age were the ones in their late twenties, while gestational ages at both sonography and delivery times were typically near full term. Fetal weights at both sonography and delivery times reflect a range of healthy weights. The mean induction time was longer than half a day, alongside labor duration, which is relatively brief. Additionally, cervical measurements such as length and angles are documented, indicating a range of anatomical variations during the delivery process (Table I).
The results indicated that the frequency distribution of demographic and clinical characteristics among the studied samples, including maternal age, placental location, methods of labor induction, fetal position during delivery, gestational age, fetal weight, and the duration of labor and induction, did not show statistically significant differences between the 2 groups of mothers who underwent vaginal delivery and those who had cesarean sections. However, a statistically significant difference was observed in the average CL and the measurements of posterior and anterior CAs between the 2 groups. Specifically, the length and anterior angle of the cervix were significantly smaller in mothers who experienced vaginal delivery compared to those who underwent cesarean sections, while the posterior angle measurement was notably greater in this group (Table II).
In the analysis of diagnostic parameters related to successful labor delivery, both univariate and multivariate regression models were employed to assess the influence of CL and CAs. The unadjusted model indicated that CL was positively associated with a cesarean section with an OR of 1.59, indicating that an increase of each millimeter of CL may increase the 59% likelihood of cesarean section; while the posterior CA showed a negative association, suggesting that an increase in this angle may decrease the 32% likelihood of cesarean section occurrence.
Conversely, the anterior CA demonstrated a positive correlation with the occurrence of cesarean section, with an OR of 1.48, indicating that an increase of each degree of anterior CA may increase the likelihood of cesarean section by 48%. In the adjusted model, CL maintained a positive association, although it was not statistically significant. The posterior CA did not show a significant relationship in this model, while the anterior CA continued to indicate a positive association without statistical significance (Table III).
The diagnostic accuracy of CL and CA in predicting labor outcomes can be summarized as follows: for CL, when measured at a cutoff of 28.55 mm, demonstrated a moderate ability to distinguish between successful and unsuccessful labor outcomes, with high sensitivity and NPV, but only fair specificity. In comparison, assessing the posterior CA at its optimal cutoff of 102.1° provided strong sensitivity and NPV, although its specificity was lower. The anterior CA performed at a cutoff of 85.15°, achieving high specificity and predictive value, but with limited sensitivity (Table IV and Figure 2).
4. Discussion
In this study, the assessment of CL and angles demonstrated significant relationships with labor outcomes. Specifically, CL and the anterior CA showed a direct significant correlation, while the posterior CA exhibited a significant inverse correlation with the likelihood of cesarean sections. The diagnostic accuracy metrics reveal that CL possesses moderate predictive capability for labor outcomes. The posterior demonstrated high sensitivity whereas the anterior CA had high specificity but lower sensitivity levels.
In this study, a cutoff value of 28.55 mm for CL was identified as a significant predictor of labor outcomes. The analysis revealed an accuracy of 58.3%, with a sensitivity of 100.0% and a specificity of 52.9%.
These metrics suggest that while the cutoff is relatively effective in identifying those at risk of cesarean section, it may also yield a considerable number of false positives. Similar to our study, a previous study indicated that a CL of 21 mm has shown 72.2% sensitivity and 79.1% specificity for cesarean delivery, while a CL of 22 mm indicated 66.6% sensitivity for labor induction (11). Also, in line with our study, a systematic review indicated that CL has moderate effectiveness in predicting successful IOL with pooled sensitivity and specificity of 67% and 70%, respectively (8). A diagnostic study demonstrated that CL yielded a sensitivity of 91.84% and a specificity of 80.95% in predicting the success of labor induction (12). A meta-analysis study revealed a significant association between CL and the prediction of successful labor induction, indicating that it is a strong predictor of labor outcomes (13). Overall, while the current study's findings contribute valuable insights into the predictive capabilities of CL, the moderate accuracy and specificity indicate that further research is needed to refine these metrics and enhance their clinical applicability in predicting labor outcomes effectively.
In this study, the posterior CA was evaluated as a predictor of labor outcomes, with a cutoff value established at 102.15°. The analysis revealed an AUC of 0.743, indicating moderate discriminative ability. Furthermore, the posterior CA demonstrated an accuracy of 51%, alongside a sensitivity of 90.91% and a specificity of 45.88%.
These metrics suggest that while the cutoff is relatively effective in identifying those at risk of cesarean section, it may also yield a considerable number of false positives.
In a study, the sensitivity and specificity of 91.84 and 90.48, at a cut-point of 99.5° in predicting labor induction success was reported for posterior CA, and they stated that posterior CA has been identified as a reliable measure for predicting successful IOL, with higher sensitivity compared to CL alone (12). A study found that the area under the ROC curve for predicting vaginal delivery based on the posterior CA was 0.667, with a cutoff value of 96.5°, and this predicting value was significant (14). In a study, the authors stated that measuring the CL and posterior CA offers a more objective and accurate prediction of successful labor induction than the Bishop score, owing to the strong correlation between successful induction and the posterior CA (15). Overall, while the posterior CA shows a promising outcome as a predictive tool, its limitations in sensitivity warrant further investigation to enhance its clinical applicability and ensure comprehensive risk assessment for labor outcomes.
In this study, a cutoff of 85.15° of anterior CA (uterocervical) showed an accuracy of 92.7%, a sensitivity of 36.4%, and a specificity of 100% in predicting cesarean section. In a study, the authors found that a utero CA ≥ 98.86° predicts preterm birth with 91% sensitivity and 75.5% specificity, outperforming CL in this context (16). Overall, while the high specificity of the current study's results is notable, the low sensitivity indicates that while the anterior CA can reliably rule out cesarean delivery when it exceeds the cutoff, it may not effectively predict successful vaginal deliveries, suggesting a need for further investigation into supplementary predictive measures or combined approaches for improved clinical outcomes.
In conclusion, while cervical measurements are valuable in predicting labor outcomes, their effectiveness can vary significantly based on specific contextual factors, including the timing of assessment, the gestational age of the patient, and the unique characteristics of the population being studied. For instance, CL measurements may be more predictive in certain stages of pregnancy or among populations with specific risk factors for preterm labor. Additionally, variations in measurement techniques and the clinician's experience can influence the reliability of these assessments. To enhance predictive accuracy, further research could explore the integration of cervical measures with other clinical indicators, such as maternal demographics, obstetric history, and real-time fetal monitoring data. This multifaceted approach could lead to the development of more comprehensive models that not only improve prediction rates for labor outcomes but also facilitate personalized care strategies tailored to individual patient profiles. By combining cervical assessments with additional clinical parameters, healthcare providers may be better equipped to make informed decisions regarding labor management and intervention strategies, ultimately improving maternal and neonatal outcomes.
4.1. Strengths and Limitations
This study has several limitations; firstly, the sample size of 100 participants may limit the generalizability of the findings, as a larger cohort could provide more robust data and enhance statistical power. Secondly, the study's exclusion criteria, which omitted women with certain complications such as fetal anomalies and pre-labor bleeding, may introduce selection bias, potentially affecting the applicability of the results to broader populations. Additionally, inaccuracies inherent in angle measurements via ultrasound, such as operator dependency, varying fetal and maternal positioning, and equipment limitations, could affect the precision and reliability of the CAs assessments, potentially impacting the diagnostic efficacy reported. Furthermore, the study's observational design does not allow for causal inferences regarding the relationship between cervical metrics and labor outcomes, limiting the ability to definitively establish predictive cutoffs for cesarean section risk. Finally, a significant limitation of this study is the considerable class imbalance, with only 15 out of 100 participants undergoing cesarean sections (of these 15 cases, 4 underwent cesarean section due to fetal distress or meconium-stained amniotic fluid and were not included in the study analysis). This uneven distribution may bias predictive metrics and analytical results, as classification models and statistical analyses often favor the majority group and may inadequately capture the characteristics or predictive factors of the minority class. These factors should be considered when interpreting the results and warrant further validation with larger samples and standardized measurement protocols.
5. Conclusion
The study’s findings indicate that CL and CA measurements exhibit meaningful yet heterogeneous associations with cesarean delivery risk, suggesting that these ultrasound-derived parameters may contribute to a more nuanced understanding of labor progression. While the observed patterns highlight the potential predictive value of these metrics, particularly the differential sensitivity and specificity demonstrated across CL, posterior CA, and anterior CA, they also underscore important methodological constraints. The limited sample size and the inherent variability in CA measurement techniques introduce uncertainty that warrants cautious interpretation. To establish the clinical reliability and applicability of these parameters, future research should prioritize larger, well‑designed studies employing standardized measurement protocols and rigorous analytical approaches, thereby enabling a more definitive assessment of the role of cervical metrics in labor management and cesarean risk stratification.
Data Availability
The data collected for this study are available upon reasonable request to the corresponding author.
Author Contributions
All authors met the 4 criteria for authorship contribution based on recommendations of the International Committee of Medical Journal Editors. S. Khazardoust: Conceptualization, data curation, writing (review and editing of original draft), supervision. Z. Zamanpour: Visualization, investigation, writing (review and editing of original draft). M. Aliasgharpoor: Conceptualization, methodology, formal analysis, writing (review and editing of original draft). M.A. Shafaat: Conceptualization, data curation, writing (review and editing of original draft). Z. Hamidi Madani: Conceptualization, data curation, project management, writing (review and editing of original draft). M. Ghalandari: Conceptualization, validation, writing (review and editing of original draft).
Acknowledgments
We extend our heartfelt appreciation to the participants, medical personnel, and administrative staff at Imam Khomeini hospital, Tehran, Iran for their exceptional support and collaboration throughout this study. Their commitment and cooperation were instrumental in facilitating our research, and we are truly grateful for their invaluable contributions. Tehran University of Medical Sciences, Tehran, Iran, financially supported this study (grant number: 71457). During the preparation of this work, the authors utilized artificial intelligence (Perplexity.ai) to refine grammar points and language style in writing. Subsequently, the authors thoroughly reviewed and edited the content as necessary, taking full responsibility for the publication’s content.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Physiology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
