
International Journal of
Reproductive Biomedicine
Fri, Jun 12, 2026
[Archive]
Volume 24, Issue 2 (February 2026)
IJRM 2026, 24(2): 163-172 |
Back to browse issues page
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Modabber M, Parsapour A, Jafari M, Malbakhsh M, Shamsi Gooshki E. Ghost mothers: Ethical challenges in Iran as an emerging destination for cross-border surrogacy: A case report. IJRM 2026; 24 (2) :163-172
URL: http://ijrm.ir/article-1-3645-en.html
URL: http://ijrm.ir/article-1-3645-en.html
Maryam Modabber1 

 , Alireza Parsapour1 , Mohammadreza Jafari2 , Mahshid Malbakhsh2 , Ehsan Shamsi Gooshki *3
, Alireza Parsapour1 , Mohammadreza Jafari2 , Mahshid Malbakhsh2 , Ehsan Shamsi Gooshki *3
, Alireza Parsapour1 , Mohammadreza Jafari2 , Mahshid Malbakhsh2 , Ehsan Shamsi Gooshki *3
1- Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran. Iran.
2- Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
3- Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran. Iran. & Monash Bioethics Center, Monash University, Melbourne, Australia. ,Ehsan.shamsigooshki@monash.edu
2- Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
3- Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran. Iran. & Monash Bioethics Center, Monash University, Melbourne, Australia. ,
Full-Text [PDF 398 kb]
(253 Downloads)
| Abstract (HTML) (441 Views)
2. Case Presentation
3. Discussion
Full-Text: (56 Views)
1. Introduction
Surrogacy, one of the methods of assisted reproduction, offers hope for some infertile people but raises complex ethical questions. These challenges intensify in international surrogacy due to cultural, legal, and economic disparities between countries.
Surrogacy is classified into 2 types based on the source of the ovum: partial (traditional) and complete (gestational). In partial surrogacy, the surrogate’s ovum is fertilized through in vitro fertilization (IVF) or intrauterine insemination with the sperm of the intended father, establishing a genetic link between the surrogate and the child (1). In complete surrogacy, the embryo is created via IVF using ova and sperm from third parties or the intended parents and transferred to the surrogate’s uterus, with no genetic connection to the surrogate (2).
Regarding compensation, surrogacy is divided into altruistic and commercial forms. In altruistic (or only reimbursement) surrogacy, the surrogate’s primary motivation is to help others, not financial gain, and only essential pregnancy-related expenses, particularly medical costs, are covered. In commercial surrogacy, however, profit is a priority, and the surrogate receives payment beyond “reasonable costs”. Defining “reasonable costs” varies across countries, making the distinction between altruistic and commercial surrogacy challenging (3, 4). Commercial surrogacy typically involves an agency that coordinates between the surrogate and intended parents, managing the process for a fee (5).
While many countries prohibit surrogacy entirely or permit only altruistic forms (5, 6), surrogacy remains prevalent and legally permissible in some countries, such as the United States, Ukraine, and Russia (7), with limited oversight (8, 9). Legal and financial factors have fueled cross-border surrogacy (CBS), where intended parents travel abroad for surrogacy services. Despite decades of debate over surrogacy compensation, many countries have yet to address the issue comprehensively or are revising their laws (10). The rise of CBS in recent years (11), has outpaced the development of international regulations, such as treaties or agreements (12).
Surrogacy, in all its forms, raises a wide range of legal, emotional, social, and financial concerns, particularly regarding the vulnerability of surrogate mothers (13). Commercial surrogacy, where a woman carries a child for a couple in exchange for payment, poses even more ethical questions (14). Proponents argue that it empowers women economically by allowing them to use their bodies as a source of income (15), and enables infertile couples to have children (16). Critics, however, contend that commodifying pregnancy raises ethical issues concerning autonomy and human rights, including risks to the surrogate’s physical, mental, and social well-being and her right to motherhood (17). Commercial surrogacy can lead to the exploitation and commodification of women’s bodies, especially in low- and middle-income countries (LMICs) (18, 19). This commodification extends to children, who may be viewed as products for sale, raising profound questions about human dignity and value (20). Legal accountability and children’s rights remain unresolved in this context. CBS exacerbates these ethical concerns, particularly when intended parents are from high-income countries (HICs) and surrogates are from LMICs (10).
International commercial surrogacy, especially when involving HIC parents and LMIC surrogates, reveals deep structural-social inequalities. Some argue that exploitation occurs only when benefits are unfairly distributed or the process causes harm. They suggest that altruistic surrogacy (with limited financial compensation) can also cause physical and psychological harm to surrogates, higher payments in commercial surrogacy could compensate for these risks, enhancing autonomy and justice (10).
However, this perspective faces criticism for overlooking structural-social inequalities such as poverty, illiteracy, and economic pressures that drive women into surrogacy, potentially undermining informed consent (21). Informed consent, a cornerstone of contemporary bioethics, is often compromised in commercial surrogacy due to power imbalances and limited education, which turns the consent process into a formal act. Economic hardship or insufficient literacy may cause undue influence and prevent surrogates from fully understanding legal agreements or the medical and psychological implications of surrogacy. Economic pressures can externally influence consent, particularly when surrogates are unaware of their right to withdraw consent or terminate contracts. A significant concern is that intended parents often exert greater control over pregnancy decisions, such as termination, than surrogates (22).
Considering the potential risks of pregnancy, commercial surrogacy poses significant risks to surrogates, often overlooked during counseling and informed consent process. IVF and multiple embryo transfers increase risks of complications like preeclampsia, gestational diabetes, ovarian torsion, chronic pelvic inflammation, reproductive cancers due to hormone therapy, and infertility (23, 24). Cesarean sections, common in surrogacy due to multiple pregnancies, carry risks of infection or long-term complications. Psychologically, separating the child from the surrogate post-birth can lead to postpartum depression or feelings of loss, particularly if the surrogate faces pressure from breastfeeding or emotional bonding with the fetus (25). If a pregnancy is lost, surrogates may forfeit payment. This necessitates protocols that strengthen surrogates’ autonomy and prevent potential exploitation by middlemen, or genetic parents (14).
Social and cultural factors, including religion, culture, and broader societal contexts, shape the social acceptance of surrogacy. Commercial surrogacy, particularly in international contexts, faces significant legal challenges due to the lack of cohesive, unified regulations across countries. Unlike traditional reproductive travel destinations like India (until 2021), Ukraine, and Russia (26), Iran has not been widely considered as a destination for surrogacy until now. This case establishes Iran as an emerging destination for international commercial surrogacy. Advanced medical infrastructure, low costs, and recent currency devaluation have made Iran attractive to intended parents from HICs. However, the absence of comprehensive laws and adequate oversight exposes Iran to the risk of becoming a center for exploiting vulnerable women. This raises new ethical questions about Iran’s responsibility to regulate this emerging industry and protect the rights of surrogates and children born through surrogacy.
In Iran, surrogacy is facilitated through infertility treatment centers. While assisted reproductive services, including third-party gamete donation, embryo donation, and surrogacy, are available for legally married couples, only embryo donation is regulated by law. Other controversial assisted reproductive methods, including surrogacy, lack clear laws and are practiced in the absence of a specific law and regulation (27). The absence of comprehensive regulations and protocols for international cases has created numerous challenges. This study examines a real-life case of international commercial surrogacy in Iran to explore the ethical, legal, and social challenges arising from CBS arrangements, with particular emphasis on the implications for surrogate mothers, children, and the Iranian healthcare and judicial systems.
Surrogacy is classified into 2 types based on the source of the ovum: partial (traditional) and complete (gestational). In partial surrogacy, the surrogate’s ovum is fertilized through in vitro fertilization (IVF) or intrauterine insemination with the sperm of the intended father, establishing a genetic link between the surrogate and the child (1). In complete surrogacy, the embryo is created via IVF using ova and sperm from third parties or the intended parents and transferred to the surrogate’s uterus, with no genetic connection to the surrogate (2).
Regarding compensation, surrogacy is divided into altruistic and commercial forms. In altruistic (or only reimbursement) surrogacy, the surrogate’s primary motivation is to help others, not financial gain, and only essential pregnancy-related expenses, particularly medical costs, are covered. In commercial surrogacy, however, profit is a priority, and the surrogate receives payment beyond “reasonable costs”. Defining “reasonable costs” varies across countries, making the distinction between altruistic and commercial surrogacy challenging (3, 4). Commercial surrogacy typically involves an agency that coordinates between the surrogate and intended parents, managing the process for a fee (5).
While many countries prohibit surrogacy entirely or permit only altruistic forms (5, 6), surrogacy remains prevalent and legally permissible in some countries, such as the United States, Ukraine, and Russia (7), with limited oversight (8, 9). Legal and financial factors have fueled cross-border surrogacy (CBS), where intended parents travel abroad for surrogacy services. Despite decades of debate over surrogacy compensation, many countries have yet to address the issue comprehensively or are revising their laws (10). The rise of CBS in recent years (11), has outpaced the development of international regulations, such as treaties or agreements (12).
Surrogacy, in all its forms, raises a wide range of legal, emotional, social, and financial concerns, particularly regarding the vulnerability of surrogate mothers (13). Commercial surrogacy, where a woman carries a child for a couple in exchange for payment, poses even more ethical questions (14). Proponents argue that it empowers women economically by allowing them to use their bodies as a source of income (15), and enables infertile couples to have children (16). Critics, however, contend that commodifying pregnancy raises ethical issues concerning autonomy and human rights, including risks to the surrogate’s physical, mental, and social well-being and her right to motherhood (17). Commercial surrogacy can lead to the exploitation and commodification of women’s bodies, especially in low- and middle-income countries (LMICs) (18, 19). This commodification extends to children, who may be viewed as products for sale, raising profound questions about human dignity and value (20). Legal accountability and children’s rights remain unresolved in this context. CBS exacerbates these ethical concerns, particularly when intended parents are from high-income countries (HICs) and surrogates are from LMICs (10).
International commercial surrogacy, especially when involving HIC parents and LMIC surrogates, reveals deep structural-social inequalities. Some argue that exploitation occurs only when benefits are unfairly distributed or the process causes harm. They suggest that altruistic surrogacy (with limited financial compensation) can also cause physical and psychological harm to surrogates, higher payments in commercial surrogacy could compensate for these risks, enhancing autonomy and justice (10).
However, this perspective faces criticism for overlooking structural-social inequalities such as poverty, illiteracy, and economic pressures that drive women into surrogacy, potentially undermining informed consent (21). Informed consent, a cornerstone of contemporary bioethics, is often compromised in commercial surrogacy due to power imbalances and limited education, which turns the consent process into a formal act. Economic hardship or insufficient literacy may cause undue influence and prevent surrogates from fully understanding legal agreements or the medical and psychological implications of surrogacy. Economic pressures can externally influence consent, particularly when surrogates are unaware of their right to withdraw consent or terminate contracts. A significant concern is that intended parents often exert greater control over pregnancy decisions, such as termination, than surrogates (22).
Considering the potential risks of pregnancy, commercial surrogacy poses significant risks to surrogates, often overlooked during counseling and informed consent process. IVF and multiple embryo transfers increase risks of complications like preeclampsia, gestational diabetes, ovarian torsion, chronic pelvic inflammation, reproductive cancers due to hormone therapy, and infertility (23, 24). Cesarean sections, common in surrogacy due to multiple pregnancies, carry risks of infection or long-term complications. Psychologically, separating the child from the surrogate post-birth can lead to postpartum depression or feelings of loss, particularly if the surrogate faces pressure from breastfeeding or emotional bonding with the fetus (25). If a pregnancy is lost, surrogates may forfeit payment. This necessitates protocols that strengthen surrogates’ autonomy and prevent potential exploitation by middlemen, or genetic parents (14).
Social and cultural factors, including religion, culture, and broader societal contexts, shape the social acceptance of surrogacy. Commercial surrogacy, particularly in international contexts, faces significant legal challenges due to the lack of cohesive, unified regulations across countries. Unlike traditional reproductive travel destinations like India (until 2021), Ukraine, and Russia (26), Iran has not been widely considered as a destination for surrogacy until now. This case establishes Iran as an emerging destination for international commercial surrogacy. Advanced medical infrastructure, low costs, and recent currency devaluation have made Iran attractive to intended parents from HICs. However, the absence of comprehensive laws and adequate oversight exposes Iran to the risk of becoming a center for exploiting vulnerable women. This raises new ethical questions about Iran’s responsibility to regulate this emerging industry and protect the rights of surrogates and children born through surrogacy.
In Iran, surrogacy is facilitated through infertility treatment centers. While assisted reproductive services, including third-party gamete donation, embryo donation, and surrogacy, are available for legally married couples, only embryo donation is regulated by law. Other controversial assisted reproductive methods, including surrogacy, lack clear laws and are practiced in the absence of a specific law and regulation (27). The absence of comprehensive regulations and protocols for international cases has created numerous challenges. This study examines a real-life case of international commercial surrogacy in Iran to explore the ethical, legal, and social challenges arising from CBS arrangements, with particular emphasis on the implications for surrogate mothers, children, and the Iranian healthcare and judicial systems.
2. Case Presentation
A 33-yr-old woman, mother of 4 children, pregnant with twins at 32 wk, was admitted to a public hospital in Tehran, Iran due to severe vaginal bleeding. She had connected with an intermediary agency through social media and, driven by financial hardship, agreed to serve as a surrogate specifically through complete (gestational) commercial surrogacy. The financial compensation included an initial payment, monthly payments, and a surplus for a twin pregnancy, totaling 400 million IRR for a single pregnancy (US$ 4000-5000). Due to the emergency, a cesarean section was performed, resulting in the birth of 2 healthy infants.
The surrogate mother reported that the pregnancy was facilitated through embryo transfer at a private infertility clinic in Tehran, Iran for genetic parents residing in the United States. After birth, a lawyer representing the genetic parents submitted the power of attorney and embryo transfer documents to request birth certificates. However, the hospital, citing the absence of the genetic parents and legal complexities around the foreign nationality of the genetic parents, refused to issue the certificates, referring the matter to the regional health authority. The infants were temporarily transferred to welfare services pending resolution. After one and a half months of document review and judicial correspondence, the genetic parents traveled to Iran. A court-approved private laboratory confirmed their genetic relationship through a paternity test, and birth certificates were issued, allowing the infants to be transferred to the US with their genetic parents. The genetic parents or their legal representatives did not obtain a court order to register genetic parentage on the birth certificate prior to birth, likely due to the absence of clear legal pathways for international surrogacy in Iran at the time, as the law does not explicitly provide for pre-birth judicial processes in CBS cases, leading to reliance on post-birth resolutions that exacerbated delays.
While key ethical questions in surrogacy often include the moral justification of commercial surrogacy, distinctions between commercial and altruistic surrogacy, distinctions between international and domestic surrogacy, and ethical considerations of multiple embryo transfers, this case was referred for clinical ethics consultation due to its legal, judicial, and ethical complexities within Iran’s healthcare system. These complexities included the absence of genetic parents at birth, challenges in issuing birth certificates, delays in transferring the infants to their genetic parents, and discrepancies in procedures for Iranian vs. foreign genetic parents.
2.1. Ethical Considerations
A clinical ethics consultation conducted through the hospital ethics committee, with medical ethicists and obstetricians, using the Moral Case Deliberation approach, explored the case’s multifaceted dimensions. For this report, existing documents were reviewed, informed consent was obtained from the surrogate mother, and additional information was gathered through a telephonic interview with the surrogate to complete the analysis.
The surrogate mother reported that the pregnancy was facilitated through embryo transfer at a private infertility clinic in Tehran, Iran for genetic parents residing in the United States. After birth, a lawyer representing the genetic parents submitted the power of attorney and embryo transfer documents to request birth certificates. However, the hospital, citing the absence of the genetic parents and legal complexities around the foreign nationality of the genetic parents, refused to issue the certificates, referring the matter to the regional health authority. The infants were temporarily transferred to welfare services pending resolution. After one and a half months of document review and judicial correspondence, the genetic parents traveled to Iran. A court-approved private laboratory confirmed their genetic relationship through a paternity test, and birth certificates were issued, allowing the infants to be transferred to the US with their genetic parents. The genetic parents or their legal representatives did not obtain a court order to register genetic parentage on the birth certificate prior to birth, likely due to the absence of clear legal pathways for international surrogacy in Iran at the time, as the law does not explicitly provide for pre-birth judicial processes in CBS cases, leading to reliance on post-birth resolutions that exacerbated delays.
While key ethical questions in surrogacy often include the moral justification of commercial surrogacy, distinctions between commercial and altruistic surrogacy, distinctions between international and domestic surrogacy, and ethical considerations of multiple embryo transfers, this case was referred for clinical ethics consultation due to its legal, judicial, and ethical complexities within Iran’s healthcare system. These complexities included the absence of genetic parents at birth, challenges in issuing birth certificates, delays in transferring the infants to their genetic parents, and discrepancies in procedures for Iranian vs. foreign genetic parents.
2.1. Ethical Considerations
A clinical ethics consultation conducted through the hospital ethics committee, with medical ethicists and obstetricians, using the Moral Case Deliberation approach, explored the case’s multifaceted dimensions. For this report, existing documents were reviewed, informed consent was obtained from the surrogate mother, and additional information was gathered through a telephonic interview with the surrogate to complete the analysis.
3. Discussion
Surrogacy in Iran, despite its prevalence in infertility clinics, lacks a clear and comprehensive legal framework, leading to moral distress among healthcare professionals and clinic administrators. Currently, surrogacy arrangements are claimed to be operated under the Embryo Donation Act (2003) (27), which was not designed for surrogacy and fails to address its legal and ethical complexities. This law focuses solely on embryo donation, omitting the rights and obligations of surrogates, genetic parents, or children born through surrogacy. Consequently, informal and unpredictable judicial processes have emerged in hospitals and courts. A significant disparity was observed in the issuance of birth certificates for domestic vs. international surrogacy cases. Under Iranian law, the attending physician is required to issue a birth certificate in the name of the woman who gave birth, and issuing a false certificate carries criminal liability and penalties (28, 29).
In Iran, for all typical pregnancies and deliveries, a hospital birth certificate is first issued for any newborn. Based on this hospital birth certificate, the parents then apply for an official birth certificate from the National Organization for Civil Registration of Iran, which operates under the Ministry of Interior. The same process is followed in routine domestic surrogacy cases involving Iranian genetic parents. The hospital issues the initial birth certificate in the name of the surrogate mother, listing her as the mother in the main section of the form, since she is the one who physically gave birth to the child (or children, in cases of multiple births). The names of the genetic parents are then annotated in the margin of the form, based on supporting documentation provided by the infertility clinic.
Based on this hospital birth certificate, the genetic parents apply for a court order, and a subsequent court ruling instructs the National Organization for Civil Registration to issue an official birth certificate naming only the genetic parents, effectively removing the surrogate’s identity. As a result, in the final official birth certificate, only the genetic parents are listed, while the name of the surrogate mother is retained solely in the records of the hospital, the court, and the Civil Registration Organization.
This case demonstrates that the routine process for international surrogacy cases involving foreign genetic parents differs significantly from that of domestic surrogacy. In this instance, a representative from the commercial surrogacy mediator company requested that the hospital issue the birth certificate directly in the name of the genetic mother, arguing that this is standard practice in international arrangements. In such cases, private fertility clinics typically coordinate with contracted private hospitals to issue the hospital birth certificate directly in the name of the genetic mother, even though she did not physically give birth. Unlike domestic surrogacy, where the surrogate mother’s identity is recorded in the main section of the hospital birth certificate, and the genetic parents’ names appear in the margin, the identity of the surrogate is completely omitted in international cases’ documents. This practice bypasses the standard annotation process leading to the absence of any official record of the surrogate’s involvement in the hospital, judicial, or civil registration documents. As a result, no trace of the surrogate mother was found in the legal records, effectively erasing her role from the official narrative.
In the absence of clear regulations, commercial surrogacy contracts are drawn up opaquely, mediated by infertility clinics and formalized in notary offices, with deliveries typically occurring in private facilities. In cases like this one, where complications necessitate transfer to better-equipped public university hospitals, additional challenges arise.
The central issue is protecting surrogates from harm, particularly exploitation. Iran’s healthcare system has long faced accusations of commodification of the human body and possible exploitation of paid kidney providers (30). Mechanisms like the “gift of reward” for kidney donors, intended to protect vulnerable individuals, have proven inadequate. This raises a red flag for vulnerable surrogate mothers. In this case, while the surrogate was informed of the possibility of a multiple pregnancy, she lacked sufficient knowledge of its risks, and no copy of an informed consent form was provided to her. Additionally, no evidence of pre-pregnancy psychological counseling was found. While the surrogate’s identity is obscured even in domestic surrogacy cases, at least her name appears in some form on the hospital birth certificate. However, in international cases, the surrogate’s name is entirely excluded, raising serious ethical concerns about erasing her identity and commodifying motherhood.
The differing procedures for Iranian and foreign commissioning parents further amplify concerns about discrimination, a recurring issue in medical travel/tourism ethics. In this case, foreign genetic parents received their child without the surrogate’s identity being recorded, placing surrogates in international contracts at an even greater disadvantage compared to those in domestic arrangements. Moreover, the involvement of intermediary agencies minimizes direct contact between the surrogate and genetic parents, further diminishing the potential for human or social connection.
From a children’s rights perspective, Iran’s Embryo Donation Law sets minimal eligibility criteria for commissioning couples, such as legal marriage and financial stability, but these are not enforced in commercial surrogacy, particularly in international cases. This case was managed by the agency, but no evidence of ethical, psychological, or physical health assessments of the genetic parents was found. The delay in issuing birth certificates and the temporary transfer of the infants to welfare services highlighted the vulnerability of children in the absence of robust legal frameworks. In this case, beyond the welfare of children born through surrogacy, the surrogate’s 4 biological children are hidden stakeholders whose psychological and social well-being, impacted by their mother’s participation in surrogacy, remains unexplored and warrants further study. These issues underscore the need for protocols to ensure children’s rights, including oversight of parental eligibility and support for their legal and psychological well-being and identity. The surrogate in this case expressed her intention to pursue surrogacy again due to financial need, raising concerns about the cumulative impact of multiple pregnancies, a twin delivery, and a cesarean section on her physical, mental, and social well-being.
Iran’s economic situation, particularly the sharp devaluation of the national currency (Rial) over the past decade, has made the country an affordable destination for international commercial surrogacy. This cost disparity between Iran and countries such as the USA, combined with opaque contracts, heightens the risk of surrogate exploitation, as many women, driven by economic hardship and lacking legal awareness sign agreements that do not fully protect their rights. These contracts, often non-standardized and inaccessible to the public, are formalized in notary offices, lending an official facing to potentially unfair or exploitative terms. Regulatory oversight of notary offices is needed to prevent such practices. The presence of intermediary agencies in Iran, which coordinate between genetic parents and surrogates, underscores the commercialization of the process. These agencies often earn significant profits, while surrogates receive compensation, equivalent to a few months of Iran’s minimum wage ($200-300 per month), which is inadequate given the medical and psychological risks and cost of living.
Minimum wage standards are an inappropriate benchmark in countries where they fail to cover basic living expenses. Economic disparities, coupled with weak regulation, create conditions for exploiting vulnerable women and position Iran as a destination for reproductive tourism.
Healthcare professionals and clinic administrators, bound by ethical guidelines to prioritize patient care and integrity (31), face moral distress due to legal ambiguities and frequent involvement in judicial processes, as seen in this case. This can lead to defensive medical practices among providers and administrators (32, 33).
While precise details about the operations of intermediary agencies in international surrogacy in Iran are scarce, this case demonstrates that infant handover without the genetic parents’ presence is possible. The agency, armed with the power of attorney, requested the transfer of the infants abroad, highlighting the potential for “surrogacy without genetic parental presence” in the absence of clear regulations. In response to this case, Iran’s Ministry of Health issued a directive, one of the few regulations in this area, classifying the import and export of gametes and embryos as biological materials requiring ministry approval (34). This indirectly mandates the presence of genetic parents and in-country IVF processes, addressing concerns about external gamete imports or absent parents. The directive requires all surrogacy stages, including embryo transfer, to be conducted under the supervision of authorized infertility clinics, with clear documentation of the genetic parents’ and surrogate’s identities. Nevertheless, its lack of detail on surrogates’ rights, fair compensation, and international case management limits its effectiveness.
To address these challenges, the government needs to introduce comprehensive guidelines that include specific protocols for protecting surrogates, ensuring children’s rights, and aligning with international laws to reduce ethical and legal ambiguities.
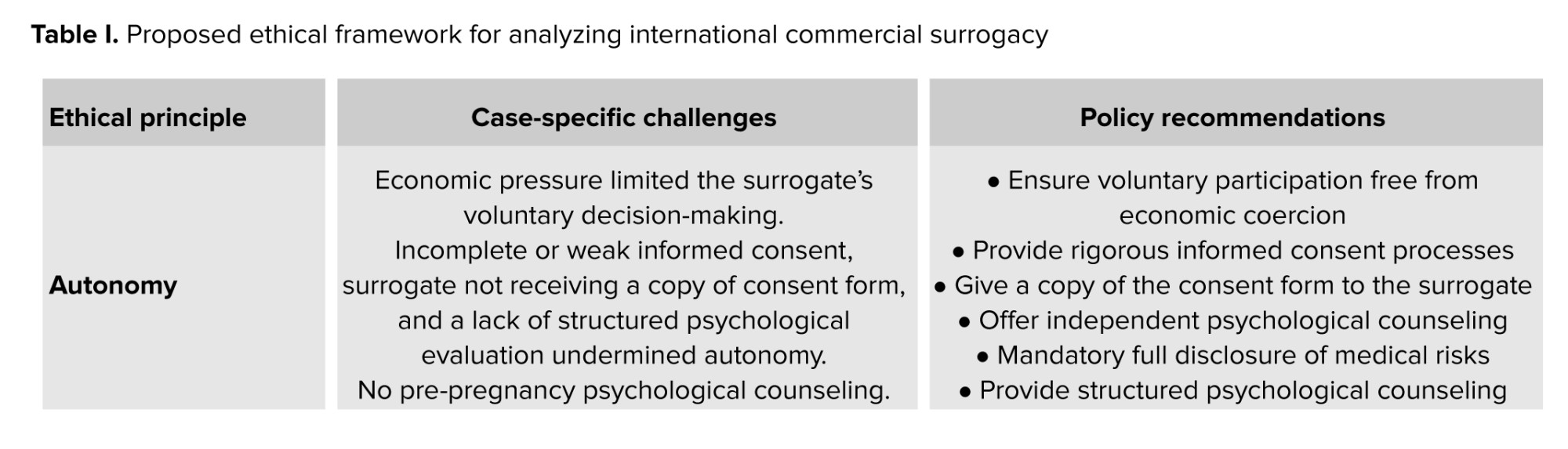
In this study, we applied a multi-dimensional ethical framework to analyze the real-life case of international commercial surrogacy in Iran. The framework integrates the following principles: autonomy, well-being, fairness, transparency, accountability, inclusion, structural justice and equity, children’s rights and welfare, and ethics of care. Table I summarizes the application of this framework to the case and provides corresponding policy recommendations.
It is important to note that this framework does not serve to justify or endorse commercial surrogacy. Rather, it offers a structured approach to assess ethical challenges and safeguards that could make the practice more defensible. Even with full adherence to these principles, some scholars argue that commercial surrogacy remains ethically problematic due to structural exploitation and commodification of women and children. Therefore, while this framework identifies conditions under which ethical concerns could be mitigated, it does not provide an absolute ethical endorsement of international commercial surrogacy.

In Iran, for all typical pregnancies and deliveries, a hospital birth certificate is first issued for any newborn. Based on this hospital birth certificate, the parents then apply for an official birth certificate from the National Organization for Civil Registration of Iran, which operates under the Ministry of Interior. The same process is followed in routine domestic surrogacy cases involving Iranian genetic parents. The hospital issues the initial birth certificate in the name of the surrogate mother, listing her as the mother in the main section of the form, since she is the one who physically gave birth to the child (or children, in cases of multiple births). The names of the genetic parents are then annotated in the margin of the form, based on supporting documentation provided by the infertility clinic.
Based on this hospital birth certificate, the genetic parents apply for a court order, and a subsequent court ruling instructs the National Organization for Civil Registration to issue an official birth certificate naming only the genetic parents, effectively removing the surrogate’s identity. As a result, in the final official birth certificate, only the genetic parents are listed, while the name of the surrogate mother is retained solely in the records of the hospital, the court, and the Civil Registration Organization.
This case demonstrates that the routine process for international surrogacy cases involving foreign genetic parents differs significantly from that of domestic surrogacy. In this instance, a representative from the commercial surrogacy mediator company requested that the hospital issue the birth certificate directly in the name of the genetic mother, arguing that this is standard practice in international arrangements. In such cases, private fertility clinics typically coordinate with contracted private hospitals to issue the hospital birth certificate directly in the name of the genetic mother, even though she did not physically give birth. Unlike domestic surrogacy, where the surrogate mother’s identity is recorded in the main section of the hospital birth certificate, and the genetic parents’ names appear in the margin, the identity of the surrogate is completely omitted in international cases’ documents. This practice bypasses the standard annotation process leading to the absence of any official record of the surrogate’s involvement in the hospital, judicial, or civil registration documents. As a result, no trace of the surrogate mother was found in the legal records, effectively erasing her role from the official narrative.
In the absence of clear regulations, commercial surrogacy contracts are drawn up opaquely, mediated by infertility clinics and formalized in notary offices, with deliveries typically occurring in private facilities. In cases like this one, where complications necessitate transfer to better-equipped public university hospitals, additional challenges arise.
The central issue is protecting surrogates from harm, particularly exploitation. Iran’s healthcare system has long faced accusations of commodification of the human body and possible exploitation of paid kidney providers (30). Mechanisms like the “gift of reward” for kidney donors, intended to protect vulnerable individuals, have proven inadequate. This raises a red flag for vulnerable surrogate mothers. In this case, while the surrogate was informed of the possibility of a multiple pregnancy, she lacked sufficient knowledge of its risks, and no copy of an informed consent form was provided to her. Additionally, no evidence of pre-pregnancy psychological counseling was found. While the surrogate’s identity is obscured even in domestic surrogacy cases, at least her name appears in some form on the hospital birth certificate. However, in international cases, the surrogate’s name is entirely excluded, raising serious ethical concerns about erasing her identity and commodifying motherhood.
The differing procedures for Iranian and foreign commissioning parents further amplify concerns about discrimination, a recurring issue in medical travel/tourism ethics. In this case, foreign genetic parents received their child without the surrogate’s identity being recorded, placing surrogates in international contracts at an even greater disadvantage compared to those in domestic arrangements. Moreover, the involvement of intermediary agencies minimizes direct contact between the surrogate and genetic parents, further diminishing the potential for human or social connection.
From a children’s rights perspective, Iran’s Embryo Donation Law sets minimal eligibility criteria for commissioning couples, such as legal marriage and financial stability, but these are not enforced in commercial surrogacy, particularly in international cases. This case was managed by the agency, but no evidence of ethical, psychological, or physical health assessments of the genetic parents was found. The delay in issuing birth certificates and the temporary transfer of the infants to welfare services highlighted the vulnerability of children in the absence of robust legal frameworks. In this case, beyond the welfare of children born through surrogacy, the surrogate’s 4 biological children are hidden stakeholders whose psychological and social well-being, impacted by their mother’s participation in surrogacy, remains unexplored and warrants further study. These issues underscore the need for protocols to ensure children’s rights, including oversight of parental eligibility and support for their legal and psychological well-being and identity. The surrogate in this case expressed her intention to pursue surrogacy again due to financial need, raising concerns about the cumulative impact of multiple pregnancies, a twin delivery, and a cesarean section on her physical, mental, and social well-being.
Iran’s economic situation, particularly the sharp devaluation of the national currency (Rial) over the past decade, has made the country an affordable destination for international commercial surrogacy. This cost disparity between Iran and countries such as the USA, combined with opaque contracts, heightens the risk of surrogate exploitation, as many women, driven by economic hardship and lacking legal awareness sign agreements that do not fully protect their rights. These contracts, often non-standardized and inaccessible to the public, are formalized in notary offices, lending an official facing to potentially unfair or exploitative terms. Regulatory oversight of notary offices is needed to prevent such practices. The presence of intermediary agencies in Iran, which coordinate between genetic parents and surrogates, underscores the commercialization of the process. These agencies often earn significant profits, while surrogates receive compensation, equivalent to a few months of Iran’s minimum wage ($200-300 per month), which is inadequate given the medical and psychological risks and cost of living.
Minimum wage standards are an inappropriate benchmark in countries where they fail to cover basic living expenses. Economic disparities, coupled with weak regulation, create conditions for exploiting vulnerable women and position Iran as a destination for reproductive tourism.
Healthcare professionals and clinic administrators, bound by ethical guidelines to prioritize patient care and integrity (31), face moral distress due to legal ambiguities and frequent involvement in judicial processes, as seen in this case. This can lead to defensive medical practices among providers and administrators (32, 33).
While precise details about the operations of intermediary agencies in international surrogacy in Iran are scarce, this case demonstrates that infant handover without the genetic parents’ presence is possible. The agency, armed with the power of attorney, requested the transfer of the infants abroad, highlighting the potential for “surrogacy without genetic parental presence” in the absence of clear regulations. In response to this case, Iran’s Ministry of Health issued a directive, one of the few regulations in this area, classifying the import and export of gametes and embryos as biological materials requiring ministry approval (34). This indirectly mandates the presence of genetic parents and in-country IVF processes, addressing concerns about external gamete imports or absent parents. The directive requires all surrogacy stages, including embryo transfer, to be conducted under the supervision of authorized infertility clinics, with clear documentation of the genetic parents’ and surrogate’s identities. Nevertheless, its lack of detail on surrogates’ rights, fair compensation, and international case management limits its effectiveness.
To address these challenges, the government needs to introduce comprehensive guidelines that include specific protocols for protecting surrogates, ensuring children’s rights, and aligning with international laws to reduce ethical and legal ambiguities.
In this study, we applied a multi-dimensional ethical framework to analyze the real-life case of international commercial surrogacy in Iran. The framework integrates the following principles: autonomy, well-being, fairness, transparency, accountability, inclusion, structural justice and equity, children’s rights and welfare, and ethics of care. Table I summarizes the application of this framework to the case and provides corresponding policy recommendations.
It is important to note that this framework does not serve to justify or endorse commercial surrogacy. Rather, it offers a structured approach to assess ethical challenges and safeguards that could make the practice more defensible. Even with full adherence to these principles, some scholars argue that commercial surrogacy remains ethically problematic due to structural exploitation and commodification of women and children. Therefore, while this framework identifies conditions under which ethical concerns could be mitigated, it does not provide an absolute ethical endorsement of international commercial surrogacy.
4. Conclusion
International commercial surrogacy in Iran, driven by economic disparities and a lack of legal frameworks, raises profound ethical challenges, including moral distress for healthcare professionals, exploitation, and commodification of women and children. This case revealed how economic pressures undermine surrogates’ autonomy and turn informed consent into a merely formal act. The erasure of surrogates’ identities in legal documents for international cases, unlike domestic ones, exposes structural discrimination and violates human dignity. From a children’s rights perspective, the absence of mechanisms to verify commissioning parents’ ethical, psychological, and financial suitability heightens the risk of child exploitation. Medical and psychological risks to surrogates, social impacts on their biological children, and vulnerabilities of children born through surrogacy highlight the need for comprehensive protections. Commercialization, exacerbated by intermediary agencies and opaque contracts, further fuels the commodification of women and children. While this case prompted a Ministry of Health directive mandating the presence of genetic parents, other aspects of surrogacy, particularly international commercial cases, remain unregulated. Iran’s emergence as a reproductive tourism destination underscores its responsibility to regulate this process. It is recommended that until transparent legal frameworks are developed with stakeholder input, all commercial surrogacy, especially international cases, be suspended.
Author Contributions
E. Shamsi Gooshki: Designed and supervised the research and critically revised the manuscript. M. Jafari: Administrative support for data collection. M. Malbakhsh: Data collection. M. Modabber: Drafted the manuscript and contributed to data collection. M. Modabber and A. Parsapour: Data analysis and interpretation. All authors read and approved the final manuscript.
Acknowledgments
The authors express their gratitude to the surrogate mother, hospital authorities, and academic staff and students of Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran for their collaboration in the ethical analysis of this case. ChatGPT (version 4) was used solely for translation and grammar checking during the preparation of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Author Contributions
E. Shamsi Gooshki: Designed and supervised the research and critically revised the manuscript. M. Jafari: Administrative support for data collection. M. Malbakhsh: Data collection. M. Modabber: Drafted the manuscript and contributed to data collection. M. Modabber and A. Parsapour: Data analysis and interpretation. All authors read and approved the final manuscript.
Acknowledgments
The authors express their gratitude to the surrogate mother, hospital authorities, and academic staff and students of Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran for their collaboration in the ethical analysis of this case. ChatGPT (version 4) was used solely for translation and grammar checking during the preparation of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Case Report |
Subject:
Medical Ethics in Reproductive Sciences
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
