
International Journal of
Reproductive Biomedicine
Tue, Jun 23, 2026
[Archive]
Volume 24, Issue 4 (April 2026)
IJRM 2026, 24(4): 315-324 |
Back to browse issues page


Ethics code: IR.MAZUMS.IMAMHOSPITAL.REC.1398.006
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zamaniyan M, Abbasi T, Habibpour M, Peyvandi S, Jafarpour H, Mohammadpour Tahamtan R A et al . Effect of dual trigger on pregnancy outcomes in women with diminished ovarian reserve: A single-blind randomized clinical trial. IJRM 2026; 24 (4) :315-324
URL: http://ijrm.ir/article-1-3675-en.html
URL: http://ijrm.ir/article-1-3675-en.html
Marzieh Zamaniyan1 

 , Tahereh Abbasi2 , Manizheh Habibpour *3 , Sepideh Peyvandi4 , Hamed Jafarpour2 , Reza Ali Mohammadpour Tahamtan5 , Noushin Gordani6
, Tahereh Abbasi2 , Manizheh Habibpour *3 , Sepideh Peyvandi4 , Hamed Jafarpour2 , Reza Ali Mohammadpour Tahamtan5 , Noushin Gordani6
, Tahereh Abbasi2 , Manizheh Habibpour *3 , Sepideh Peyvandi4 , Hamed Jafarpour2 , Reza Ali Mohammadpour Tahamtan5 , Noushin Gordani6
1- Sexual and Reproductive Health Research Center, Mazandaran University of Medical Sciences, Sari, Iran. & Diabetes Research Center, Mazandaran University of Medical Sciences, Sari, Iran.
2- Student Research Committee, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Laboratory Sciences, School of Allied Medical Sciences, Mazandaran University of Medical Sciences, Sari, Iran. & Department of Laboratory Hematology and Blood Banking, School of Allied Medical Sciences, Kerman University of Medical Sciences, Kerman, Iran. ,manizheh.habibpour@yahoo.com; m.habibpour@kmu.ac.ir
4- Department of Obstetrics and Gynecology, School of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
5- Department of Biostatistics and Epidemiology, School of Health, Diabetes Research Center, Cancer Research Institute, Mazandaran University of Medical Sciences, Sari, Iran.
6- Mazandaran University of Medical Sciences, Sari, Iran.
2- Student Research Committee, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Laboratory Sciences, School of Allied Medical Sciences, Mazandaran University of Medical Sciences, Sari, Iran. & Department of Laboratory Hematology and Blood Banking, School of Allied Medical Sciences, Kerman University of Medical Sciences, Kerman, Iran. ,
4- Department of Obstetrics and Gynecology, School of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
5- Department of Biostatistics and Epidemiology, School of Health, Diabetes Research Center, Cancer Research Institute, Mazandaran University of Medical Sciences, Sari, Iran.
6- Mazandaran University of Medical Sciences, Sari, Iran.
Keywords: Intracytoplasmic sperm injections, Human chorionic gonadotropin, Gonadotropin-releasing hormone agonist, Ovarian stimulation.
Full-Text [PDF 428 kb]
(145 Downloads)
| Abstract (HTML) (188 Views)
Full-Text: (17 Views)
1. Introduction
Ovarian reserve can be a predictor of reproductive outcomes in women, whose rate is different at every age. Diminished ovarian reserve (DOR) as a medical condition is one of the problems in assisted reproductive treatment. The prevalence of DOR is 5-18% in the in vitro fertilization (IVF) cycles. The extent of pregnancy in this group of women is very low, 2-4% (1).
There are multiple definitions for patients with poor ovarian reserve or DOR. The European Society of Human Reproduction and Embryology introduced standardized diagnostic criteria, known as the Bologna criteria, to identify patients with DOR. These criteria include: 1) age ≥ 40 yr; 2) poor response to IVF (cycle cancellation due to lack of follicular growth or retrieval of ≤ 3 oocytes); and 3) abnormal ovarian reserve tests (anti-Müllerian hormone [AMH] < 1.1 ng/ml or antral follicle count < 7 in both ovaries) (2-3).
Women with severe DOR usually have little time to become pregnant with their own ova. Different protocols have been scrutinized to increase fertility rates in this group of women, but none have been superior to the other (1, 2). The gonadotropin-releasing hormone (GnRH) antagonist protocol is a standard method in IVF cycles to prevent the premature luteinizing hormone (LH) surge, especially in poor responders. Human chorionic gonadotropin (HCG) is commonly used to induce LH surge and final oocyte maturation in IVF cycles for final follicular maturation (1).
One of these interventions in women with DOR is the augmentation of GnRH agonist into an HCG ampoule at final follicular maturation to improve final oocyte maturation in antagonist cycles. The possible mechanism is to mimic the physiological cycle and induce follicle-stimulating hormone (FSH) peak in the cycle and increase the number of mature oocytes (1, 2). In contrast, the HCG only induces the LH peak. However, the relevant studies reported contradictory findings, some of which have been applied in females with severe ovarian response to reduce the risk of ovarian hyperstimulation syndrome (1, 2). Numerous studies have been used in normal responders, and the number of oocytes and extent of pregnancy have increased in some of them (1-5). In a meta-analysis study on normal responders, the addition of agonists to HCG resulted in a significant improvement in the clinical pregnancy in antagonist cycles. However, the extent of pregnancy was not observed in other indices, such as the number of mature or fertilized oocytes (1).
However, fewer studies have been conducted on poor responders or were found to be associated with inconsistent findings. In the other 2 studies, there was no difference in dual ovarian stimulation or the GnRH agonist + HCG and HCG alone in normal and poor responders (1, 2), which may be due to lower doses of HCG in these 2 studies and fresh embryo transfer (ET). Studies have shown that final stimulation with agonists can reduce endometrial receptivity and the extent of pregnancy in fresh ET cycles. Due to low studies in poor responders, low oocyte counts, and low-quality oocytes and embryos despite high doses of gonadotropin hormone in IVF cycles, we decided to investigate the effect of final follicular stimulation with HCG agonist with HCG + GnRH compared to previous studies within a prospective study in the antagonist cycles on retrieved oocytes, mature oocytes and fetal counts, and good quality fetuses and clinical pregnancy in frozen cycles rather than fresh cycles in previous studies and abortion rates (3-6).
This prospective study seeks to clarify the role of dual triggering in poor responders, addressing gaps in existing literature by focusing on frozen cycles rather than fresh transfers, which may better preserve endometrial receptivity and improve pregnancy outcomes.
2. Materials and Methods
2.1. Study design and cases
The present single-blind randomized clinical trial was conducted on infertile women with diminished ovarian response referred to the Kosar Infertility Center, Imam Khomeini hospital, Sari, Iran, between May and November 2019 to initiate an intracytoplasmic sperm injection-ET cycle.
Inclusion criteria were women aged 20-45 yr, normal endometrium in hysterosalpingography, AMH levels < 1.1 ng/ml, antral follicle count < 7 in both ovaries, and prior < 3 failed IVF cycles. Women with normal ovarian response in ovulatory cycles were excluded from the study.
2.2. Intervention
Cases that met the inclusion criteria and demonstrated a poor ovarian response (antral follicle count < 7 or AMH level < 1.1 ng/ml), as confirmed by previous medical history, were consulted.
Women who have entered the IVF cycle were randomly assigned to each group and randomized based on the randomized block software.
Women were entered into each group by an IVF nurse, and the ultrasound operator was blind to the intervention.
All women who underwent the antagonist protocol for ovulation induction due to poor ovarian response and received daily 300 IU subcutaneous Cinnal‑F (75 IU/mL Follitropin alfa, CinnaGen Co., Iran) starting on day 3 of menstruation (based on age and ovarian reserve test results) were included in the study.
Upon follicle size of 12-14 mm, they received 250 µg of subcutaneous Cetrotide as GnRH antagonist (Cetrorelix acetate 0.25 mg, Merck Serono, Germany) daily, and folliculography and endometrial thickness examinations were routinely performed. The dose of gonadotropins was adjusted based on the size and number of follicles observed on ultrasound. When 2 or more follicles reached 17 mm or more in size, 10,000 units of intramuscular Choriomon (HCG 5000 IU, IBSA Co., Switzerland) and 0.2 mg of subcutaneous Variopeptyl® (Triptorelin acetate 0.1 mg), a GnRH agonist (Varian Pharmed Pharmaceutical Co., Iran) were injected. Then, oocyte retrieval was performed 34-36 hr later. In the next cycle, transplantation of 2 or 3 8-12-cell embryos was performed according to the age of the case, starting with oral estradiol 2 mg, 3 times daily, and serial transvaginal ultrasound (HONDA-2000, 7.5 megahertz) reaching an endometrium above 7 mm. In the HCG group, an intracytoplasmic sperm injection-ET cycle was performed with Chorimonas injection alone, and the cycle continued as mentioned earlier.
Luteal support was started in the frozen ET cycle after administration of 6 mg daily estradiol and reaching endometrial thickness above 7 mm, and 3 days before ET. The females received a single Cyclogest vaginal suppository (Progesterone 400 mg, Actover Inc., the UK) every 12 hr. The pregnancy test with blood β-HCG was estimated to be 15 days after ET. If tested positive, luteal support continued until 12 wk of gestation. If the pregnancy test was positive, the serial transvaginal ultrasound was performed 3-4 wk later to confirm gestational sac and clinical pregnancy.
2.3. Outcomes and data collection
The primary outcome of the study was the clinical pregnancy rate. This was assessed 4 wk after ET by transvaginal ultrasound performed by a qualified physician. The presence of a gestational sac was considered confirmation of clinical pregnancy.
The secondary outcomes included several parameters related to ovarian response, embryo development, and pregnancy progression. The oocyte recovery rate was evaluated 48 hr after administration of HCG. Oocytes were retrieved and examined under light microscopy by an experienced physician to determine the number and maturity of oocytes collected. Embryo development was assessed 3 days after oocyte retrieval. Embryos were cultured and evaluated microscopically, with the embryo rate calculated based on the proportion of fertilized oocytes that developed into cleavage-stage embryos.
Additional secondary outcomes included the miscarriage rate, which was monitored for up to 20 wk after ET. Miscarriage was defined as pregnancy loss prior to 20 wk of gestation and was confirmed by ultrasound examination. Oocyte quality was also assessed at the time of oocyte retrieval. Each oocyte was examined microscopically to determine morphological characteristics and maturity, providing an index of oocyte quality for each patient.
2.4. Sample size
The sample size was determined with reference to the study by Shapiro et al. which compared dual trigger (HCG + GnRH agonist) with HCG alone for final oocyte maturation in IVF cycles (7). Given the similarity in design, we adopted a sample size of 40 patients per group in the present study. To account for potential attrition, 82 women were recruited, ensuring that 80 participants (40 per group) remained for analysis.
For clinical outcomes (e.g., clinical pregnancy rate), the sample size was calculated using the formula for 2 independent proportions:

Where p1 = 0.82, p2 = 0.63, pˉ = (p1 + p2)/2, α = 0.05, and power 1-β = 0.80. This calculation indicates that approximately 85 participants per group would be required to detect a 19% absolute difference in clinical pregnancy rates with adequate power. Our study, with 40 per group, was therefore underpowered for clinical endpoints, which we acknowledge as a limitation.
For laboratory outcomes (e.g., number of metaphase II [MII] oocytes), the formula for 2 independent means was applied:
Where σ2 is the estimated variance and δ is the minimum clinically important difference. Assumptions for σ and δ were derived from pilot data and previous literature. Based on these assumptions, approximately 40 participants per group were sufficient to detect differences in laboratory outcomes with 80% power at α = 0.05.
To account for potential dropouts, 10% was added to the calculated sample size, resulting in a total recruitment of 82 women.
2.5. Ethical Considerations
This study may not benefit the individual; although evidence has shown that co-administration of GnRH agonist with HCG has been beneficial in final follicular stimulation for females with poor ovarian response, it is not harmful to the female. In accordance with ethical principles, written consent was obtained from all cases before entering the study. Complete and transparent information about the research process was given to the participants. The participants could freely leave the study at any stage of the project. All records were kept confidential. No cost was received from females at any stage of the study. The study began after receiving approval from the ethics committee on Biomedical Research at Imam Khomeini hospital, Sari, Iran (Code: IR.MAZUMS.IMAMHOSPITAL.REC.1398.006) and the Iranian Registry of Clinical Trials (IRCT20160815029374N4). The registration date was May 09, 2019, 1398/02/19 and the last date of updating the registry system is July 21, 2025, 1404/04/30.
2.6. Statistical Analysis
The statistical analysis was performed on both categorical and numerical data. Categorical variables (e.g., history of pregnancy and abortion) were presented as frequencies and percentages. Numerical variables (e.g., age, oocyte counts, embryo counts, and implantation rate) were expressed as mean ± standard deviation.
The normality of the distribution for all numerical variables was assessed using the Kolmogorov-Smirnov test. Based on the normality test results, intergroup comparisons were conducted using the Independent Samples t test for normally distributed data and the Mann-Whitney U test for non-normally distributed data. Comparisons of categorical variables between the groups were performed using the Chi-square test. A p < 0.050 was considered statistically significant for all analyses. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (Released 2012; IBM Corp., Armonk, NY, USA).
3. Results
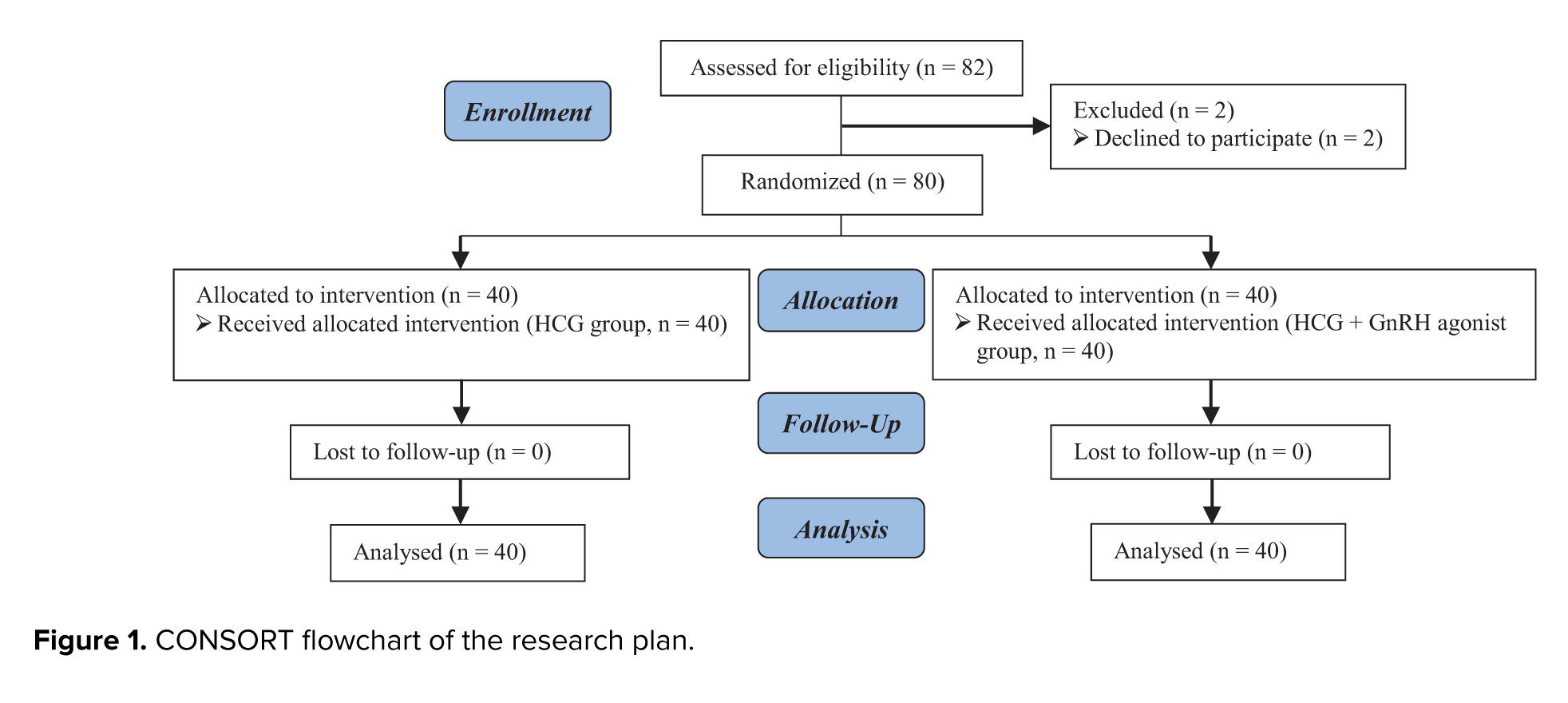
A total of 82 infertile women were assessed for eligibility. 2 participants declined to participate, resulting in 80 women who were randomized into 2 groups of 40 each. All 80 participants received their allocated intervention and were included in the final analysis (Figure 1).
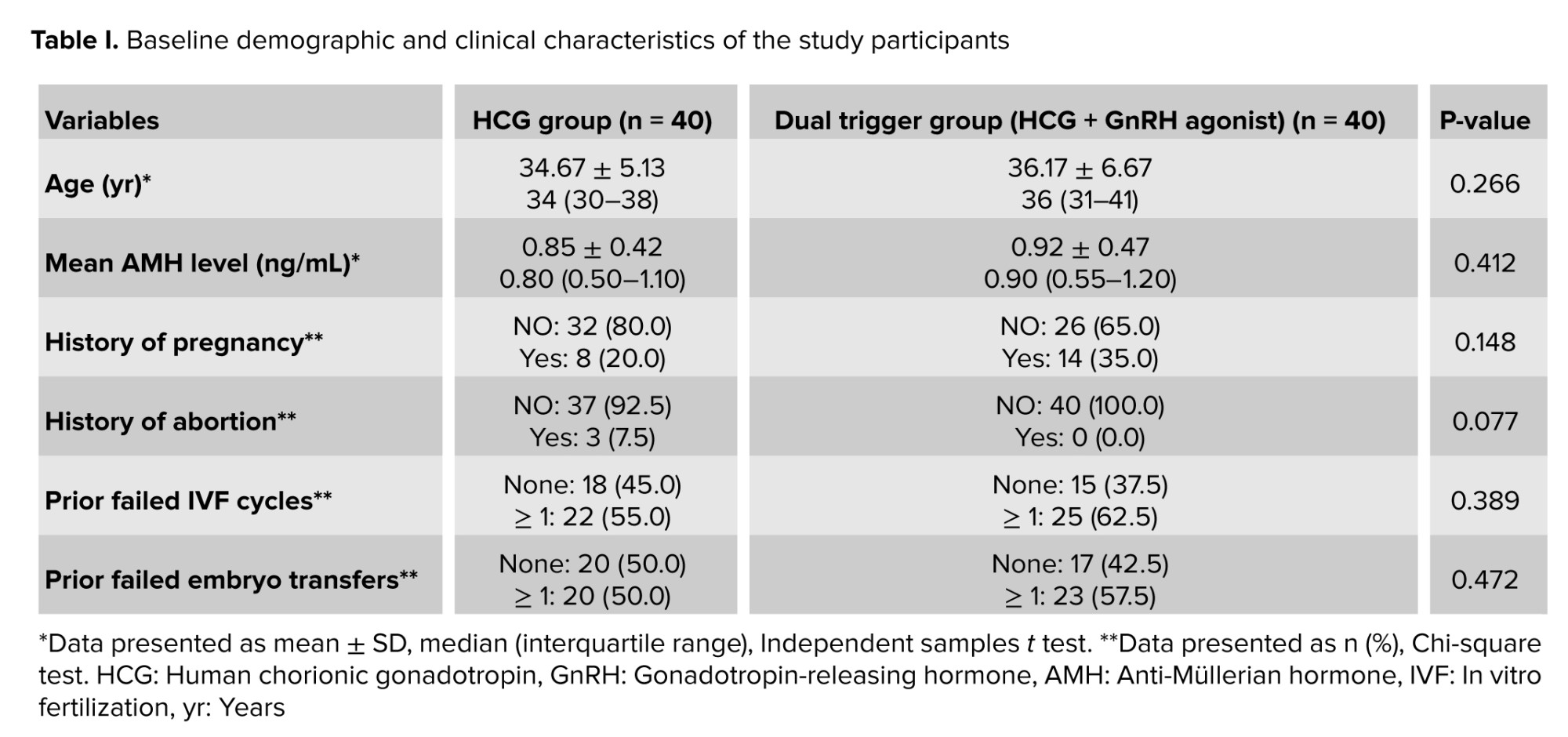
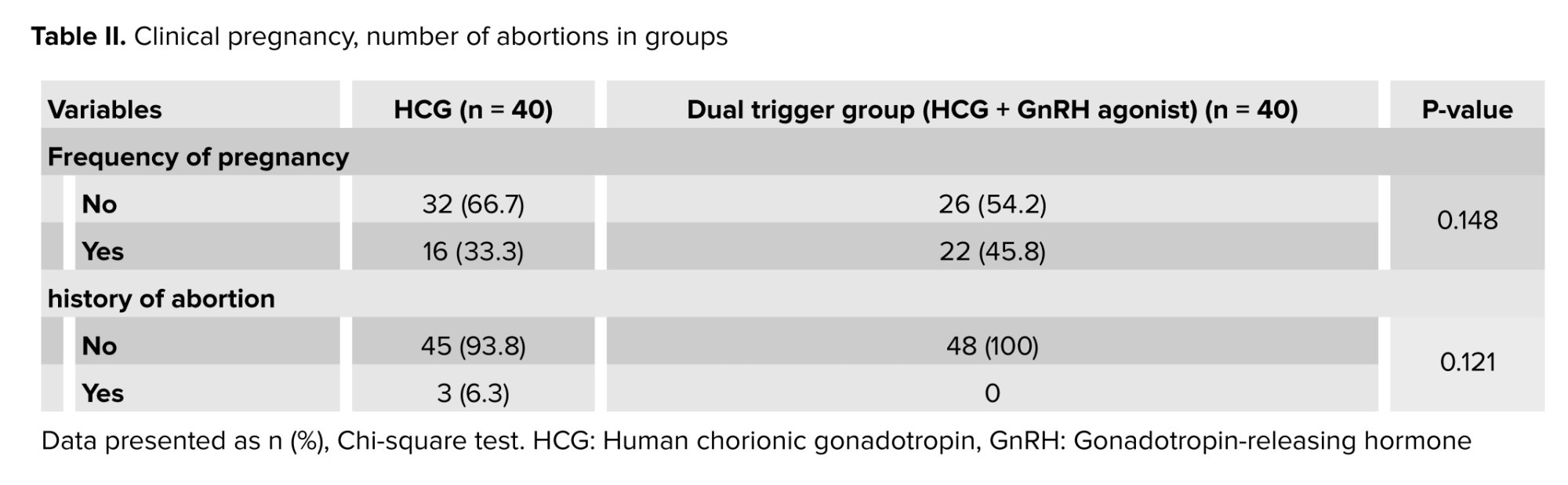
The baseline demographic and clinical characteristics of the participants are presented in table I. The 2 groups were comparable at baseline, with no statistically significant differences observed in age, history of pregnancy, or history of abortion (all p > 0.050). In the clinical pregnancy, the number of abortions in both groups are presented in table II.
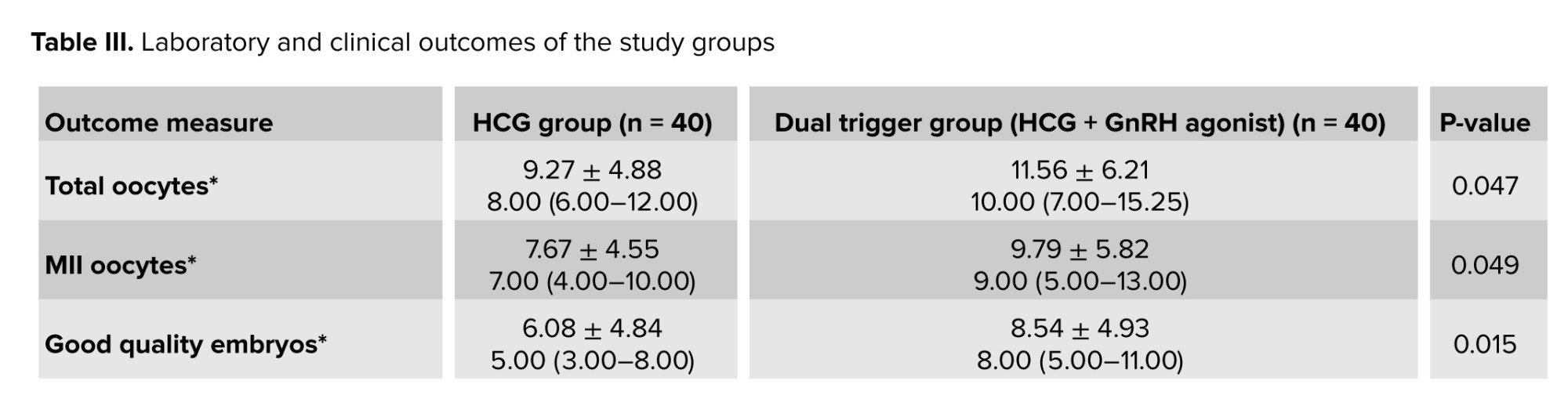
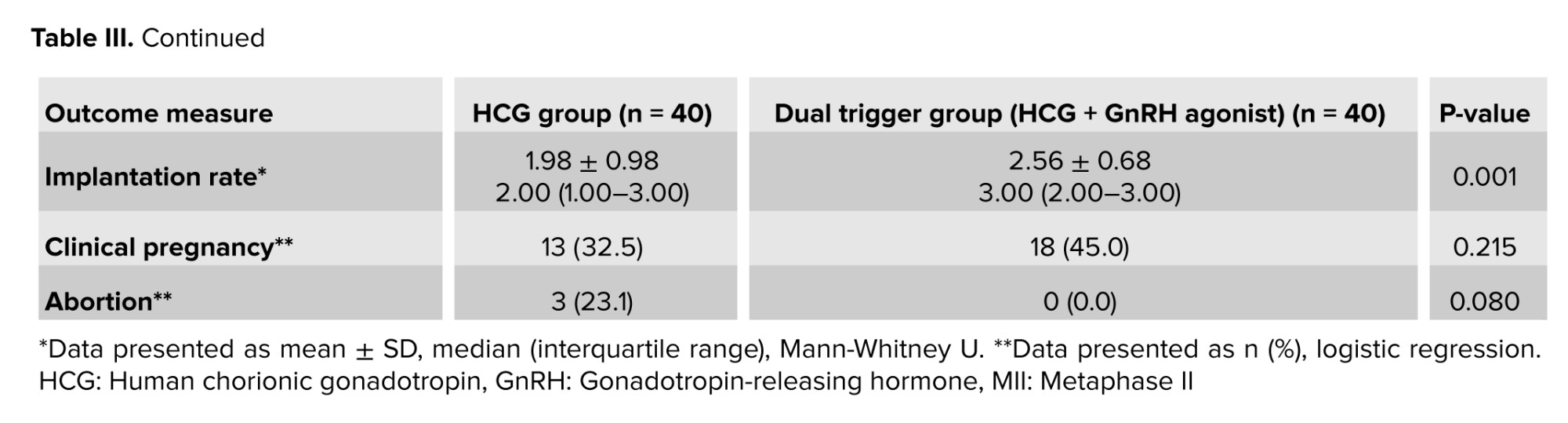
As shown in table III, the mean number of total oocytes and mature oocytes (MII) was lower in the HCG group compared with the dual trigger group (HCG + GnRH agonist). Statistical analysis demonstrated a significant difference between the 2 groups for both total oocytes and MII oocytes (p ≤ 0.050). Similarly, the number of good-quality embryos was significantly higher in the dual trigger group than in the HCG group (p ≤ 0.050). This difference was reflected in the implantation rate, which was also significantly greater in the dual trigger group (p ≤ 0.050).
Although the clinical pregnancy rate appeared higher in the dual trigger group compared with the HCG group, the difference did not reach statistical significance (p > 0.050). Likewise, no significant difference was observed in abortion rates between the 2 groups, despite the absence of abortions in the dual trigger group.
4. Discussion
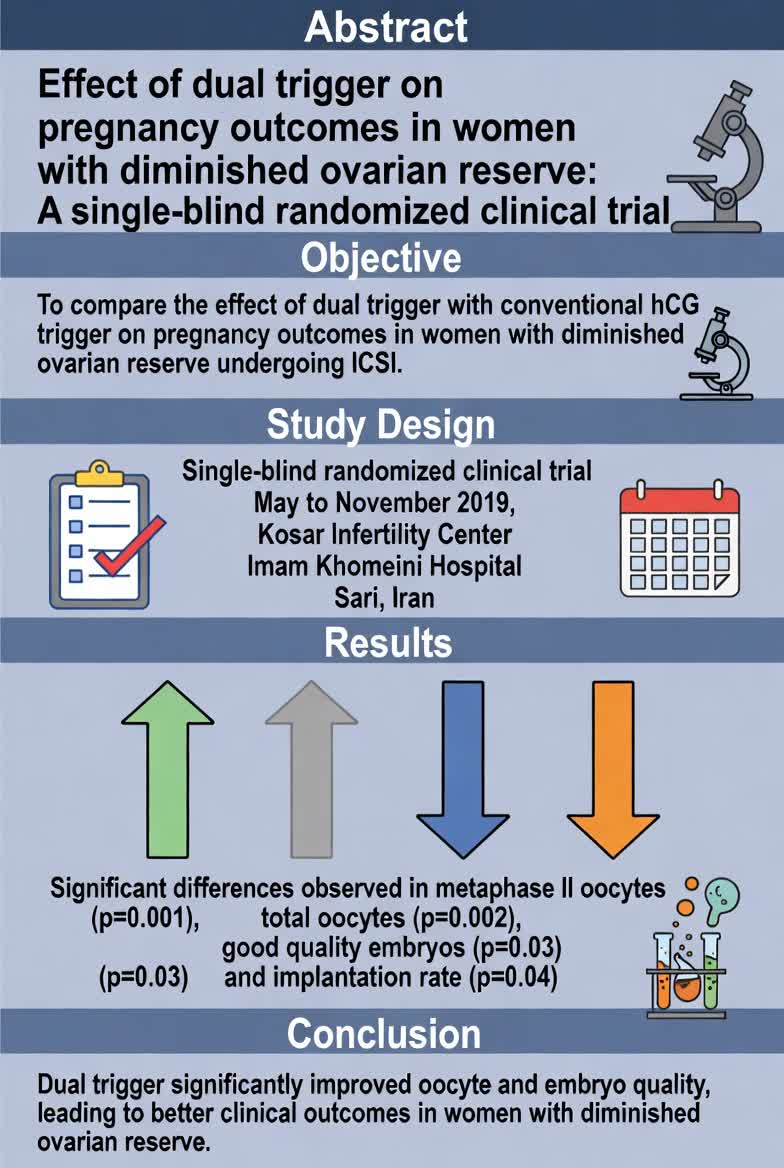
This study demonstrated that using a dual trigger (HCG + GnRH agonist) for final oocyte maturation significantly improved laboratory outcomes in women with DOR compared with HCG alone. The dual‑trigger group produced a higher number of total and MII oocytes, better‑quality embryos, and a superior implantation rate. These results align with earlier studies, reinforcing evidence that dual triggering can enhance oocyte maturation and embryo quality in poor responders (5, 8, 9-14).
The physiological basis for this improvement lies in the GnRH‑agonist-induced surge of both LH and FSH, mimicking the natural mid‑cycle hormonal peak more accurately than HCG alone, which elicits only an LH‑like response. The concurrent FSH surge facilitates optimal follicular maturation by upregulating gonadotropin receptors in granulosa cells, promoting cumulus expansion, and improving cytoplasmic maturation-all critical for oocyte competence and embryo viability (8, 11).
Several investigations have similarly reported an enhancement in oocyte and embryo parameters following dual triggering in this population (5, 9, 13, 15). For example, Chen et al. observed improved mature‑oocyte yield and embryo quality in women with DOR, while the 2025 meta‑analysis by Mercorio et al. confirmed the benefit of dual triggering among poor ovarian responders defined by both the Bologna and POSEIDON criteria (11).
However, clinical outcomes such as pregnancy and live‑birth rates remain inconsistent. Some studies, particularly smaller single‑center trials (10, 15), did not demonstrate statistically significant differences despite improved laboratory results. A 2023 meta‑analysis reported higher pregnancy rates in fresh cycles but considerable inter‑study variability (7). These discrepancies likely reflect differences in study design, patient selection, and limited sample sizes that reduce statistical power.
Variation in stimulation protocol and transfer strategy also contributes to heterogeneity. Trials performing fresh ET often reported reduced benefits, potentially because GnRH‑agonist use may impair endometrial receptivity. By contrast, our study employed frozen ET cycles, minimizing this effect and enabling transfer into a hormonally synchronized endometrium. Additionally, disparities in HCG dosage, timing of oocyte retrieval, and luteal‑phase support can influence clinical outcomes (16).
Collectively, available evidence suggests that while dual triggering consistently enhances laboratory indicators (notably oocyte maturity and embryo quality) the effect on clinical endpoints is less uniform and likely multifactorial, influenced by patient characteristics, protocol details, and study design. Future large, multicenter randomized controlled trials are warranted to delineate which subgroups of women with DOR derive the greatest clinical benefit (17, 18).
In summary, employing a dual trigger with GnRH agonist and HCG represents a promising and biologically sound approach for improving oocyte and embryo outcomes in women with DOR, potentially advancing IVF efficiency in this difficult‑to‑treat population.
Here is a condensed version of that text (approx. 220 words), focusing on clarity and flow:
While studies consistently show that dual triggering reliably improves laboratory outcomes (specifically oocyte maturation and embryo quality) its impact on clinical pregnancy and live-birth rates remains variable (5, 8, 11-13). Despite superior embryological yield, our study observed only a favorable trend, rather than statistical significance, in clinical pregnancy and miscarriage rates. This disconnect is well-documented; while oocyte yield and embryo quality are key, clinical success is multifactorial, depending on endometrial receptivity, transfer technique, luteal-phase support, and patient-specific factors such as age and comorbidities (4, 8, 11). Furthermore, DOR is itself associated with higher miscarriage risks, further complicating clinical outcomes (4).
The lack of statistical significance in our study likely reflects limitations in sample size and power, a common challenge in single-center trials focusing on poor responders (10, 15). Conversely, larger multi-center studies have reported significant improvements in clinical pregnancy and live-birth rates, underscoring the need for adequately powered trials to confirm these benefits (6, 11, 14, 18).
In conclusion, dual triggering is a promising strategy to enhance embryological outcomes in women with DOR. By producing more and higher-quality embryos, this approach optimizes the fertilization process and represents a practical advancement in treating this challenging patient population. Future large-scale randomized controlled trials are essential to definitively determine the long-term clinical impact and identify the specific subgroups that benefit most (6, 17, 18).
4.1. Strengths and Limitations
This study possesses several notable strengths. First, its design as a RCT minimizes selection bias and enhances the internal validity of the findings through random allocation of participants. Second, the focus on frozen ET cycles in women with DOR addresses a critical gap in the literature, as many prior studies utilized fresh transfers where GnRH agonist effects on endometrial receptivity may confound outcomes. Third, the use of a standardized, clinically relevant protocol improves the reproducibility and practical applicability of the results.
Several limitations should be considered. The single-center design and relatively small sample size limit the statistical power to detect differences in clinical outcomes such as pregnancy and live birth rates. The study also lacked long-term follow-up, preventing assessment of cumulative live birth rates or neonatal outcomes. Additionally, the homogeneous participant population may restrict generalizability to broader groups, such as those with obesity or other comorbidities. Finally, the absence of detailed cost-effectiveness analysis or data on patient-reported outcomes (e.g., treatment tolerability) represents an area for future research. Addressing these limitations in larger, multi-center trials would strengthen the evidence base.
5. Conclusion
Final oocyte maturation using dual ovarian stimulation with GnRH agonists and HCG improves the number of good-quality embryos and can be a practical approach to enhance the efficiency of the fertilization process in infertile women with DOR. Further research into larger sample sizes is needed to determine the specificity of the effect on quality of oocyte and the extent of pregnancy. Future research is suggested to investigate the effect of human GnRH agonist therapy and human gonadotropin on infertile women, with more underlying variables being assessed during the study and their correlation with the extent of pregnancy.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to ethical considerations and participant confidentiality. However, anonymized data may be made available upon reasonable requests from qualified researchers, subject to approval by the institutional ethics committee. Requests for data access should be directed to the corresponding author and will require a formal data sharing agreement to ensure compliance with ethical and legal standards. Any shared data will be stripped of identifiable information to protect participant privacy. For further inquiries, please contact manizheh.habibpour@yahoo.com.
Author Contributions
M. Zamaniyan: Conceptualization, methodology, supervision, writing-review and editing. T. Abbasi: Data curation, formal analysis, investigation, writing-original draft. M. Habibpour: Conceptualization, methodology, resources, supervision, writing-review and editing. S. Peyvandi: Conceptualization, methodology, resources, supervision, writing-review and editing. H. Jafarpour: Investigation, data curation. R.A. Mohammadpour Tahamtan: Formal analysis, software, validation. N. Gordani: Resources, project administration. Manizheh Habibpour and Sepideh Peyvandi are designated as co-corresponding authors. This is because the study involves interdisciplinary collaboration across laboratory sciences (MH's expertise) and clinical obstetrics/gynecology (SP's expertise), with both authors sharing equal responsibility for overseeing the research, responding to post-publication queries, managing data access requests, and handling correspondence with the journal and readers.
Acknowledgments
We thank the staff and colleagues at Mazandaran University of Medical Sciences and Sari Imam Khomeini hospital, Sari, Iran for their valuable support during this study. We are also grateful to the biostatistics consultant for assistance with data analysis and to the patients who participated generously. Without their cooperation and trust, this research would not have been possible. The authors declare that no Artificial Intelligence tools, including large language models or translation software, were used in the writing, revision, or data analysis of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Ovarian reserve can be a predictor of reproductive outcomes in women, whose rate is different at every age. Diminished ovarian reserve (DOR) as a medical condition is one of the problems in assisted reproductive treatment. The prevalence of DOR is 5-18% in the in vitro fertilization (IVF) cycles. The extent of pregnancy in this group of women is very low, 2-4% (1).
There are multiple definitions for patients with poor ovarian reserve or DOR. The European Society of Human Reproduction and Embryology introduced standardized diagnostic criteria, known as the Bologna criteria, to identify patients with DOR. These criteria include: 1) age ≥ 40 yr; 2) poor response to IVF (cycle cancellation due to lack of follicular growth or retrieval of ≤ 3 oocytes); and 3) abnormal ovarian reserve tests (anti-Müllerian hormone [AMH] < 1.1 ng/ml or antral follicle count < 7 in both ovaries) (2-3).
Women with severe DOR usually have little time to become pregnant with their own ova. Different protocols have been scrutinized to increase fertility rates in this group of women, but none have been superior to the other (1, 2). The gonadotropin-releasing hormone (GnRH) antagonist protocol is a standard method in IVF cycles to prevent the premature luteinizing hormone (LH) surge, especially in poor responders. Human chorionic gonadotropin (HCG) is commonly used to induce LH surge and final oocyte maturation in IVF cycles for final follicular maturation (1).
One of these interventions in women with DOR is the augmentation of GnRH agonist into an HCG ampoule at final follicular maturation to improve final oocyte maturation in antagonist cycles. The possible mechanism is to mimic the physiological cycle and induce follicle-stimulating hormone (FSH) peak in the cycle and increase the number of mature oocytes (1, 2). In contrast, the HCG only induces the LH peak. However, the relevant studies reported contradictory findings, some of which have been applied in females with severe ovarian response to reduce the risk of ovarian hyperstimulation syndrome (1, 2). Numerous studies have been used in normal responders, and the number of oocytes and extent of pregnancy have increased in some of them (1-5). In a meta-analysis study on normal responders, the addition of agonists to HCG resulted in a significant improvement in the clinical pregnancy in antagonist cycles. However, the extent of pregnancy was not observed in other indices, such as the number of mature or fertilized oocytes (1).
However, fewer studies have been conducted on poor responders or were found to be associated with inconsistent findings. In the other 2 studies, there was no difference in dual ovarian stimulation or the GnRH agonist + HCG and HCG alone in normal and poor responders (1, 2), which may be due to lower doses of HCG in these 2 studies and fresh embryo transfer (ET). Studies have shown that final stimulation with agonists can reduce endometrial receptivity and the extent of pregnancy in fresh ET cycles. Due to low studies in poor responders, low oocyte counts, and low-quality oocytes and embryos despite high doses of gonadotropin hormone in IVF cycles, we decided to investigate the effect of final follicular stimulation with HCG agonist with HCG + GnRH compared to previous studies within a prospective study in the antagonist cycles on retrieved oocytes, mature oocytes and fetal counts, and good quality fetuses and clinical pregnancy in frozen cycles rather than fresh cycles in previous studies and abortion rates (3-6).
This prospective study seeks to clarify the role of dual triggering in poor responders, addressing gaps in existing literature by focusing on frozen cycles rather than fresh transfers, which may better preserve endometrial receptivity and improve pregnancy outcomes.
2. Materials and Methods
2.1. Study design and cases
The present single-blind randomized clinical trial was conducted on infertile women with diminished ovarian response referred to the Kosar Infertility Center, Imam Khomeini hospital, Sari, Iran, between May and November 2019 to initiate an intracytoplasmic sperm injection-ET cycle.
Inclusion criteria were women aged 20-45 yr, normal endometrium in hysterosalpingography, AMH levels < 1.1 ng/ml, antral follicle count < 7 in both ovaries, and prior < 3 failed IVF cycles. Women with normal ovarian response in ovulatory cycles were excluded from the study.
2.2. Intervention
Cases that met the inclusion criteria and demonstrated a poor ovarian response (antral follicle count < 7 or AMH level < 1.1 ng/ml), as confirmed by previous medical history, were consulted.
Women who have entered the IVF cycle were randomly assigned to each group and randomized based on the randomized block software.
Women were entered into each group by an IVF nurse, and the ultrasound operator was blind to the intervention.
All women who underwent the antagonist protocol for ovulation induction due to poor ovarian response and received daily 300 IU subcutaneous Cinnal‑F (75 IU/mL Follitropin alfa, CinnaGen Co., Iran) starting on day 3 of menstruation (based on age and ovarian reserve test results) were included in the study.
Upon follicle size of 12-14 mm, they received 250 µg of subcutaneous Cetrotide as GnRH antagonist (Cetrorelix acetate 0.25 mg, Merck Serono, Germany) daily, and folliculography and endometrial thickness examinations were routinely performed. The dose of gonadotropins was adjusted based on the size and number of follicles observed on ultrasound. When 2 or more follicles reached 17 mm or more in size, 10,000 units of intramuscular Choriomon (HCG 5000 IU, IBSA Co., Switzerland) and 0.2 mg of subcutaneous Variopeptyl® (Triptorelin acetate 0.1 mg), a GnRH agonist (Varian Pharmed Pharmaceutical Co., Iran) were injected. Then, oocyte retrieval was performed 34-36 hr later. In the next cycle, transplantation of 2 or 3 8-12-cell embryos was performed according to the age of the case, starting with oral estradiol 2 mg, 3 times daily, and serial transvaginal ultrasound (HONDA-2000, 7.5 megahertz) reaching an endometrium above 7 mm. In the HCG group, an intracytoplasmic sperm injection-ET cycle was performed with Chorimonas injection alone, and the cycle continued as mentioned earlier.
Luteal support was started in the frozen ET cycle after administration of 6 mg daily estradiol and reaching endometrial thickness above 7 mm, and 3 days before ET. The females received a single Cyclogest vaginal suppository (Progesterone 400 mg, Actover Inc., the UK) every 12 hr. The pregnancy test with blood β-HCG was estimated to be 15 days after ET. If tested positive, luteal support continued until 12 wk of gestation. If the pregnancy test was positive, the serial transvaginal ultrasound was performed 3-4 wk later to confirm gestational sac and clinical pregnancy.
2.3. Outcomes and data collection
The primary outcome of the study was the clinical pregnancy rate. This was assessed 4 wk after ET by transvaginal ultrasound performed by a qualified physician. The presence of a gestational sac was considered confirmation of clinical pregnancy.
The secondary outcomes included several parameters related to ovarian response, embryo development, and pregnancy progression. The oocyte recovery rate was evaluated 48 hr after administration of HCG. Oocytes were retrieved and examined under light microscopy by an experienced physician to determine the number and maturity of oocytes collected. Embryo development was assessed 3 days after oocyte retrieval. Embryos were cultured and evaluated microscopically, with the embryo rate calculated based on the proportion of fertilized oocytes that developed into cleavage-stage embryos.
Additional secondary outcomes included the miscarriage rate, which was monitored for up to 20 wk after ET. Miscarriage was defined as pregnancy loss prior to 20 wk of gestation and was confirmed by ultrasound examination. Oocyte quality was also assessed at the time of oocyte retrieval. Each oocyte was examined microscopically to determine morphological characteristics and maturity, providing an index of oocyte quality for each patient.
2.4. Sample size
The sample size was determined with reference to the study by Shapiro et al. which compared dual trigger (HCG + GnRH agonist) with HCG alone for final oocyte maturation in IVF cycles (7). Given the similarity in design, we adopted a sample size of 40 patients per group in the present study. To account for potential attrition, 82 women were recruited, ensuring that 80 participants (40 per group) remained for analysis.
For clinical outcomes (e.g., clinical pregnancy rate), the sample size was calculated using the formula for 2 independent proportions:
Where p1 = 0.82, p2 = 0.63, pˉ = (p1 + p2)/2, α = 0.05, and power 1-β = 0.80. This calculation indicates that approximately 85 participants per group would be required to detect a 19% absolute difference in clinical pregnancy rates with adequate power. Our study, with 40 per group, was therefore underpowered for clinical endpoints, which we acknowledge as a limitation.
For laboratory outcomes (e.g., number of metaphase II [MII] oocytes), the formula for 2 independent means was applied:
Where σ2 is the estimated variance and δ is the minimum clinically important difference. Assumptions for σ and δ were derived from pilot data and previous literature. Based on these assumptions, approximately 40 participants per group were sufficient to detect differences in laboratory outcomes with 80% power at α = 0.05.
To account for potential dropouts, 10% was added to the calculated sample size, resulting in a total recruitment of 82 women.
2.5. Ethical Considerations
This study may not benefit the individual; although evidence has shown that co-administration of GnRH agonist with HCG has been beneficial in final follicular stimulation for females with poor ovarian response, it is not harmful to the female. In accordance with ethical principles, written consent was obtained from all cases before entering the study. Complete and transparent information about the research process was given to the participants. The participants could freely leave the study at any stage of the project. All records were kept confidential. No cost was received from females at any stage of the study. The study began after receiving approval from the ethics committee on Biomedical Research at Imam Khomeini hospital, Sari, Iran (Code: IR.MAZUMS.IMAMHOSPITAL.REC.1398.006) and the Iranian Registry of Clinical Trials (IRCT20160815029374N4). The registration date was May 09, 2019, 1398/02/19 and the last date of updating the registry system is July 21, 2025, 1404/04/30.
2.6. Statistical Analysis
The statistical analysis was performed on both categorical and numerical data. Categorical variables (e.g., history of pregnancy and abortion) were presented as frequencies and percentages. Numerical variables (e.g., age, oocyte counts, embryo counts, and implantation rate) were expressed as mean ± standard deviation.
The normality of the distribution for all numerical variables was assessed using the Kolmogorov-Smirnov test. Based on the normality test results, intergroup comparisons were conducted using the Independent Samples t test for normally distributed data and the Mann-Whitney U test for non-normally distributed data. Comparisons of categorical variables between the groups were performed using the Chi-square test. A p < 0.050 was considered statistically significant for all analyses. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21.0 (Released 2012; IBM Corp., Armonk, NY, USA).
3. Results
A total of 82 infertile women were assessed for eligibility. 2 participants declined to participate, resulting in 80 women who were randomized into 2 groups of 40 each. All 80 participants received their allocated intervention and were included in the final analysis (Figure 1).
The baseline demographic and clinical characteristics of the participants are presented in table I. The 2 groups were comparable at baseline, with no statistically significant differences observed in age, history of pregnancy, or history of abortion (all p > 0.050). In the clinical pregnancy, the number of abortions in both groups are presented in table II.
As shown in table III, the mean number of total oocytes and mature oocytes (MII) was lower in the HCG group compared with the dual trigger group (HCG + GnRH agonist). Statistical analysis demonstrated a significant difference between the 2 groups for both total oocytes and MII oocytes (p ≤ 0.050). Similarly, the number of good-quality embryos was significantly higher in the dual trigger group than in the HCG group (p ≤ 0.050). This difference was reflected in the implantation rate, which was also significantly greater in the dual trigger group (p ≤ 0.050).
Although the clinical pregnancy rate appeared higher in the dual trigger group compared with the HCG group, the difference did not reach statistical significance (p > 0.050). Likewise, no significant difference was observed in abortion rates between the 2 groups, despite the absence of abortions in the dual trigger group.
4. Discussion
This study demonstrated that using a dual trigger (HCG + GnRH agonist) for final oocyte maturation significantly improved laboratory outcomes in women with DOR compared with HCG alone. The dual‑trigger group produced a higher number of total and MII oocytes, better‑quality embryos, and a superior implantation rate. These results align with earlier studies, reinforcing evidence that dual triggering can enhance oocyte maturation and embryo quality in poor responders (5, 8, 9-14).
The physiological basis for this improvement lies in the GnRH‑agonist-induced surge of both LH and FSH, mimicking the natural mid‑cycle hormonal peak more accurately than HCG alone, which elicits only an LH‑like response. The concurrent FSH surge facilitates optimal follicular maturation by upregulating gonadotropin receptors in granulosa cells, promoting cumulus expansion, and improving cytoplasmic maturation-all critical for oocyte competence and embryo viability (8, 11).
Several investigations have similarly reported an enhancement in oocyte and embryo parameters following dual triggering in this population (5, 9, 13, 15). For example, Chen et al. observed improved mature‑oocyte yield and embryo quality in women with DOR, while the 2025 meta‑analysis by Mercorio et al. confirmed the benefit of dual triggering among poor ovarian responders defined by both the Bologna and POSEIDON criteria (11).
However, clinical outcomes such as pregnancy and live‑birth rates remain inconsistent. Some studies, particularly smaller single‑center trials (10, 15), did not demonstrate statistically significant differences despite improved laboratory results. A 2023 meta‑analysis reported higher pregnancy rates in fresh cycles but considerable inter‑study variability (7). These discrepancies likely reflect differences in study design, patient selection, and limited sample sizes that reduce statistical power.
Variation in stimulation protocol and transfer strategy also contributes to heterogeneity. Trials performing fresh ET often reported reduced benefits, potentially because GnRH‑agonist use may impair endometrial receptivity. By contrast, our study employed frozen ET cycles, minimizing this effect and enabling transfer into a hormonally synchronized endometrium. Additionally, disparities in HCG dosage, timing of oocyte retrieval, and luteal‑phase support can influence clinical outcomes (16).
Collectively, available evidence suggests that while dual triggering consistently enhances laboratory indicators (notably oocyte maturity and embryo quality) the effect on clinical endpoints is less uniform and likely multifactorial, influenced by patient characteristics, protocol details, and study design. Future large, multicenter randomized controlled trials are warranted to delineate which subgroups of women with DOR derive the greatest clinical benefit (17, 18).
In summary, employing a dual trigger with GnRH agonist and HCG represents a promising and biologically sound approach for improving oocyte and embryo outcomes in women with DOR, potentially advancing IVF efficiency in this difficult‑to‑treat population.
Here is a condensed version of that text (approx. 220 words), focusing on clarity and flow:
While studies consistently show that dual triggering reliably improves laboratory outcomes (specifically oocyte maturation and embryo quality) its impact on clinical pregnancy and live-birth rates remains variable (5, 8, 11-13). Despite superior embryological yield, our study observed only a favorable trend, rather than statistical significance, in clinical pregnancy and miscarriage rates. This disconnect is well-documented; while oocyte yield and embryo quality are key, clinical success is multifactorial, depending on endometrial receptivity, transfer technique, luteal-phase support, and patient-specific factors such as age and comorbidities (4, 8, 11). Furthermore, DOR is itself associated with higher miscarriage risks, further complicating clinical outcomes (4).
The lack of statistical significance in our study likely reflects limitations in sample size and power, a common challenge in single-center trials focusing on poor responders (10, 15). Conversely, larger multi-center studies have reported significant improvements in clinical pregnancy and live-birth rates, underscoring the need for adequately powered trials to confirm these benefits (6, 11, 14, 18).
In conclusion, dual triggering is a promising strategy to enhance embryological outcomes in women with DOR. By producing more and higher-quality embryos, this approach optimizes the fertilization process and represents a practical advancement in treating this challenging patient population. Future large-scale randomized controlled trials are essential to definitively determine the long-term clinical impact and identify the specific subgroups that benefit most (6, 17, 18).
4.1. Strengths and Limitations
This study possesses several notable strengths. First, its design as a RCT minimizes selection bias and enhances the internal validity of the findings through random allocation of participants. Second, the focus on frozen ET cycles in women with DOR addresses a critical gap in the literature, as many prior studies utilized fresh transfers where GnRH agonist effects on endometrial receptivity may confound outcomes. Third, the use of a standardized, clinically relevant protocol improves the reproducibility and practical applicability of the results.
Several limitations should be considered. The single-center design and relatively small sample size limit the statistical power to detect differences in clinical outcomes such as pregnancy and live birth rates. The study also lacked long-term follow-up, preventing assessment of cumulative live birth rates or neonatal outcomes. Additionally, the homogeneous participant population may restrict generalizability to broader groups, such as those with obesity or other comorbidities. Finally, the absence of detailed cost-effectiveness analysis or data on patient-reported outcomes (e.g., treatment tolerability) represents an area for future research. Addressing these limitations in larger, multi-center trials would strengthen the evidence base.
5. Conclusion
Final oocyte maturation using dual ovarian stimulation with GnRH agonists and HCG improves the number of good-quality embryos and can be a practical approach to enhance the efficiency of the fertilization process in infertile women with DOR. Further research into larger sample sizes is needed to determine the specificity of the effect on quality of oocyte and the extent of pregnancy. Future research is suggested to investigate the effect of human GnRH agonist therapy and human gonadotropin on infertile women, with more underlying variables being assessed during the study and their correlation with the extent of pregnancy.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to ethical considerations and participant confidentiality. However, anonymized data may be made available upon reasonable requests from qualified researchers, subject to approval by the institutional ethics committee. Requests for data access should be directed to the corresponding author and will require a formal data sharing agreement to ensure compliance with ethical and legal standards. Any shared data will be stripped of identifiable information to protect participant privacy. For further inquiries, please contact manizheh.habibpour@yahoo.com.
Author Contributions
M. Zamaniyan: Conceptualization, methodology, supervision, writing-review and editing. T. Abbasi: Data curation, formal analysis, investigation, writing-original draft. M. Habibpour: Conceptualization, methodology, resources, supervision, writing-review and editing. S. Peyvandi: Conceptualization, methodology, resources, supervision, writing-review and editing. H. Jafarpour: Investigation, data curation. R.A. Mohammadpour Tahamtan: Formal analysis, software, validation. N. Gordani: Resources, project administration. Manizheh Habibpour and Sepideh Peyvandi are designated as co-corresponding authors. This is because the study involves interdisciplinary collaboration across laboratory sciences (MH's expertise) and clinical obstetrics/gynecology (SP's expertise), with both authors sharing equal responsibility for overseeing the research, responding to post-publication queries, managing data access requests, and handling correspondence with the journal and readers.
Acknowledgments
We thank the staff and colleagues at Mazandaran University of Medical Sciences and Sari Imam Khomeini hospital, Sari, Iran for their valuable support during this study. We are also grateful to the biostatistics consultant for assistance with data analysis and to the patients who participated generously. Without their cooperation and trust, this research would not have been possible. The authors declare that no Artificial Intelligence tools, including large language models or translation software, were used in the writing, revision, or data analysis of this manuscript.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Fertility & Infertility
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
