
International Journal of
Reproductive Biomedicine
Tue, Jun 23, 2026
[Archive]
Volume 24, Issue 4 (April 2026)
IJRM 2026, 24(4): 287-296 |
Back to browse issues page


Ethics code: E-30785963–020-220146
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Korkmaz O, Karabulut S, Yilmaz E, Delikara N. Clinician-related variability as an ındependent determinant of ın vitro fertilization success: A retrospective cohort study of ıntracytoplasmic sperm ınjection cycles. IJRM 2026; 24 (4) :287-296
URL: http://ijrm.ir/article-1-3712-en.html
URL: http://ijrm.ir/article-1-3712-en.html



1- Department of Histology and Embryology, Faculty of Medicine, Malatya Turgut Özal University, Malatya, Türkiye.
2- Department of Histology and Embryology, International Faculty of Medicine, Istanbul Medipol University, Istanbul, Türkiye. ,sedakarabulut@medipol.edu.tr
3- In Vitro Fertilization Center, Istanbul Medical Park Hospital, Istanbul, Türkiye.
4- In Vitro Fertilization Center, Istanbul Kadıköy Florence Nightingale Hospital, Istanbul, Türkiye.
2- Department of Histology and Embryology, International Faculty of Medicine, Istanbul Medipol University, Istanbul, Türkiye. ,
3- In Vitro Fertilization Center, Istanbul Medical Park Hospital, Istanbul, Türkiye.
4- In Vitro Fertilization Center, Istanbul Kadıköy Florence Nightingale Hospital, Istanbul, Türkiye.
Keywords: In vitro fertilization, Clinician performance, Pregnancy rate, Infertility treatment, Embryo transfer.
Full-Text [PDF 917 kb]
(157 Downloads)
| Abstract (HTML) (214 Views)
Full-Text: (18 Views)
1. Introduction
"Infertility, defined as the inability to achieve a clinical pregnancy after 12 months of regular, unprotected intercourse, affects an estimated 8-12% of couples of reproductive age worldwide" (1, 2). While the prevalence varies geographically, it remains a global public health concern with profound medical, psychological, and social consequences (3).
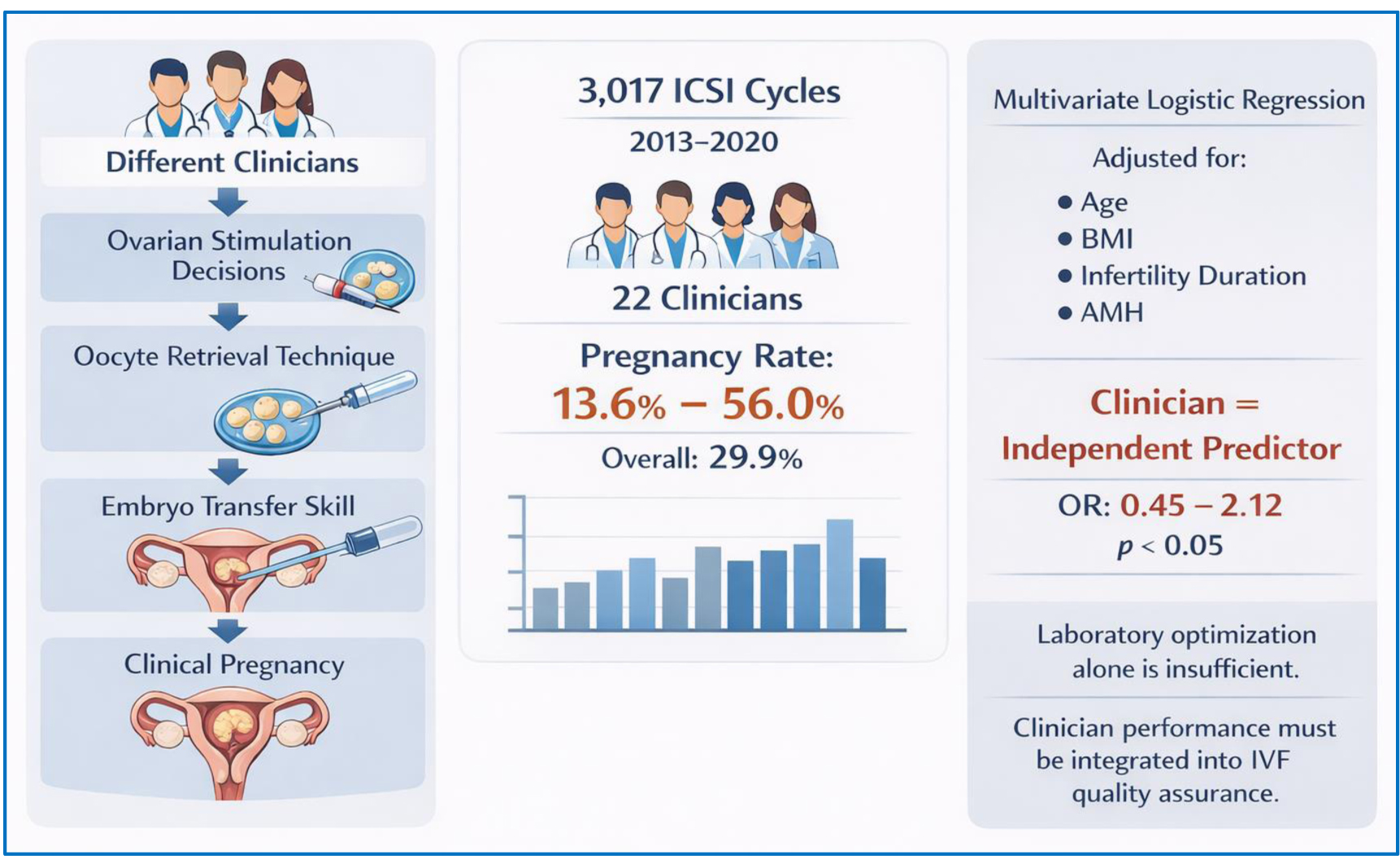
In vitro fertilization (IVF) is one of the most effective treatment strategies for infertility (4). Despite continuous advances in laboratory techniques and ovarian stimulation protocols, the average live birth rate per cycle remains around 20-35% (5). IVF outcomes are influenced by multiple variables that can be broadly categorized into 3 domains: 1) individual-related factors such as age, ovarian reserve, and sperm quality; 2) laboratory-related factors, including culture media, incubation conditions, and embryology techniques; and 3) clinic-related factors, particularly the expertise of healthcare professionals (6, 7).
Previous studies have primarily emphasized laboratory conditions and embryology practices as critical determinants of IVF success, including the role of skilled embryologists and optimized culture conditions, the importance of embryo culture media and environment, strict laboratory protocols such as vitrification and air quality control, as well as the implementation of key performance indicators (KPIs) to monitor technical and clinical quality (7). However, clinician-related variables have received considerably less attention. In practice, the clinician is directly responsible for protocol selection, medication dosing, stimulation monitoring, oocyte retrieval, and embryo transfer (ET), all of which are pivotal for treatment success. IVF protocols are complex and require intensive monitoring, with clinicians and embryologists responsible for several key decision points prior to and during the cycle.
Ovarian stimulation particularly requires numerous decisions regarding drug protocols, dosing, and timing tailored to each individual's profile, and individualized stimulation protocols enable clinicians to provide more accurate prognoses. Even when individuals and laboratory conditions are comparable, variations in clinician performance may lead to substantial differences in pregnancy outcomes. Clinical practice patterns and physician-related factors have been shown to influence treatment success beyond standardized laboratory procedures (8). Similarly, evidence indicates that even within high-performing IVF centers, variations in clinical decision-making can lead to measurable differences in outcomes (6). Furthermore, recent analyses highlight the importance of defining and monitoring KPIs to ensure clinical and embryological consistency and to minimize such variability (7).
The present study aimed to evaluate whether IVF pregnancy outcomes differ according to the clinician managing the treatment cycle. By comparing outcomes across multiple clinicians within the same IVF center, we sought to assess the independent contribution of clinician-related factors while minimizing variability from laboratory conditions.
2. Materials and Methods
2.1. Study population
In this retrospective cohort study, data of 3017 women who underwent intracytoplasmic sperm injection (ICSI) cycles at the IVF Centre of Kadıköy Florence Nightingale hospital, Istanbul, Türkiye, between January 2013 and December 2020, were extracted from their medical records and retrospectively reviewed.
2.2. Eligibility criteria
Inclusion criteria were defined as women aged between 18 and 45 yr with complete medical records, including maternal age, body mass index (BMI), infertility duration, anti-Müllerian hormone (AMH) levels, stimulation protocol, number of oocytes retrieved, and pregnancy outcome. Only cycles with fresh ET were included. Exclusion criteria were clinicians who had performed fewer than 10 ETs during the study period, cycles with incomplete clinical or laboratory data, donor oocyte cycles, cycles involving preimplantation genetic testing, and freeze-all cycles without subsequent ET. These criteria were applied to reduce heterogeneity and ensure reliable comparisons across clinicians.
2.3. Data collection and grouping
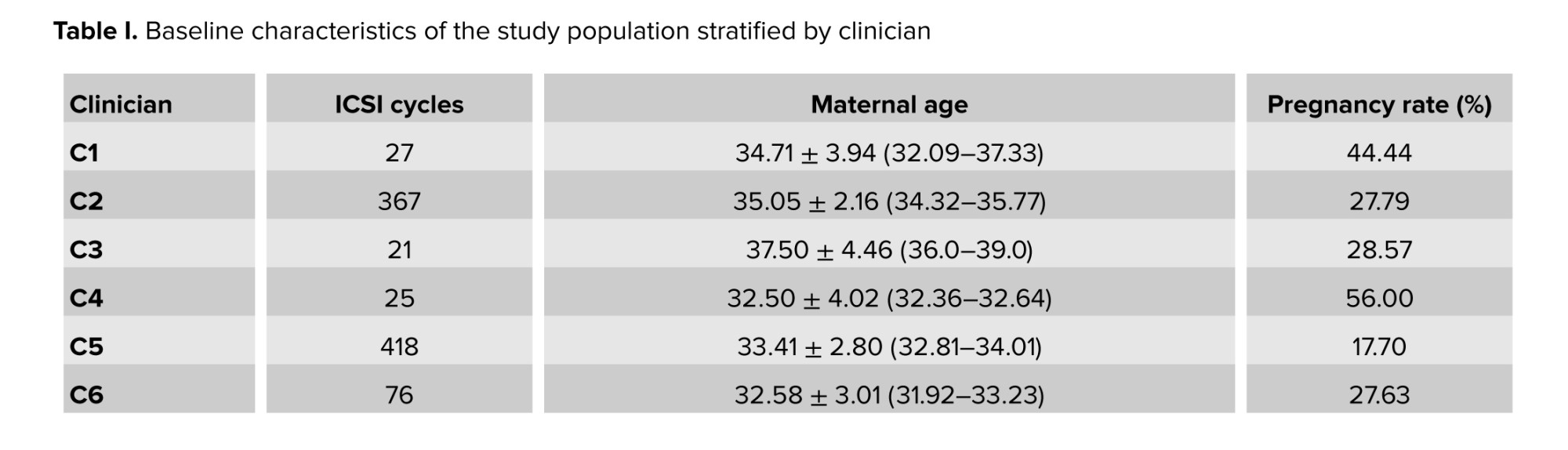
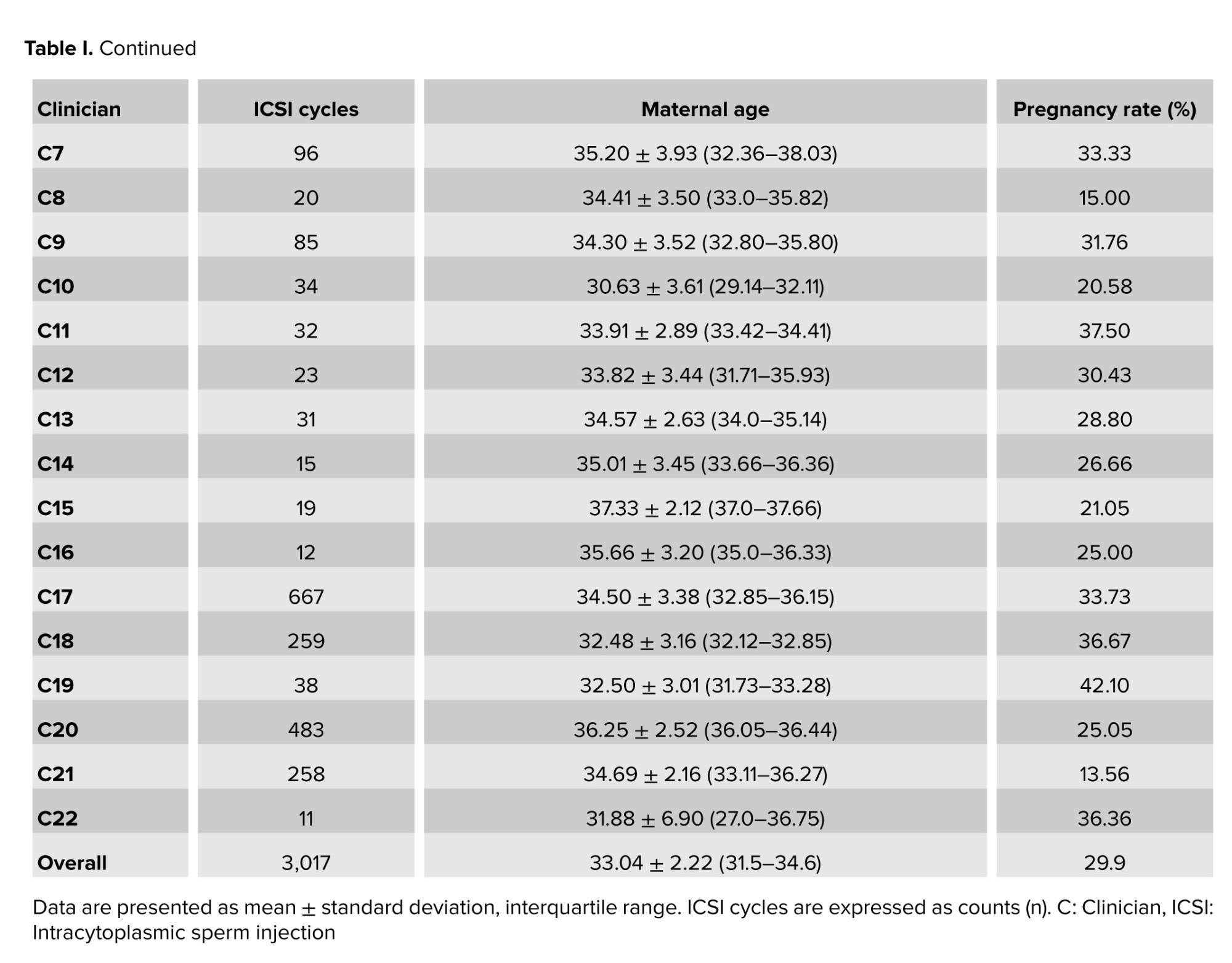
The following variables were extracted: maternal age, BMI, infertility duration, AMH, ovarian stimulation regimen, number of oocytes retrieved, number of embryos transferred, and pregnancy outcome. The primary outcome was clinical pregnancy, defined as the presence of a gestational sac on ultrasound. Individuals were grouped according to the clinician responsible for the ovarian stimulation protocol, oocyte retrieval, and ET. A total of 22 clinicians met the inclusion threshold (≥ 10 ETs).
2.4. Ethical Considerations
The study protocol was approved by the Non-Interventional Clinical Research Ethics Committee of Malatya Turgut Özal University, Malatya, Türkiye (Code: E-30785963-020-220146). Due to the retrospective nature of the study, the requirement for written informed consent was waived. The study was conducted in accordance with the principles of the Declaration of Helsinki and relevant institutional guidelines.
2.5. Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA) and R software, version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation, and categorical variables as frequencies and percentages. Normality of distributions was assessed using the Shapiro-Wilk test. Continuous variables were additionally summarized using median and interquartile range to enhance distributional reporting.
For comparisons between clinicians, categorical variables (e.g., pregnancy outcome) were analyzed using the Chi-square test. To account for potential confounding factors, a multivariate logistic regression model was constructed with clinical pregnancy (yes/no) as the dependent variable. Independent variables included clinician, maternal age, BMI, infertility duration, and AMH levels. Odds ratios (OR) with 95% confidence intervals (CI) were calculated. Results were considered statistically significant at a two-tailed p < 0.05. Data visualization, including bar plots and forest plots, was conducted in R using the ggplot2 and forestplot packages.
3. Results
Initially, 3412 ICSI cycles were reviewed; 395 cycles were excluded due to incomplete data (n = 120), donor oocyte use (n = 94), preimplantation genetic testing (n = 66), freeze-all strategy (n = 78), or clinicians performing < 10 ETs (n = 37).
3.1. Pregnancy rates across clinicians
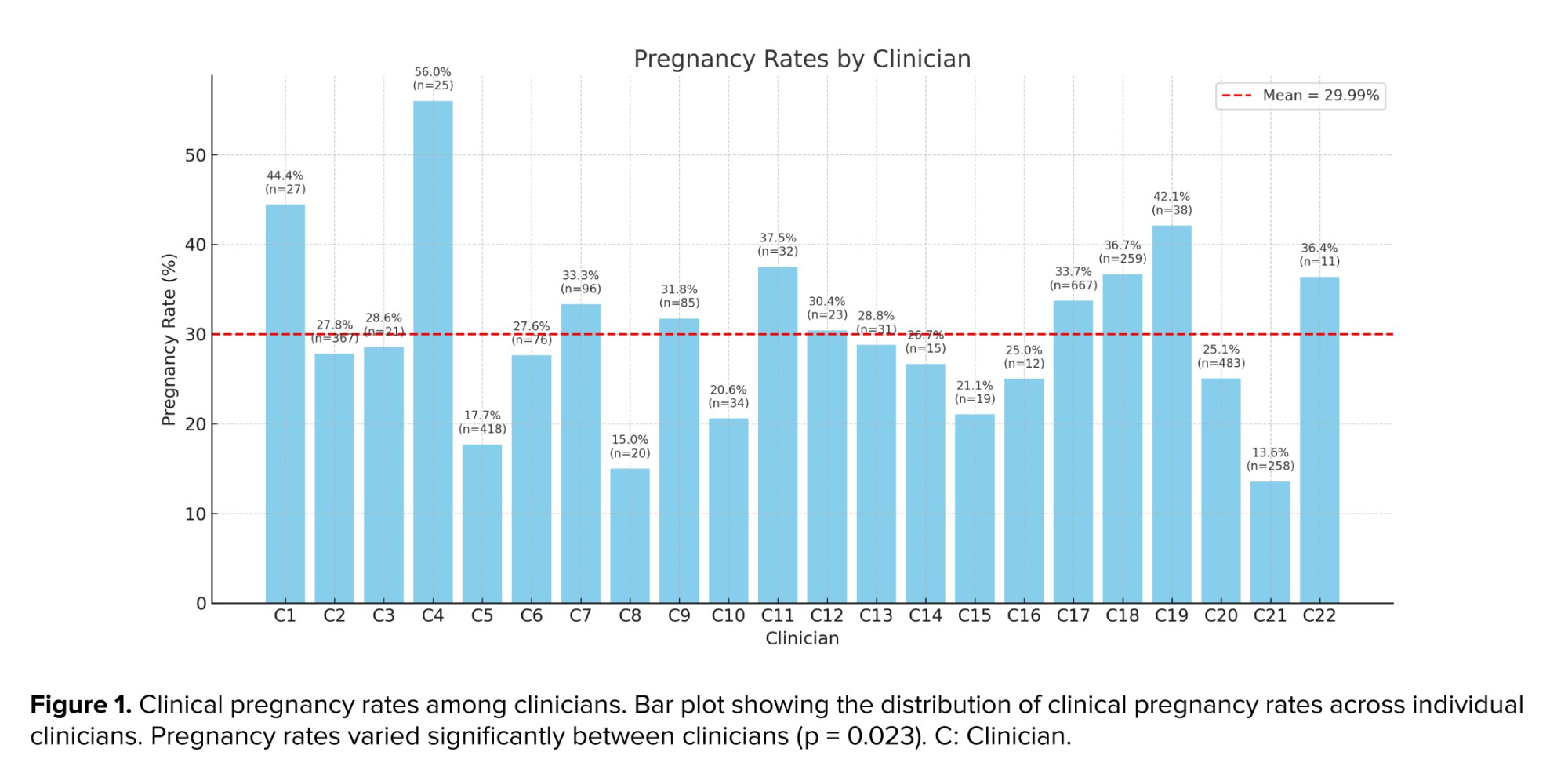
Clinical pregnancy rates varied considerably among clinicians, ranging from 13.6-56.0%, with an overall mean of 29.9% (Table I). Pregnancy rates across clinicians showed a median of 28.7% (interquartile range: 25.0-35.7).
Figure 1 illustrates the distribution of pregnancy rates across all clinicians. Although individual characteristics such as maternal age were comparable between groups, significant variability in outcomes was observed (p = 0.023).
The bar plot illustrates the clinical pregnancy rates achieved by 22 clinicians who performed ICSI cycles between 2013 and 2020. Each bar represents the percentage of clinical pregnancies per clinician, with the total number of cycles (n) indicated above the bars.
The red dashed line denotes the overall mean pregnancy rate across all clinicians (29.9%). Substantial variation in pregnancy outcomes was observed, ranging from 13.6-56.0%, despite comparable mean maternal ages across groups.
3.2. Multivariate analysis
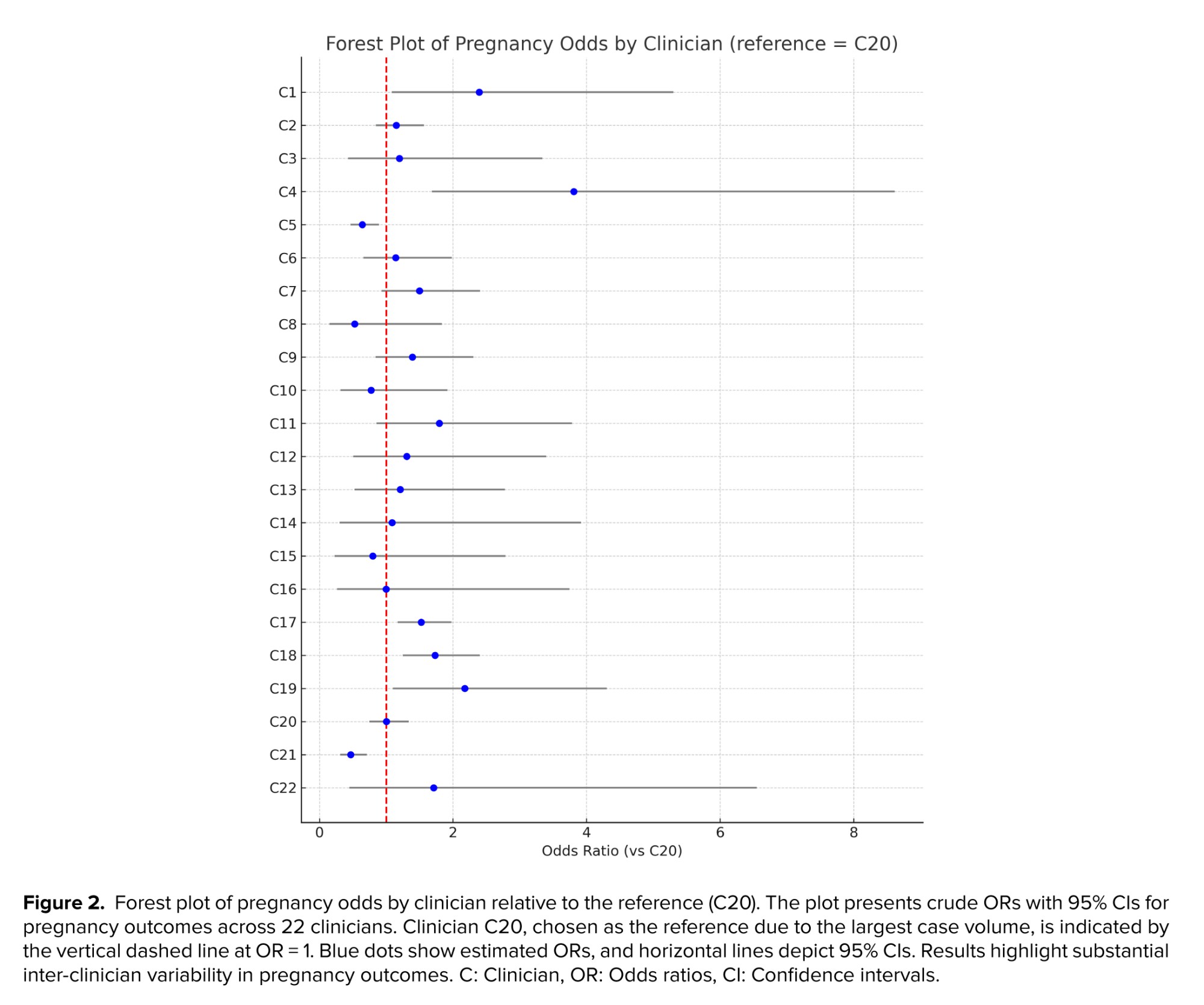
To evaluate whether these differences were attributable to clinician-related factors independent of individual characteristics, multivariate logistic regression analysis was performed. After adjusting for maternal age, BMI, infertility duration, and AMH levels, the clinician variable remained an independent predictor of pregnancy outcome (adjusted OR: 0.45-2.12, p = 0.018).
The forest plot in figure 2 presents the crude OR with 95% CI for pregnancy outcomes across clinicians, using clinician C20 as the reference due to the large number of cases performed. Several clinicians demonstrated significantly higher or lower odds of pregnancy compared with the reference, confirming that clinician-related variability substantially influenced IVF success.
4. Discussion
This retrospective cohort study demonstrated significant variability in clinical pregnancy rates among clinicians, even after adjustment for key confounding factors. These findings indicate that clinician-related factors independently influence IVF outcomes.
In the existing literature, operator-related variability in IVF outcomes has been examined mainly through the ET procedure, widely regarded as a critical determinant of implantation. Evidence shows that operator technique significantly affects clinical pregnancy rates, even when catheter type is standardized (9). Simulator-based studies highlight inter-physician variation (10), and reviews emphasize that ET success depends primarily on clinician performance (11). Guideline consensus also identifies ET as the pivotal final step for implantation (12). Early research demonstrated that catheter type and ultrasound guidance influence implantation, with soft catheters yielding higher pregnancy rates than rigid ones (13, 14). Systematic reviews further confirm that soft catheters improve implantation and that ultrasound-guided transfers enhance both implantation and ongoing pregnancy rates (15).
Several randomized and observational studies support the superiority of ultrasound-guided ET over the clinical touch method. A randomized trial showed higher pregnancy (26.3% vs. 18.1%; p < 0.05) and implantation rates (11.1% vs. 7.5%; p < 0.05) with ultrasound guidance (16). A cochrane meta-analysis of more than 6,000 women similarly reported increased odds of ongoing/live birth (OR: 1.47, 95% CI: 1.30-1.65) and clinical pregnancy (OR: 1.31, 95% CI: 1.17-1.45). Another study found substantially higher pregnancy rates with ultrasound-guided transfers (50% vs. 33.7%; p < 0.002) (17). Technical factors can also influence outcomes. Blood contamination on the catheter is associated with reduced implantation and clinical pregnancy rates (18, 19), while mucus contamination appears to have no adverse effect (19). Uterine contractions and the depth of embryo deposition may further modulate implantation success, with placement 10-15 mm below the fundus associated with superior outcomes (14, 20).
Consistent with these findings, a large retrospective analysis of 19,824 ETs showed that operator-related factors accounted for almost half of the variability in ongoing pregnancy rates, indicating that experience alone does not ensure proficiency (21). Simulator-based research likewise demonstrated considerable differences in technique among clinicians, with performance metrics correlating with live birth outcomes (10). A comprehensive review further highlighted that ET success is principally driven by clinician performance (11).
Beyond ET, multiple studies underscore the essential contribution of embryologists to IVF success. Increased embryologist experience and technical proficiency, particularly after extensive ICSI practice, are linked to higher fertilization rates, improved blastocyst development, and increased implantation (22). The specific embryologist performing the procedure may independently influence ongoing pregnancy after adjusting for confounders (23). Team-based laboratory coordination and individual-centered workflow management further enhance outcomes (24). Laboratory-related determinants such as accurate embryo grading (25), optimized gamete handling with buffered media (26), and the maintenance of stable culture temperatures (27) also affect fertilization and implantation potential.
Quality assurance systems have been widely implemented to monitor embryologist performance. A recent consensus defined 3 categories of indicators for IVF laboratories: KPIs, performance indicators, and recommendation indicators, integrating both clinical and embryological monitoring (7). Structured evaluation and quality assurance frameworks using KPIs have been recommended to maintain high laboratory standards (28). Artificial intelligence-based monitoring systems also track embryology staff performance effectively, underscoring the benefits of continuous quality assessment (29). However, far fewer studies have applied similar scrutiny to the clinical side of IVF practice, despite clinicians being responsible for numerous decisions and procedures that precede and accompany laboratory work.
Our findings extend previous research by demonstrating that clinician-related factors influence IVF outcomes across the entire treatment cycle, not only during ET. Decisions regarding ovarian stimulation, gonadotropin dosing, monitoring schedules, and trigger timing directly affect oocyte number and quality. Technical proficiency during oocyte retrieval shapes both oocyte yield and integrity, influencing subsequent fertilization and embryo development (30). Although ET remains essential, the variability observed among clinicians likely reflects the cumulative effect of multiple clinical actions rather than a single procedural step.
These results highlight the clinician as a key determinant of IVF success alongside individuals and laboratory factors. While embryologist-related variables are well standardized, clinician variability has received limited attention. Incorporating clinician performance into IVF quality assurance systems as a measurable component may help address this gap.
Several mechanisms contribute to this variability. Technical aspects such as follicular aspiration, minimizing trauma, and precise embryo deposition affect implantation potential. Clinical judgment in tailoring stimulation protocols, determining trigger timing, and adjusting medications is also crucial. Beyond procedural skills, effective clinician-individual communication, evidence-based practice, and coordination with embryology staff may enhance outcomes by improving compliance and workflow.
Structured training programs emphasizing procedural competency and individualized treatment planning may reduce variability. Routine performance monitoring and audits can identify deviations from best practice, while mentorship systems may minimize operator-related disparities. Incorporating clinician-specific quality indicators into accreditation frameworks could strengthen transparency in IVF centers.
Limitations include its retrospective single-center design and lack of full standardization for factors such as endometrial thickness, embryo grading, and stimulation protocol heterogeneity details. Clinical pregnancy, rather than live birth, was used as the outcome measure, and clinician case volume varied. Retrospective design also prevented systematic evaluation of embryologist-related variables, limiting assessment of their influence. Prospective multicenter studies with rigorous standardization are needed to isolate the independent effect of the clinician.
Future research should validate these findings using live birth as the primary endpoint. Identifying which aspects of clinician practice most influence outcomes and applying simulation-based training, artificaial inteligence-assisted decision systems, and standardized procedures may help reduce inter-clinician variability. Expanding IVF quality frameworks to include clinician performance could improve treatment success.
5. Conclusion
This study demonstrates that clinician-related factors are independent and significant determinants of IVF success. Pregnancy outcomes varied considerably among clinicians, even after adjusting for maternal age, BMI, infertility duration, and AMH levels. These findings highlight that clinical expertise, decision-making, and procedural skills exert a measurable influence on treatment results throughout the entire IVF cycle, not only during ET.
Improving laboratory conditions alone is insufficient to optimize IVF outcomes. Equal emphasis must be placed on clinician training, performance standardization, and continuous professional development. Incorporating clinician-related metrics into quality assurance programs and promoting structured mentorship may help reduce variability and improve individual care. Future prospective multicenter studies are warranted to confirm these results and to identify the specific components of clinical practice that most strongly impact IVF success.
Data Availability
Data that support the results of this study can be obtained from the corresponding author upon reasonable request.
Author Contributions
O. Korkmaz and S. Karabulut had full access to all study data and assumed responsibility for its integrity and the accuracy of the analyses, including study conceptualization and design. E. Yilmaz and N. Delikara contributed to data acquisition, analysis, and interpretation. O. Korkmaz and S. Karabulut prepared the initial draft of the manuscript and performed the statistical analyses. All authors critically revised the manuscript for important intellectual content, approved the final version, and accepted responsibility for the integrity of the work.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. During manuscript preparation, artificial intelligence-based tools (Grok version 4.1, xAI) were employed for language editing support. All content, analyses, and conclusions were generated and verified by the authors.
Conflict of Interest
The authors declare that there is no conflict of interest.
"Infertility, defined as the inability to achieve a clinical pregnancy after 12 months of regular, unprotected intercourse, affects an estimated 8-12% of couples of reproductive age worldwide" (1, 2). While the prevalence varies geographically, it remains a global public health concern with profound medical, psychological, and social consequences (3).
In vitro fertilization (IVF) is one of the most effective treatment strategies for infertility (4). Despite continuous advances in laboratory techniques and ovarian stimulation protocols, the average live birth rate per cycle remains around 20-35% (5). IVF outcomes are influenced by multiple variables that can be broadly categorized into 3 domains: 1) individual-related factors such as age, ovarian reserve, and sperm quality; 2) laboratory-related factors, including culture media, incubation conditions, and embryology techniques; and 3) clinic-related factors, particularly the expertise of healthcare professionals (6, 7).
Previous studies have primarily emphasized laboratory conditions and embryology practices as critical determinants of IVF success, including the role of skilled embryologists and optimized culture conditions, the importance of embryo culture media and environment, strict laboratory protocols such as vitrification and air quality control, as well as the implementation of key performance indicators (KPIs) to monitor technical and clinical quality (7). However, clinician-related variables have received considerably less attention. In practice, the clinician is directly responsible for protocol selection, medication dosing, stimulation monitoring, oocyte retrieval, and embryo transfer (ET), all of which are pivotal for treatment success. IVF protocols are complex and require intensive monitoring, with clinicians and embryologists responsible for several key decision points prior to and during the cycle.
Ovarian stimulation particularly requires numerous decisions regarding drug protocols, dosing, and timing tailored to each individual's profile, and individualized stimulation protocols enable clinicians to provide more accurate prognoses. Even when individuals and laboratory conditions are comparable, variations in clinician performance may lead to substantial differences in pregnancy outcomes. Clinical practice patterns and physician-related factors have been shown to influence treatment success beyond standardized laboratory procedures (8). Similarly, evidence indicates that even within high-performing IVF centers, variations in clinical decision-making can lead to measurable differences in outcomes (6). Furthermore, recent analyses highlight the importance of defining and monitoring KPIs to ensure clinical and embryological consistency and to minimize such variability (7).
The present study aimed to evaluate whether IVF pregnancy outcomes differ according to the clinician managing the treatment cycle. By comparing outcomes across multiple clinicians within the same IVF center, we sought to assess the independent contribution of clinician-related factors while minimizing variability from laboratory conditions.
2. Materials and Methods
2.1. Study population
In this retrospective cohort study, data of 3017 women who underwent intracytoplasmic sperm injection (ICSI) cycles at the IVF Centre of Kadıköy Florence Nightingale hospital, Istanbul, Türkiye, between January 2013 and December 2020, were extracted from their medical records and retrospectively reviewed.
2.2. Eligibility criteria
Inclusion criteria were defined as women aged between 18 and 45 yr with complete medical records, including maternal age, body mass index (BMI), infertility duration, anti-Müllerian hormone (AMH) levels, stimulation protocol, number of oocytes retrieved, and pregnancy outcome. Only cycles with fresh ET were included. Exclusion criteria were clinicians who had performed fewer than 10 ETs during the study period, cycles with incomplete clinical or laboratory data, donor oocyte cycles, cycles involving preimplantation genetic testing, and freeze-all cycles without subsequent ET. These criteria were applied to reduce heterogeneity and ensure reliable comparisons across clinicians.
2.3. Data collection and grouping
The following variables were extracted: maternal age, BMI, infertility duration, AMH, ovarian stimulation regimen, number of oocytes retrieved, number of embryos transferred, and pregnancy outcome. The primary outcome was clinical pregnancy, defined as the presence of a gestational sac on ultrasound. Individuals were grouped according to the clinician responsible for the ovarian stimulation protocol, oocyte retrieval, and ET. A total of 22 clinicians met the inclusion threshold (≥ 10 ETs).
2.4. Ethical Considerations
The study protocol was approved by the Non-Interventional Clinical Research Ethics Committee of Malatya Turgut Özal University, Malatya, Türkiye (Code: E-30785963-020-220146). Due to the retrospective nature of the study, the requirement for written informed consent was waived. The study was conducted in accordance with the principles of the Declaration of Helsinki and relevant institutional guidelines.
2.5. Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA) and R software, version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation, and categorical variables as frequencies and percentages. Normality of distributions was assessed using the Shapiro-Wilk test. Continuous variables were additionally summarized using median and interquartile range to enhance distributional reporting.
For comparisons between clinicians, categorical variables (e.g., pregnancy outcome) were analyzed using the Chi-square test. To account for potential confounding factors, a multivariate logistic regression model was constructed with clinical pregnancy (yes/no) as the dependent variable. Independent variables included clinician, maternal age, BMI, infertility duration, and AMH levels. Odds ratios (OR) with 95% confidence intervals (CI) were calculated. Results were considered statistically significant at a two-tailed p < 0.05. Data visualization, including bar plots and forest plots, was conducted in R using the ggplot2 and forestplot packages.
3. Results
Initially, 3412 ICSI cycles were reviewed; 395 cycles were excluded due to incomplete data (n = 120), donor oocyte use (n = 94), preimplantation genetic testing (n = 66), freeze-all strategy (n = 78), or clinicians performing < 10 ETs (n = 37).
3.1. Pregnancy rates across clinicians
Clinical pregnancy rates varied considerably among clinicians, ranging from 13.6-56.0%, with an overall mean of 29.9% (Table I). Pregnancy rates across clinicians showed a median of 28.7% (interquartile range: 25.0-35.7).
Figure 1 illustrates the distribution of pregnancy rates across all clinicians. Although individual characteristics such as maternal age were comparable between groups, significant variability in outcomes was observed (p = 0.023).
The bar plot illustrates the clinical pregnancy rates achieved by 22 clinicians who performed ICSI cycles between 2013 and 2020. Each bar represents the percentage of clinical pregnancies per clinician, with the total number of cycles (n) indicated above the bars.
The red dashed line denotes the overall mean pregnancy rate across all clinicians (29.9%). Substantial variation in pregnancy outcomes was observed, ranging from 13.6-56.0%, despite comparable mean maternal ages across groups.
3.2. Multivariate analysis
To evaluate whether these differences were attributable to clinician-related factors independent of individual characteristics, multivariate logistic regression analysis was performed. After adjusting for maternal age, BMI, infertility duration, and AMH levels, the clinician variable remained an independent predictor of pregnancy outcome (adjusted OR: 0.45-2.12, p = 0.018).
The forest plot in figure 2 presents the crude OR with 95% CI for pregnancy outcomes across clinicians, using clinician C20 as the reference due to the large number of cases performed. Several clinicians demonstrated significantly higher or lower odds of pregnancy compared with the reference, confirming that clinician-related variability substantially influenced IVF success.
4. Discussion
This retrospective cohort study demonstrated significant variability in clinical pregnancy rates among clinicians, even after adjustment for key confounding factors. These findings indicate that clinician-related factors independently influence IVF outcomes.
In the existing literature, operator-related variability in IVF outcomes has been examined mainly through the ET procedure, widely regarded as a critical determinant of implantation. Evidence shows that operator technique significantly affects clinical pregnancy rates, even when catheter type is standardized (9). Simulator-based studies highlight inter-physician variation (10), and reviews emphasize that ET success depends primarily on clinician performance (11). Guideline consensus also identifies ET as the pivotal final step for implantation (12). Early research demonstrated that catheter type and ultrasound guidance influence implantation, with soft catheters yielding higher pregnancy rates than rigid ones (13, 14). Systematic reviews further confirm that soft catheters improve implantation and that ultrasound-guided transfers enhance both implantation and ongoing pregnancy rates (15).
Several randomized and observational studies support the superiority of ultrasound-guided ET over the clinical touch method. A randomized trial showed higher pregnancy (26.3% vs. 18.1%; p < 0.05) and implantation rates (11.1% vs. 7.5%; p < 0.05) with ultrasound guidance (16). A cochrane meta-analysis of more than 6,000 women similarly reported increased odds of ongoing/live birth (OR: 1.47, 95% CI: 1.30-1.65) and clinical pregnancy (OR: 1.31, 95% CI: 1.17-1.45). Another study found substantially higher pregnancy rates with ultrasound-guided transfers (50% vs. 33.7%; p < 0.002) (17). Technical factors can also influence outcomes. Blood contamination on the catheter is associated with reduced implantation and clinical pregnancy rates (18, 19), while mucus contamination appears to have no adverse effect (19). Uterine contractions and the depth of embryo deposition may further modulate implantation success, with placement 10-15 mm below the fundus associated with superior outcomes (14, 20).
Consistent with these findings, a large retrospective analysis of 19,824 ETs showed that operator-related factors accounted for almost half of the variability in ongoing pregnancy rates, indicating that experience alone does not ensure proficiency (21). Simulator-based research likewise demonstrated considerable differences in technique among clinicians, with performance metrics correlating with live birth outcomes (10). A comprehensive review further highlighted that ET success is principally driven by clinician performance (11).
Beyond ET, multiple studies underscore the essential contribution of embryologists to IVF success. Increased embryologist experience and technical proficiency, particularly after extensive ICSI practice, are linked to higher fertilization rates, improved blastocyst development, and increased implantation (22). The specific embryologist performing the procedure may independently influence ongoing pregnancy after adjusting for confounders (23). Team-based laboratory coordination and individual-centered workflow management further enhance outcomes (24). Laboratory-related determinants such as accurate embryo grading (25), optimized gamete handling with buffered media (26), and the maintenance of stable culture temperatures (27) also affect fertilization and implantation potential.
Quality assurance systems have been widely implemented to monitor embryologist performance. A recent consensus defined 3 categories of indicators for IVF laboratories: KPIs, performance indicators, and recommendation indicators, integrating both clinical and embryological monitoring (7). Structured evaluation and quality assurance frameworks using KPIs have been recommended to maintain high laboratory standards (28). Artificial intelligence-based monitoring systems also track embryology staff performance effectively, underscoring the benefits of continuous quality assessment (29). However, far fewer studies have applied similar scrutiny to the clinical side of IVF practice, despite clinicians being responsible for numerous decisions and procedures that precede and accompany laboratory work.
Our findings extend previous research by demonstrating that clinician-related factors influence IVF outcomes across the entire treatment cycle, not only during ET. Decisions regarding ovarian stimulation, gonadotropin dosing, monitoring schedules, and trigger timing directly affect oocyte number and quality. Technical proficiency during oocyte retrieval shapes both oocyte yield and integrity, influencing subsequent fertilization and embryo development (30). Although ET remains essential, the variability observed among clinicians likely reflects the cumulative effect of multiple clinical actions rather than a single procedural step.
These results highlight the clinician as a key determinant of IVF success alongside individuals and laboratory factors. While embryologist-related variables are well standardized, clinician variability has received limited attention. Incorporating clinician performance into IVF quality assurance systems as a measurable component may help address this gap.
Several mechanisms contribute to this variability. Technical aspects such as follicular aspiration, minimizing trauma, and precise embryo deposition affect implantation potential. Clinical judgment in tailoring stimulation protocols, determining trigger timing, and adjusting medications is also crucial. Beyond procedural skills, effective clinician-individual communication, evidence-based practice, and coordination with embryology staff may enhance outcomes by improving compliance and workflow.
Structured training programs emphasizing procedural competency and individualized treatment planning may reduce variability. Routine performance monitoring and audits can identify deviations from best practice, while mentorship systems may minimize operator-related disparities. Incorporating clinician-specific quality indicators into accreditation frameworks could strengthen transparency in IVF centers.
Limitations include its retrospective single-center design and lack of full standardization for factors such as endometrial thickness, embryo grading, and stimulation protocol heterogeneity details. Clinical pregnancy, rather than live birth, was used as the outcome measure, and clinician case volume varied. Retrospective design also prevented systematic evaluation of embryologist-related variables, limiting assessment of their influence. Prospective multicenter studies with rigorous standardization are needed to isolate the independent effect of the clinician.
Future research should validate these findings using live birth as the primary endpoint. Identifying which aspects of clinician practice most influence outcomes and applying simulation-based training, artificaial inteligence-assisted decision systems, and standardized procedures may help reduce inter-clinician variability. Expanding IVF quality frameworks to include clinician performance could improve treatment success.
5. Conclusion
This study demonstrates that clinician-related factors are independent and significant determinants of IVF success. Pregnancy outcomes varied considerably among clinicians, even after adjusting for maternal age, BMI, infertility duration, and AMH levels. These findings highlight that clinical expertise, decision-making, and procedural skills exert a measurable influence on treatment results throughout the entire IVF cycle, not only during ET.
Improving laboratory conditions alone is insufficient to optimize IVF outcomes. Equal emphasis must be placed on clinician training, performance standardization, and continuous professional development. Incorporating clinician-related metrics into quality assurance programs and promoting structured mentorship may help reduce variability and improve individual care. Future prospective multicenter studies are warranted to confirm these results and to identify the specific components of clinical practice that most strongly impact IVF success.
Data Availability
Data that support the results of this study can be obtained from the corresponding author upon reasonable request.
Author Contributions
O. Korkmaz and S. Karabulut had full access to all study data and assumed responsibility for its integrity and the accuracy of the analyses, including study conceptualization and design. E. Yilmaz and N. Delikara contributed to data acquisition, analysis, and interpretation. O. Korkmaz and S. Karabulut prepared the initial draft of the manuscript and performed the statistical analyses. All authors critically revised the manuscript for important intellectual content, approved the final version, and accepted responsibility for the integrity of the work.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. During manuscript preparation, artificial intelligence-based tools (Grok version 4.1, xAI) were employed for language editing support. All content, analyses, and conclusions were generated and verified by the authors.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Biology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
