
International Journal of
Reproductive Biomedicine
Sun, Jul 26, 2026
[Archive]
Volume 24, Issue 3 (March 2026)
IJRM 2026, 24(3): 209-218 |
Back to browse issues page


Ethics code: IR.SBMU.RETECH.REC.1404.033
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseini S, Salehpour S, Amiresmaili N, Meshkat M, Karimi F. Serum anti-Müllerian hormone and ovarian stimulation parameters in women with polycystic ovary syndrome undergoing assisted reproductive technology: A cross-sectional study. IJRM 2026; 24 (3) :209-218
URL: http://ijrm.ir/article-1-3650-en.html
URL: http://ijrm.ir/article-1-3650-en.html



1- Preventative Gynecology Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Reproductive Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
3- Preventative Gynecology Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,dr.karimi@sbmu.ac.ir
2- Department of Reproductive Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
3- Preventative Gynecology Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. ,
Keywords: Anti-Mullerian hormone, Polycystic ovary syndrome, In vitro fertilization, Oocytes, Assisted reproductive techniques.
Full-Text [PDF 574 kb]
(277 Downloads)
| Abstract (HTML) (353 Views)
Full-Text: (31 Views)
1. Introduction
Polycystic ovary syndrome (PCOS) is among the most common endocrine disorders affecting women of reproductive age, with a global prevalence estimated at 8-15% depending on diagnostic criteria (1). It is a leading cause of anovulatory infertility and is characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. A hallmark of PCOS is the accumulation of small antral follicles, which contributes to elevated serum levels of anti-Müllerian hormone (AMH) (2).
AMH is a glycoprotein produced by granulosa cells of pre-antral and small antral follicles. It serves as an indicator of ovarian reserve, representing the pool of follicles that can be recruited (3). In PCOS, AMH levels are typically 2-4 times higher than in women with regular menstrual cycles because of an increased follicle count rather than follicle quality (4). Consequently, AMH has been widely adopted in assisted reproductive technology (ART) protocols for predicting ovarian response. Research indicates an association between AMH levels and oocyte yield during controlled ovarian stimulation, especially among participants with PCOS (5). The ability of AMH to predict oocyte maturity, embryo quality, implantation, and live birth has not been definitively established. Some studies report that high AMH levels improve ART outcomes (6), while others suggest that supraphysiological levels may impair folliculogenesis and embryo development due to follicular arrest or dysregulated hormonal environment (7).
A growing body of evidence suggests that the relationship between AMH and ART outcomes in PCOS may follow a nonlinear, inverted-U pattern, where optimal results are seen at intermediate AMH levels (8). For instance, Mohammed and Haddad reported that women with AMH levels between 1.6 and 4.0 ng/mL achieved the highest clinical pregnancy rates in a PCOS cohort (9). In contrast, Liu et al. found no significant differences in pregnancy outcomes across AMH quartiles, suggesting that this biomarker may not have predictive value for final reproductive success (10). Given the inconsistent literature, further clarification is required regarding the role of AMH in guiding ART treatment strategies for women with PCOS. The present study aimed to evaluate the relationship between AMH and a broad range of ART outcomes, including gonadotropin dose, stimulation duration, oocyte yield and maturity, and embryo formation, in a real-world cohort of women with PCOS. We sought to investigate both linear and nonlinear associations and determine whether mid-range AMH levels are associated with better outcomes in this population.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study included 204 women aged 20-45 yr diagnosed with PCOS who underwent in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI) cycles at Taleghani hospital, Tehran, Iran between March 2023 and March 2025.
Clinical records were reviewed using a census sampling method. Data extraction was performed retrospectively by 2 independent researchers using a structured checklist. After excluding 32 cases due to incomplete key records or meeting exclusion criteria, 172 participants were finally analyzed.
2.2. Eligibility criteria
Inclusion criteria were: age between 20 and 45 yr; a diagnosis of PCOS based on the Rotterdam criteria (presence of at least 2 of the following: oligo- or anovulation, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology); having undergone controlled ovarian stimulation followed by IVF or ICSI during the study period; and availability of complete clinical records (11). Required records included serum AMH levels, total gonadotropin dose administered, number of stimulation days, oocyte retrieval details (including oocyte subtypes), and embryo development outcomes.
Participants were excluded from the study if they presented with severe male factor infertility, such as azoospermia, had a history of recurrent implantation failure, were diagnosed with endometriosis, or had incomplete or missing medical records.
2.3. Variables and outcome measures
All data were manually collected from paper-based clinical files and embryology laboratory reports archived at the hospital. A structured data abstraction form and standardized checklist were used by 2 trained investigators who independently extracted all required variables. Any discrepancies were resolved through discussion, and a random 10% of records were reassessed for quality control. Serum AMH levels were obtained from the most recent measurement within 3 months before the ART cycle. Gonadotropin dose, stimulation duration, number and type of retrieved oocytes )metaphase II [MII], metaphase I [MI], and germinal vesicle(, and number of embryos formed were extracted from clinical and embryology records. Embryo grading was not evaluated in this study. Maternal age and body mass index (BMI), measured at the initial clinic visit, were included as additional variables. For analytical purposes, AMH levels were categorized into 3 clinically meaningful groups: low (< 2.5 ng/mL), mid-range (2.5-6.5 ng/mL), and high (> 6.5 ng/mL). All data were entered into a pre-coded spreadsheet prior to statistical analysis.
2.4. Ethical Considerations
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.RETECH.REC.1404.033) and conducted by institutional and national ethical standards. Data were anonymized prior to analysis, with confidentiality maintained by removing identifiers and limiting access to the research team. The data were solely used for research purposes.
2.5. Statistical Analysis
Statistical analyses were performed using Statistical Package for the Social Sciences version 17.0 (Statistical Package for the Social Sciences Inc., Chicago, IL, USA). Normality of continuous variables was assessed using the Shapiro-Wilk test. Numerical variables were summarized as mean ± standard deviation or median (interquartile range), and categorical variables as frequencies and percentages. The association between serum AMH and ART outcomes was evaluated using Spearman’s rank correlation. Group comparisons across AMH categories were performed with the Kruskal-Wallis test. Multivariate linear regression was applied to assess independent relationships after adjusting for age and BMI. A p < 0.05 was considered statistically significant.
3. Results
3.1. Participants
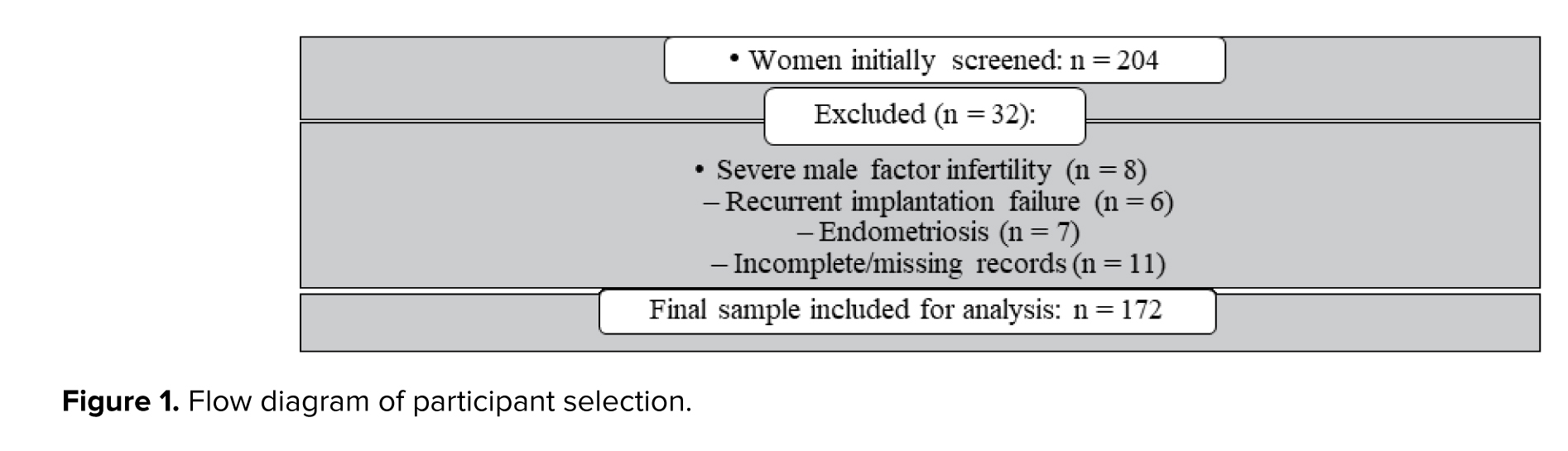
During the study period, 204 women with PCOS undergoing ART cycles were screened for eligibility. A total of 32 women were excluded because of incomplete key data or meeting exclusion criteria (severe male factor infertility, recurrent implantation failure, or endometriosis). Finally, 172 participants were included in the analysis (Figure 1).
3.2. Baseline data
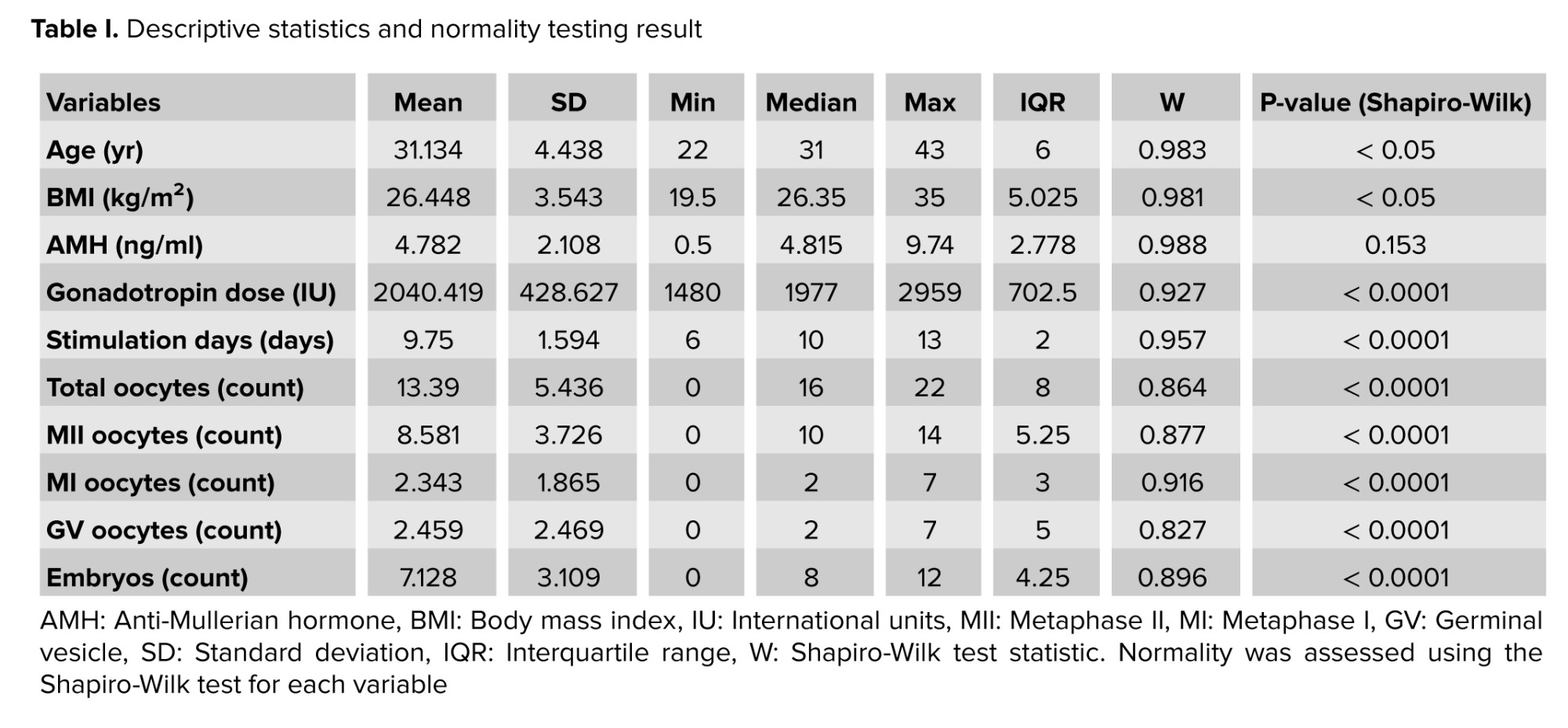
Baseline demographic and clinical characteristics of the participants are presented in table I. The mean age was approximately 31 yr, the mean BMI was in the overweight range, and a wide distribution of AMH values and ovarian response parameters was observed. Shapiro-Wilk testing indicated that most variables were not normally distributed.
3.3. Descriptive data
Stimulation characteristics and laboratory findings, including gonadotropin dose, stimulation days, total oocytes, MII oocytes, and embryo count, are summarized in table I. All variables are shown with their respective means, standard deviations, medians, ranges, and normality test results.
3.4. Outcome data
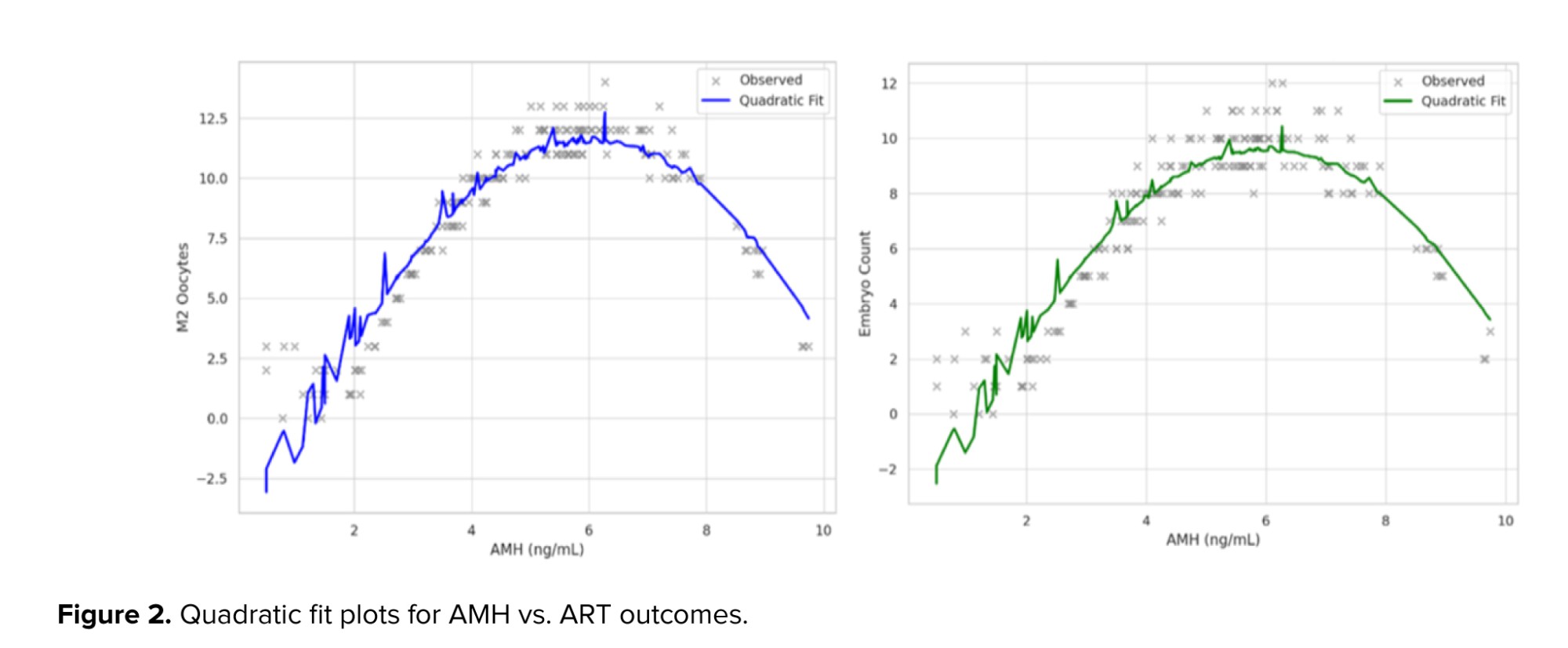
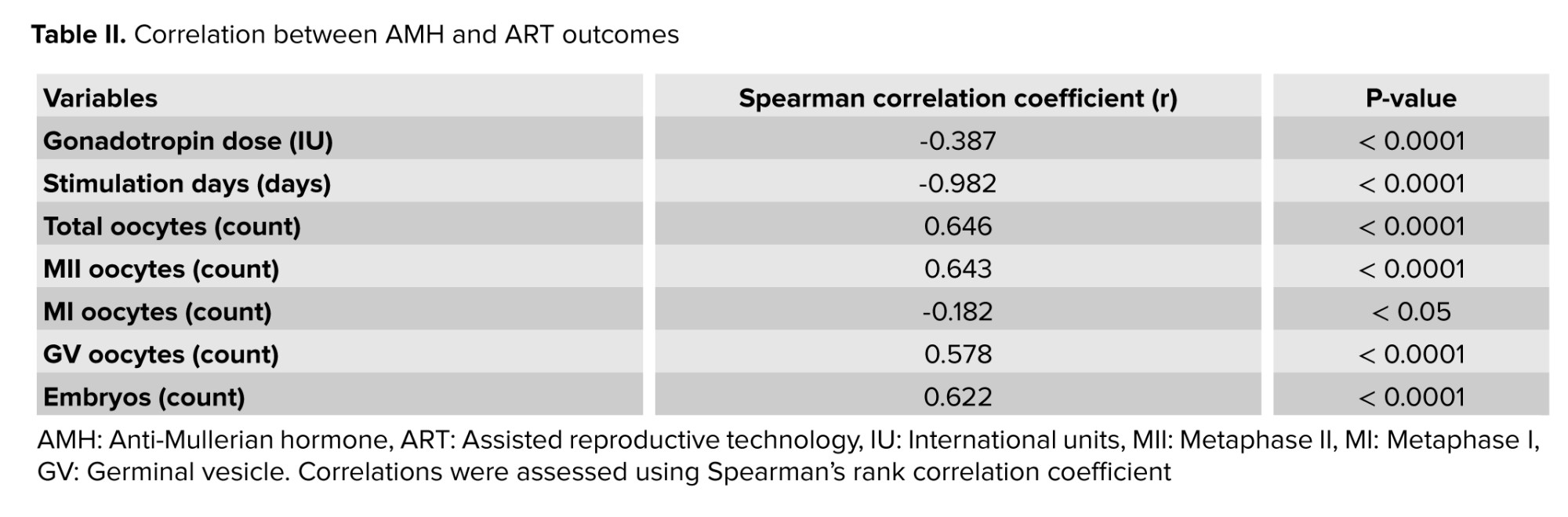
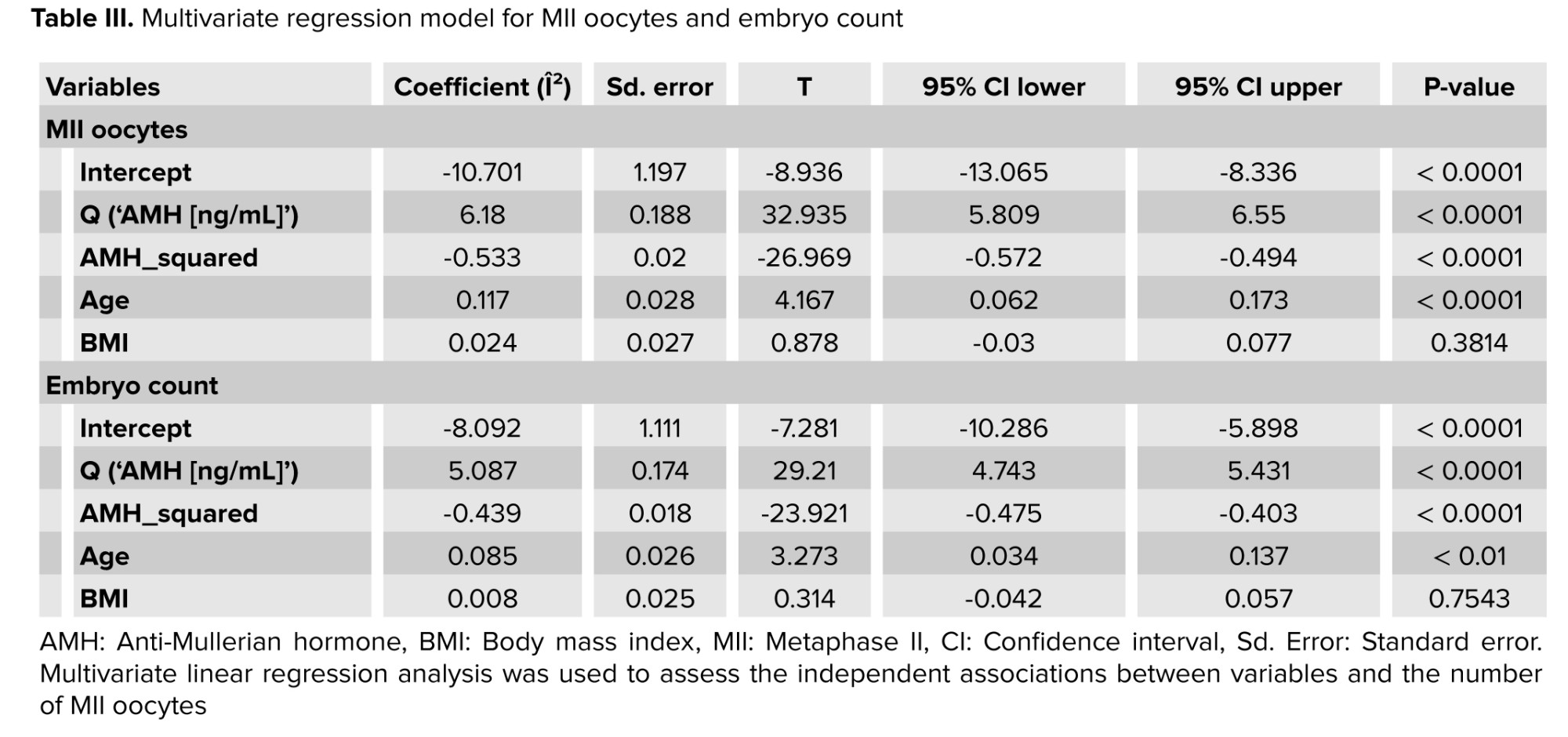
Correlation analyses between AMH and ART outcomes are shown in table II. Higher AMH levels were moderately associated with lower gonadotropin dose and fewer stimulation days, and positively associated with total oocyte count, MII oocytes, and embryo formation. Multivariable regression analyses (Table III) confirmed a significant nonlinear association between AMH and both MII oocytes and embryo count after adjustment for age and BMI. Quadratic AMH terms indicated an inverted-U pattern, with peak response at mid-range AMH levels. Predicted fitted curves are displayed in figure 2.
3.5. Main results
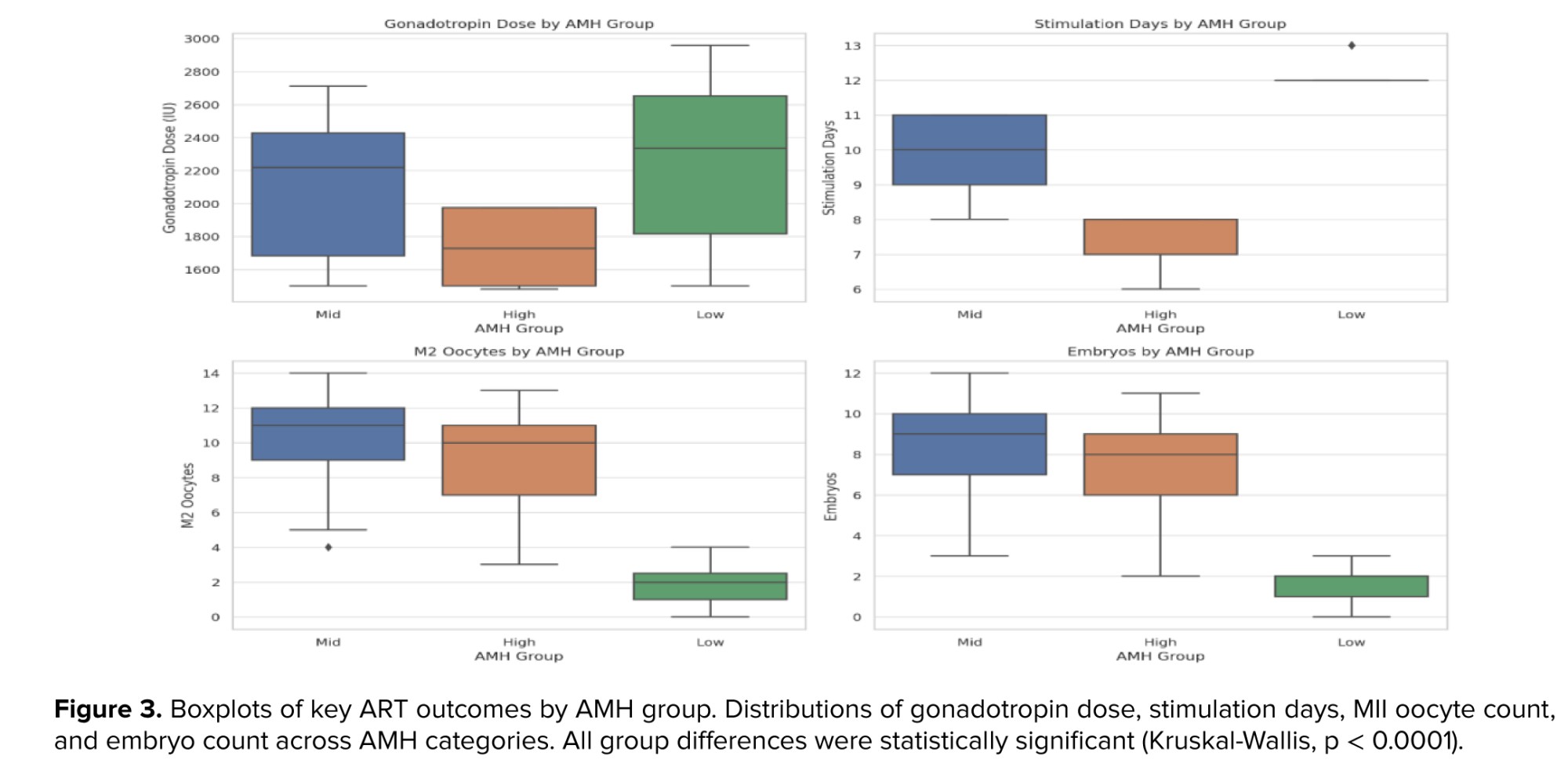
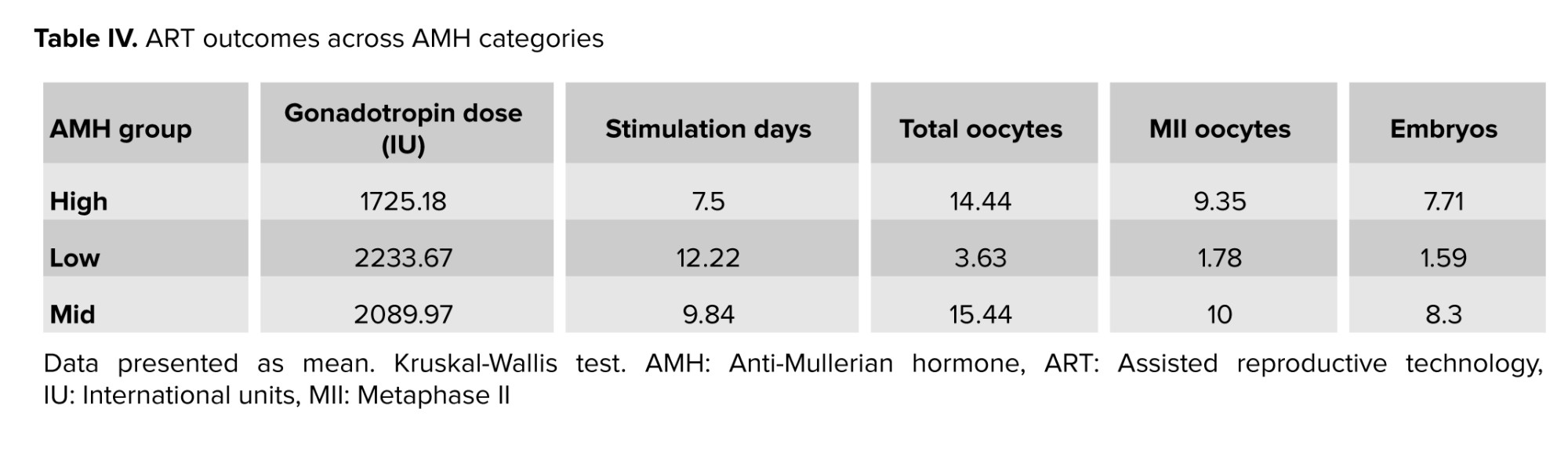
Comparisons across AMH categories (low < 2.5, mid 2.5-6.5, high > 6.5 ng/mL) demonstrated significant differences in stimulation burden and ovarian response (Table IV). Women in the mid-AMH group achieved the best overall outcomes, with the highest mean MII oocytes and embryos while maintaining moderate gonadotropin requirements. The low-AMH group required the most gonadotropin and had the poorest response, whereas the high-AMH group responded quickly but did not exceed the mid group in embryo yield. Distributions across groups are visualized in figure 3.
3.6. Other analyses
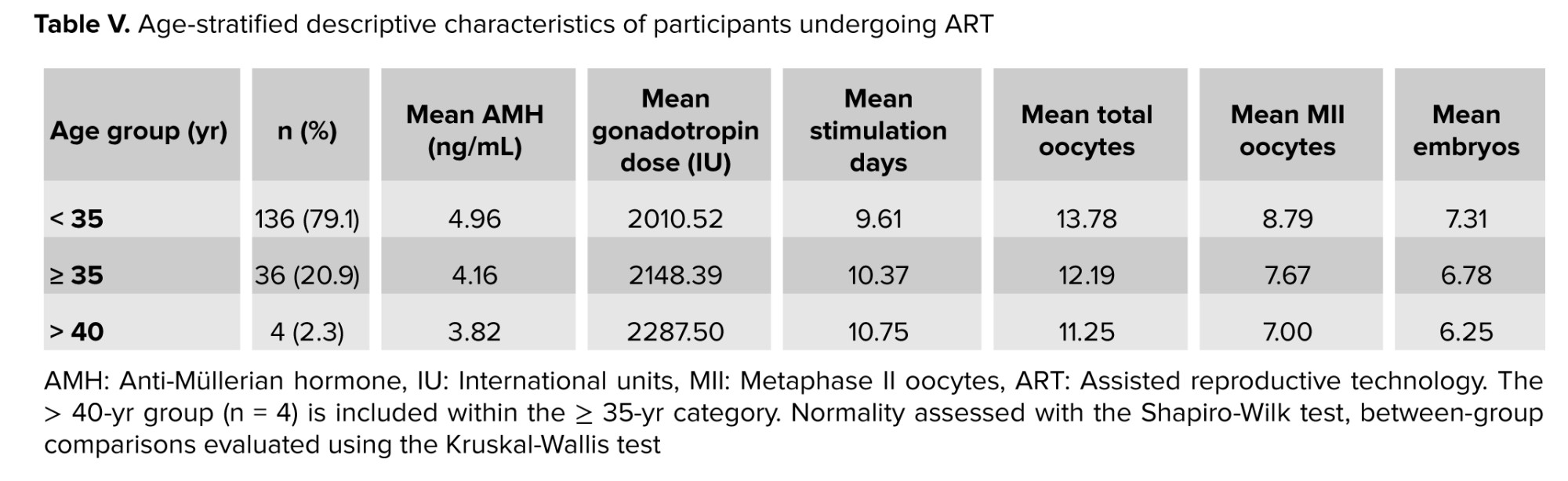
Age-stratified descriptive analysis showed similar AMH-outcome patterns among women < 35 yr and ≥ 35 yr. Detailed subgroup values are presented in table V. Because the ≥ 40 yr subset was very small (n = 4), no inferential subgroup testing was performed.
4. Discussion
In this study, serum AMH showed a significant yet nonlinear relationship with ovarian stimulation outcomes in women with PCOS undergoing ART. The most favorable responses, defined by higher numbers of mature oocytes and embryos, along with moderate gonadotropin requirements, were observed in participants with AMH levels between 2.5 and 6.5 ng/mL, suggesting that this range may represent the optimal biological window for ovarian stimulation in this population.
Recent reviews and meta-analyses have highlighted that AMH in PCOS patients indicates a complex and non-linear biological relationship rather than a straightforward dose-response pattern (12). Elevated AMH levels are consistently linked to a higher oocyte yield but reduced embryo quality and lower fertilization rates, highlighting a discrepancy between follicular quantity and competence (13). Furthermore, studies suggest that extreme AMH levels, either very low or very high, are associated with subpar laboratory results and less successful ART responses (14). This supports that an intermediate AMH range may indicate optimal follicular development.
Evidence also suggests that AMH primarily serves as a marker of ovarian responsiveness rather than a predictor of embryo viability or implantation potential (15). The quadratic trend in our data reflects that low AMH levels predict weaker results, requiring longer stimulation and higher gonadotropins. High levels, though linked to rapid response, may produce oocytes with reduced potential due to follicular asynchrony (16). These findings, aligned with previous research, show that excessive granulosa cell activity and altered intra-ovarian hormones can impair folliculogenesis (17).
Similarly, studies evaluating IVF outcomes in PCOS have shown that women with mid-range AMH levels achieve higher fertilization and cleavage rates compared with those at the extremes (18). Conversely, excessively high AMH levels may indicate a hyper-responsive ovarian environment prone to producing many immature or poor-quality oocytes, ultimately leading to fewer viable embryos (19). Recent literature supports that AMH is a threshold-dependent predictor of ovarian response.
Our data refine understanding of AMH as a biomarker for personalized stimulation, with inverse correlations between AMH and both gonadotropin dose and stimulation duration. This suggests AMH can help calibrate medication to prevent over- or under-stimulation. Prior research shows that women with moderate AMH levels achieve an adequate oocyte yield with balanced gonadotropins, while those with lower AMH levels require higher doses for sufficient follicular recruitment (1). In contrast, reducing the gonadotropin dosage in women with high AMH may lower the risk of ovarian hyperstimulation without compromising oocyte maturity (2).
Multiple independent studies have demonstrated the clinical utility of AMH as a marker of ovarian sensitivity, underscoring its value as a reliable biochemical indicator for customizing ART protocols (3). However, it is increasingly clear that AMH alone cannot predict pregnancy or live birth outcomes. Instead, it should be integrated with complementary factors such as age, BMI, antral follicle count, and baseline gonadotropin levels to enhance predictive accuracy (4). The combination of these markers offers a more comprehensive view of ovarian physiology and responsiveness during stimulation. Our findings also support that AMH variability in PCOS mainly results from differences in small antral follicle count and granulosa-cell function, not true ovarian reserve variations (5). This explains why very high AMH levels often fail to correspond with improved embryo development or higher clinical success rates. Furthermore, elevated AMH may signify a hormonal milieu that promotes follicular overcrowding and dysregulated selection, ultimately reducing oocyte competence (6). Genetic studies have revealed that polymorphisms in AMH or AMH receptor signaling pathways can further contribute to this interindividual variability, underscoring the need to interpret serum levels within a broader biological and clinical context (7).
The nonlinear association identified in the present study may thus represent the net outcome of these multifactorial processes. Women with mid-range AMH appear to maintain an optimal equilibrium between follicular recruitment and endocrine feedback, facilitating coordinated folliculogenesis and higher-quality oocytes (8). Conversely, very high AMH levels might reflect a state of impaired follicular selection, while very low levels indicate diminished responsiveness. Hence, rather than viewing AMH as a linear marker of ovarian reserve, it should be considered a dynamic biomarker reflecting both the quantity and regulatory balance of growing follicles (9).
From a clinical standpoint, integration of AMH into stimulation algorithms holds considerable potential for improving treatment personalization. The ovarian sensitivity index and AMH-derived nomograms have already demonstrated value in optimizing gonadotropin dosing and reducing iatrogenic risks such as ovarian hyperstimulation syndrome (10).
Our study demonstrates that AMH's ability to pinpoint the “optimal zone” of response supports refining predictive tools specifically for PCOS populations. Key strengths include a uniform group of PCOS patients treated with standardized antagonist protocols, exclusion of major confounding factors like severe male-factor infertility and endometriosis, and the use of nonlinear modeling to reveal complex biological interactions. The consistency of the pattern across age groups further enhances the internal validity. However, the limited number of participants over 40 restricted subgroup analyses, and the retrospective design means causality cannot be confirmed. Additional limitations include the lack of embryo grading and pregnancy outcome data, restricting interpretation to laboratory endpoints. AMH levels were measured using a single assay platform, reducing variability within the study but limiting external comparison. Although the sample size was adequate for correlation analyses, the single-center scope limits the broader applicability of the findings.
Future multicenter studies with larger, more ethnically diverse PCOS groups are necessary to confirm these results. Long-term follow-up during implantation, clinical pregnancy, and live birth stages will clarify whether the nonlinear trend observed in laboratory settings correlates with reproductive outcomes. Additionally, standardizing AMH assays and establishing population-specific cut-off values are crucial for reliable clinical interpretation. Combining AMH with other markers such as luteinizing hormone, antral follicle count, and the ovarian sensitivity index in predictive models or nomograms could further improve the accuracy and safety of personalized ART treatments.
5. Conclusion
This study demonstrates that serum AMH is a strong, yet nonlinear, predictor of ART response in women with PCOS. While elevated AMH levels are generally linked to increased oocyte yield, our analysis shows that mid-range AMH values (2.5-6.5 ng/mL) provide the most favorable outcomes in terms of both MII oocyte maturity and embryo formation. Participants with low AMH required more intensive stimulation and exhibited the poorest response. Conversely, participants with very high AMH levels responded more quickly but did not have better embryo outcomes, supporting a threshold-sensitive, inverted-U relationship between AMH and ART effectiveness.
These findings emphasize that using AMH levels for stratification can improve ovarian stimulation, enhance treatment effectiveness, and avoid overly aggressive stimulation. Nonetheless, relying solely on AMH to forecast embryo quality or long-term reproductive success is insufficient without accounting for other participant-specific factors.
Further prospective studies with standardized AMH assays and live birth data are essential to define universal cut-off values and optimize ART outcomes in PCOS participants.
Data Availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
S. Hosseini: Contributed to the conception and design of the study, acquisition and interpretation of data, and critically revised the manuscript for important intellectual content. S. Salehpour: Assisted in study design, supervised the research process, contributed to data analysis and interpretation, and revised the manuscript. N. Amiresmaili: Participated in statistical analysis, interpretation of results, and manuscript drafting. Provided critical revision and approved the final version. M. Meshkat: Assisted with data collection, literature review, and initial drafting of the manuscript. Approved the final version and agrees to be accountable for all aspects of the work. F. Karimi: Led the conception and design of the study, coordinated data acquisition, performed data analysis and interpretation, drafted and revised the manuscript, and managed all correspondence. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the Taleghani hospital, IVF Center, Tehran, Iran staff for their cooperation and the biostatistics consultant for reviewing analyses. The study received no funding. The authors declare that no artificial intelligence tools were used in the design, data analysis, translation, or revision of this manuscript. All writing and editing were performed by the authors themselves.
Conflict of Interest
The authors declare that there is no conflict of interest.
Polycystic ovary syndrome (PCOS) is among the most common endocrine disorders affecting women of reproductive age, with a global prevalence estimated at 8-15% depending on diagnostic criteria (1). It is a leading cause of anovulatory infertility and is characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. A hallmark of PCOS is the accumulation of small antral follicles, which contributes to elevated serum levels of anti-Müllerian hormone (AMH) (2).
AMH is a glycoprotein produced by granulosa cells of pre-antral and small antral follicles. It serves as an indicator of ovarian reserve, representing the pool of follicles that can be recruited (3). In PCOS, AMH levels are typically 2-4 times higher than in women with regular menstrual cycles because of an increased follicle count rather than follicle quality (4). Consequently, AMH has been widely adopted in assisted reproductive technology (ART) protocols for predicting ovarian response. Research indicates an association between AMH levels and oocyte yield during controlled ovarian stimulation, especially among participants with PCOS (5). The ability of AMH to predict oocyte maturity, embryo quality, implantation, and live birth has not been definitively established. Some studies report that high AMH levels improve ART outcomes (6), while others suggest that supraphysiological levels may impair folliculogenesis and embryo development due to follicular arrest or dysregulated hormonal environment (7).
A growing body of evidence suggests that the relationship between AMH and ART outcomes in PCOS may follow a nonlinear, inverted-U pattern, where optimal results are seen at intermediate AMH levels (8). For instance, Mohammed and Haddad reported that women with AMH levels between 1.6 and 4.0 ng/mL achieved the highest clinical pregnancy rates in a PCOS cohort (9). In contrast, Liu et al. found no significant differences in pregnancy outcomes across AMH quartiles, suggesting that this biomarker may not have predictive value for final reproductive success (10). Given the inconsistent literature, further clarification is required regarding the role of AMH in guiding ART treatment strategies for women with PCOS. The present study aimed to evaluate the relationship between AMH and a broad range of ART outcomes, including gonadotropin dose, stimulation duration, oocyte yield and maturity, and embryo formation, in a real-world cohort of women with PCOS. We sought to investigate both linear and nonlinear associations and determine whether mid-range AMH levels are associated with better outcomes in this population.
2. Materials and Methods
2.1. Study design and participants
This cross-sectional study included 204 women aged 20-45 yr diagnosed with PCOS who underwent in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI) cycles at Taleghani hospital, Tehran, Iran between March 2023 and March 2025.
Clinical records were reviewed using a census sampling method. Data extraction was performed retrospectively by 2 independent researchers using a structured checklist. After excluding 32 cases due to incomplete key records or meeting exclusion criteria, 172 participants were finally analyzed.
2.2. Eligibility criteria
Inclusion criteria were: age between 20 and 45 yr; a diagnosis of PCOS based on the Rotterdam criteria (presence of at least 2 of the following: oligo- or anovulation, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology); having undergone controlled ovarian stimulation followed by IVF or ICSI during the study period; and availability of complete clinical records (11). Required records included serum AMH levels, total gonadotropin dose administered, number of stimulation days, oocyte retrieval details (including oocyte subtypes), and embryo development outcomes.
Participants were excluded from the study if they presented with severe male factor infertility, such as azoospermia, had a history of recurrent implantation failure, were diagnosed with endometriosis, or had incomplete or missing medical records.
2.3. Variables and outcome measures
All data were manually collected from paper-based clinical files and embryology laboratory reports archived at the hospital. A structured data abstraction form and standardized checklist were used by 2 trained investigators who independently extracted all required variables. Any discrepancies were resolved through discussion, and a random 10% of records were reassessed for quality control. Serum AMH levels were obtained from the most recent measurement within 3 months before the ART cycle. Gonadotropin dose, stimulation duration, number and type of retrieved oocytes )metaphase II [MII], metaphase I [MI], and germinal vesicle(, and number of embryos formed were extracted from clinical and embryology records. Embryo grading was not evaluated in this study. Maternal age and body mass index (BMI), measured at the initial clinic visit, were included as additional variables. For analytical purposes, AMH levels were categorized into 3 clinically meaningful groups: low (< 2.5 ng/mL), mid-range (2.5-6.5 ng/mL), and high (> 6.5 ng/mL). All data were entered into a pre-coded spreadsheet prior to statistical analysis.
2.4. Ethical Considerations
This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBMU.RETECH.REC.1404.033) and conducted by institutional and national ethical standards. Data were anonymized prior to analysis, with confidentiality maintained by removing identifiers and limiting access to the research team. The data were solely used for research purposes.
2.5. Statistical Analysis
Statistical analyses were performed using Statistical Package for the Social Sciences version 17.0 (Statistical Package for the Social Sciences Inc., Chicago, IL, USA). Normality of continuous variables was assessed using the Shapiro-Wilk test. Numerical variables were summarized as mean ± standard deviation or median (interquartile range), and categorical variables as frequencies and percentages. The association between serum AMH and ART outcomes was evaluated using Spearman’s rank correlation. Group comparisons across AMH categories were performed with the Kruskal-Wallis test. Multivariate linear regression was applied to assess independent relationships after adjusting for age and BMI. A p < 0.05 was considered statistically significant.
3. Results
3.1. Participants
During the study period, 204 women with PCOS undergoing ART cycles were screened for eligibility. A total of 32 women were excluded because of incomplete key data or meeting exclusion criteria (severe male factor infertility, recurrent implantation failure, or endometriosis). Finally, 172 participants were included in the analysis (Figure 1).
3.2. Baseline data
Baseline demographic and clinical characteristics of the participants are presented in table I. The mean age was approximately 31 yr, the mean BMI was in the overweight range, and a wide distribution of AMH values and ovarian response parameters was observed. Shapiro-Wilk testing indicated that most variables were not normally distributed.
3.3. Descriptive data
Stimulation characteristics and laboratory findings, including gonadotropin dose, stimulation days, total oocytes, MII oocytes, and embryo count, are summarized in table I. All variables are shown with their respective means, standard deviations, medians, ranges, and normality test results.
3.4. Outcome data
Correlation analyses between AMH and ART outcomes are shown in table II. Higher AMH levels were moderately associated with lower gonadotropin dose and fewer stimulation days, and positively associated with total oocyte count, MII oocytes, and embryo formation. Multivariable regression analyses (Table III) confirmed a significant nonlinear association between AMH and both MII oocytes and embryo count after adjustment for age and BMI. Quadratic AMH terms indicated an inverted-U pattern, with peak response at mid-range AMH levels. Predicted fitted curves are displayed in figure 2.
3.5. Main results
Comparisons across AMH categories (low < 2.5, mid 2.5-6.5, high > 6.5 ng/mL) demonstrated significant differences in stimulation burden and ovarian response (Table IV). Women in the mid-AMH group achieved the best overall outcomes, with the highest mean MII oocytes and embryos while maintaining moderate gonadotropin requirements. The low-AMH group required the most gonadotropin and had the poorest response, whereas the high-AMH group responded quickly but did not exceed the mid group in embryo yield. Distributions across groups are visualized in figure 3.
3.6. Other analyses
Age-stratified descriptive analysis showed similar AMH-outcome patterns among women < 35 yr and ≥ 35 yr. Detailed subgroup values are presented in table V. Because the ≥ 40 yr subset was very small (n = 4), no inferential subgroup testing was performed.
4. Discussion
In this study, serum AMH showed a significant yet nonlinear relationship with ovarian stimulation outcomes in women with PCOS undergoing ART. The most favorable responses, defined by higher numbers of mature oocytes and embryos, along with moderate gonadotropin requirements, were observed in participants with AMH levels between 2.5 and 6.5 ng/mL, suggesting that this range may represent the optimal biological window for ovarian stimulation in this population.
Recent reviews and meta-analyses have highlighted that AMH in PCOS patients indicates a complex and non-linear biological relationship rather than a straightforward dose-response pattern (12). Elevated AMH levels are consistently linked to a higher oocyte yield but reduced embryo quality and lower fertilization rates, highlighting a discrepancy between follicular quantity and competence (13). Furthermore, studies suggest that extreme AMH levels, either very low or very high, are associated with subpar laboratory results and less successful ART responses (14). This supports that an intermediate AMH range may indicate optimal follicular development.
Evidence also suggests that AMH primarily serves as a marker of ovarian responsiveness rather than a predictor of embryo viability or implantation potential (15). The quadratic trend in our data reflects that low AMH levels predict weaker results, requiring longer stimulation and higher gonadotropins. High levels, though linked to rapid response, may produce oocytes with reduced potential due to follicular asynchrony (16). These findings, aligned with previous research, show that excessive granulosa cell activity and altered intra-ovarian hormones can impair folliculogenesis (17).
Similarly, studies evaluating IVF outcomes in PCOS have shown that women with mid-range AMH levels achieve higher fertilization and cleavage rates compared with those at the extremes (18). Conversely, excessively high AMH levels may indicate a hyper-responsive ovarian environment prone to producing many immature or poor-quality oocytes, ultimately leading to fewer viable embryos (19). Recent literature supports that AMH is a threshold-dependent predictor of ovarian response.
Our data refine understanding of AMH as a biomarker for personalized stimulation, with inverse correlations between AMH and both gonadotropin dose and stimulation duration. This suggests AMH can help calibrate medication to prevent over- or under-stimulation. Prior research shows that women with moderate AMH levels achieve an adequate oocyte yield with balanced gonadotropins, while those with lower AMH levels require higher doses for sufficient follicular recruitment (1). In contrast, reducing the gonadotropin dosage in women with high AMH may lower the risk of ovarian hyperstimulation without compromising oocyte maturity (2).
Multiple independent studies have demonstrated the clinical utility of AMH as a marker of ovarian sensitivity, underscoring its value as a reliable biochemical indicator for customizing ART protocols (3). However, it is increasingly clear that AMH alone cannot predict pregnancy or live birth outcomes. Instead, it should be integrated with complementary factors such as age, BMI, antral follicle count, and baseline gonadotropin levels to enhance predictive accuracy (4). The combination of these markers offers a more comprehensive view of ovarian physiology and responsiveness during stimulation. Our findings also support that AMH variability in PCOS mainly results from differences in small antral follicle count and granulosa-cell function, not true ovarian reserve variations (5). This explains why very high AMH levels often fail to correspond with improved embryo development or higher clinical success rates. Furthermore, elevated AMH may signify a hormonal milieu that promotes follicular overcrowding and dysregulated selection, ultimately reducing oocyte competence (6). Genetic studies have revealed that polymorphisms in AMH or AMH receptor signaling pathways can further contribute to this interindividual variability, underscoring the need to interpret serum levels within a broader biological and clinical context (7).
The nonlinear association identified in the present study may thus represent the net outcome of these multifactorial processes. Women with mid-range AMH appear to maintain an optimal equilibrium between follicular recruitment and endocrine feedback, facilitating coordinated folliculogenesis and higher-quality oocytes (8). Conversely, very high AMH levels might reflect a state of impaired follicular selection, while very low levels indicate diminished responsiveness. Hence, rather than viewing AMH as a linear marker of ovarian reserve, it should be considered a dynamic biomarker reflecting both the quantity and regulatory balance of growing follicles (9).
From a clinical standpoint, integration of AMH into stimulation algorithms holds considerable potential for improving treatment personalization. The ovarian sensitivity index and AMH-derived nomograms have already demonstrated value in optimizing gonadotropin dosing and reducing iatrogenic risks such as ovarian hyperstimulation syndrome (10).
Our study demonstrates that AMH's ability to pinpoint the “optimal zone” of response supports refining predictive tools specifically for PCOS populations. Key strengths include a uniform group of PCOS patients treated with standardized antagonist protocols, exclusion of major confounding factors like severe male-factor infertility and endometriosis, and the use of nonlinear modeling to reveal complex biological interactions. The consistency of the pattern across age groups further enhances the internal validity. However, the limited number of participants over 40 restricted subgroup analyses, and the retrospective design means causality cannot be confirmed. Additional limitations include the lack of embryo grading and pregnancy outcome data, restricting interpretation to laboratory endpoints. AMH levels were measured using a single assay platform, reducing variability within the study but limiting external comparison. Although the sample size was adequate for correlation analyses, the single-center scope limits the broader applicability of the findings.
Future multicenter studies with larger, more ethnically diverse PCOS groups are necessary to confirm these results. Long-term follow-up during implantation, clinical pregnancy, and live birth stages will clarify whether the nonlinear trend observed in laboratory settings correlates with reproductive outcomes. Additionally, standardizing AMH assays and establishing population-specific cut-off values are crucial for reliable clinical interpretation. Combining AMH with other markers such as luteinizing hormone, antral follicle count, and the ovarian sensitivity index in predictive models or nomograms could further improve the accuracy and safety of personalized ART treatments.
5. Conclusion
This study demonstrates that serum AMH is a strong, yet nonlinear, predictor of ART response in women with PCOS. While elevated AMH levels are generally linked to increased oocyte yield, our analysis shows that mid-range AMH values (2.5-6.5 ng/mL) provide the most favorable outcomes in terms of both MII oocyte maturity and embryo formation. Participants with low AMH required more intensive stimulation and exhibited the poorest response. Conversely, participants with very high AMH levels responded more quickly but did not have better embryo outcomes, supporting a threshold-sensitive, inverted-U relationship between AMH and ART effectiveness.
These findings emphasize that using AMH levels for stratification can improve ovarian stimulation, enhance treatment effectiveness, and avoid overly aggressive stimulation. Nonetheless, relying solely on AMH to forecast embryo quality or long-term reproductive success is insufficient without accounting for other participant-specific factors.
Further prospective studies with standardized AMH assays and live birth data are essential to define universal cut-off values and optimize ART outcomes in PCOS participants.
Data Availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
S. Hosseini: Contributed to the conception and design of the study, acquisition and interpretation of data, and critically revised the manuscript for important intellectual content. S. Salehpour: Assisted in study design, supervised the research process, contributed to data analysis and interpretation, and revised the manuscript. N. Amiresmaili: Participated in statistical analysis, interpretation of results, and manuscript drafting. Provided critical revision and approved the final version. M. Meshkat: Assisted with data collection, literature review, and initial drafting of the manuscript. Approved the final version and agrees to be accountable for all aspects of the work. F. Karimi: Led the conception and design of the study, coordinated data acquisition, performed data analysis and interpretation, drafted and revised the manuscript, and managed all correspondence. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the Taleghani hospital, IVF Center, Tehran, Iran staff for their cooperation and the biostatistics consultant for reviewing analyses. The study received no funding. The authors declare that no artificial intelligence tools were used in the design, data analysis, translation, or revision of this manuscript. All writing and editing were performed by the authors themselves.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
