
International Journal of
Reproductive Biomedicine
Mon, Aug 3, 2026
[Archive]
Volume 24, Issue 3 (March 2026)
IJRM 2026, 24(3): 219-230 |
Back to browse issues page


Ethics code: IR.SUMS.REC.1399.922
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
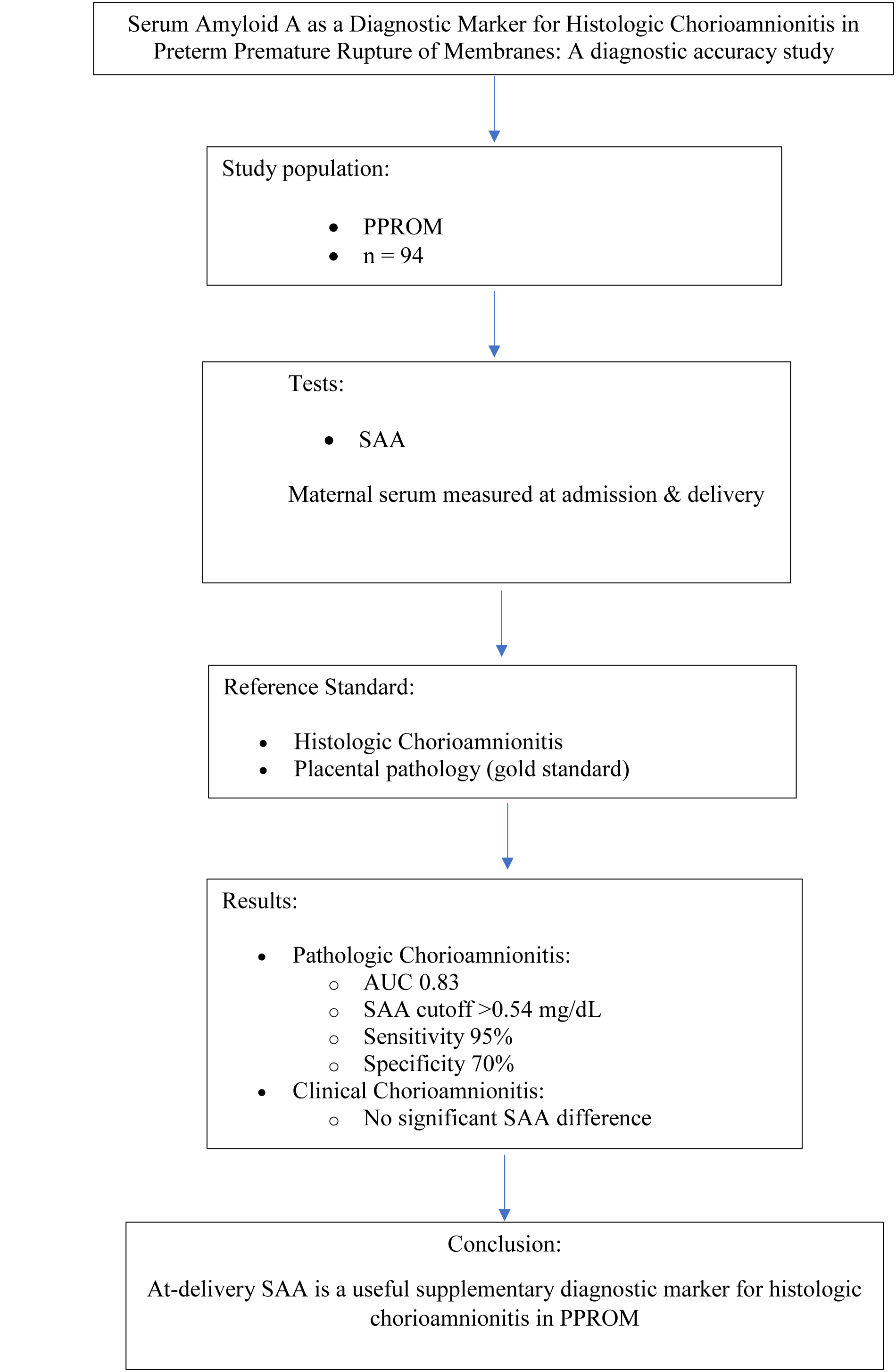
Faraji A, Mehraban M, Kasraeian M, Akbarzadeh-Jahromi M, Vafaei H, Asadi N, et al . Serum amyloid A as a diagnostic marker for histologic chorioamnionitis in preterm premature rupture of membranes: A diagnostic accuracy study. IJRM 2026; 24 (3) :219-230
URL: http://ijrm.ir/article-1-3515-en.html
URL: http://ijrm.ir/article-1-3515-en.html
Azam Faraji1 

 , Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
, Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
, Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
1- Maternal-Fetal Medicine Research Center, Department of Obstetrics and Gynecology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Pathology Department, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran. & Maternal-Fetal Medicine Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Department of Public Health, Khalkhal University of Medical Sciences, Khalkhal, Iran. ,marjan.zare@gmail.com; mar.zare@khalums.ac.ir
2- Pathology Department, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran. & Maternal-Fetal Medicine Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Department of Public Health, Khalkhal University of Medical Sciences, Khalkhal, Iran. ,
Abstract: (347 Views)
Background: Chorioamnionitis is an acute inflammation of the fetal membrane in mothers with preterm premature rupture of the membrane (PPROM). The diagnosis of chorioamnionitis is based on clinical findings; however, laboratory tests may help diagnose the disease.
Objective: It aimed to evaluate the accuracy of maternal serum-amyloid A (SAA) protein levels in diagnosing histopathologic chorioamnionitis following PPROM mothers; secondarily, it assessed their accuracy for diagnosing clinical chorioamnionitis.
Materials and Methods: In this diagnostic accuracy study, 94 PPROM pregnancies, referred to Namazi, Hafez, and Zeinabiyeh hospitals, Shiraz, Iran, from March 2022 to March 2023 were followed. All placentas were examined for histopathological evidence of chorioamnionitis, and participants were classified into 2 pathologic chorioamnionitis and normal placenta groups.
Results: From the 94 participants, 50 (43.20%) were pathologically diagnosed with chorioamnionitis as pathologic chorioamnionitis group, and the remaining 44 (46.80%) belonged to control “normal placenta group”. In addition, 50% (25/50) of women with pathological chorioamnionitis were clinically diagnosed with chorioamnionitis as clinic chorioamnionitis group, and the remaining 50% (25/50) with no clinical signs of chorioamnionitis belonged to their control. Pathologic at-delivery SAA were more in the pathologic chorioamnionitis group compared with normal placenta group; adjusted odds ratio (95% confidence interval); 15.20 (2.62-88.20); the area under curve values (cutoff point, sensitivity, specificity, negative predictive value, positive predictive value, and accuracy) were 0.83 (> 0.54 mg/dl, 95%, 70%, 86%, 88%, and 84%) for pathologic at-delivery SAA. However, clinic at-delivery SAA did not significantly change between clinic chorioamnionitis group and not having clinic chorioamnionitis. A no-clinic chorioamnionitis PPROM mother could be chorioamnionitis one by a 50% chance, even with no clinical sign.
Conclusion: Pathologic at-delivery SAA level could be a supplementary test in PPROM mothers. At-delivery SAA serial measurements and long-term evaluation of infants born to these mothers are recommended.
Objective: It aimed to evaluate the accuracy of maternal serum-amyloid A (SAA) protein levels in diagnosing histopathologic chorioamnionitis following PPROM mothers; secondarily, it assessed their accuracy for diagnosing clinical chorioamnionitis.
Materials and Methods: In this diagnostic accuracy study, 94 PPROM pregnancies, referred to Namazi, Hafez, and Zeinabiyeh hospitals, Shiraz, Iran, from March 2022 to March 2023 were followed. All placentas were examined for histopathological evidence of chorioamnionitis, and participants were classified into 2 pathologic chorioamnionitis and normal placenta groups.
Results: From the 94 participants, 50 (43.20%) were pathologically diagnosed with chorioamnionitis as pathologic chorioamnionitis group, and the remaining 44 (46.80%) belonged to control “normal placenta group”. In addition, 50% (25/50) of women with pathological chorioamnionitis were clinically diagnosed with chorioamnionitis as clinic chorioamnionitis group, and the remaining 50% (25/50) with no clinical signs of chorioamnionitis belonged to their control. Pathologic at-delivery SAA were more in the pathologic chorioamnionitis group compared with normal placenta group; adjusted odds ratio (95% confidence interval); 15.20 (2.62-88.20); the area under curve values (cutoff point, sensitivity, specificity, negative predictive value, positive predictive value, and accuracy) were 0.83 (> 0.54 mg/dl, 95%, 70%, 86%, 88%, and 84%) for pathologic at-delivery SAA. However, clinic at-delivery SAA did not significantly change between clinic chorioamnionitis group and not having clinic chorioamnionitis. A no-clinic chorioamnionitis PPROM mother could be chorioamnionitis one by a 50% chance, even with no clinical sign.
Conclusion: Pathologic at-delivery SAA level could be a supplementary test in PPROM mothers. At-delivery SAA serial measurements and long-term evaluation of infants born to these mothers are recommended.
Type of Study: Original Article |
Subject:
Reproductive Pattology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
