
International Journal of
Reproductive Biomedicine
Tue, Aug 4, 2026
[Archive]
Volume 24, Issue 3 (March 2026)
IJRM 2026, 24(3): 219-230 |
Back to browse issues page


Ethics code: IR.SUMS.REC.1399.922
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Faraji A, Mehraban M, Kasraeian M, Akbarzadeh-Jahromi M, Vafaei H, Asadi N, et al . Serum amyloid A as a diagnostic marker for histologic chorioamnionitis in preterm premature rupture of membranes: A diagnostic accuracy study. IJRM 2026; 24 (3) :219-230
URL: http://ijrm.ir/article-1-3515-en.html
URL: http://ijrm.ir/article-1-3515-en.html
Azam Faraji1 

 , Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
, Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
, Mitra Mehraban1 , Maryam Kasraeian1 , Mojgan Akbarzadeh-Jahromi2 , Homeira Vafaei1 , Nasrin Asadi1 , Zahra Oveisi1 , Marzieh Kasraie1 , Marjan Zare *3
1- Maternal-Fetal Medicine Research Center, Department of Obstetrics and Gynecology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Pathology Department, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran. & Maternal-Fetal Medicine Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Department of Public Health, Khalkhal University of Medical Sciences, Khalkhal, Iran. ,marjan.zare@gmail.com; mar.zare@khalums.ac.ir
2- Pathology Department, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran. & Maternal-Fetal Medicine Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
3- Department of Public Health, Khalkhal University of Medical Sciences, Khalkhal, Iran. ,
Full-Text [PDF 509 kb]
(301 Downloads)
| Abstract (HTML) (360 Views)
m = kn
α = type I error = 0.05 (Z α 2 =1.96) Z 0.02 =2.05)
When n is estimated, it is multiplied by k to estimate m.
2.4. Variable definition and measurement
PPROM (a membrane rupture occurring before 37 wk of gestation, diagnosed by a sterile speculum in the first examination before prescribing any medication to mothers) (yes/no); (16) Chorioamnionitis (acute inflammation of the membranes and chorion of the placenta, typically due to ascending polymicrobial bacterial infection in the setting of membrane rupture) (yes/no); gestational age (the last menstrual period at the first-trimester ultrasound examination) (wk), gravid (number), parity (number), delivery type (normal/cesarean section), fever (yes/no) (temperature above 38oC) (yes/no), vaginosis (yes/no), uterine tenderness (yes/no), tachycardia (yes/no), delivery time (wk), birth weight (gr), 1 min Apgar score (minute), 5 min Apgar score (minute), NICU admission (yes/no), and sepsis (yes/no).
For a definitive diagnosis of chorioamnionitis, the placenta of women who consented was sent to a pathologist for pathologic and histologic analysis. The tissue was fixed in 10% buffered formalin and then embedded in paraffin. Multiple sections were taken from each placenta, including 2 sections from the umbilical cord and one from the membrane roll, and stained with hematoxylin-eosin. The criterion for pathologic chorioamnionitis was the presence of neutrophils in the chorion or the chorion and amnion on the examination of a membrane roll and chorionic plate of the placenta based on Khong et al. (17).
2.5. Ethical Considerations
The Institutional Review Board and the Medical Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran approved this study (Code: IR.SUMS.REC.1399.922). Written informed consent was obtained from all mothers who participated in this study. All ethical principles were in concordance with the World Medical Association Declaration of Helsinki.
2.6. Statistical Analysis
Quantitative and qualitative variables were described as mean ± SD/median (interquartile range: Q3-Q1) and frequency (relative frequency), respectively. The Kolmogorov-Smirnov normality test was used to test normal distribution. Independent sample t test, Mann-Whitney test, Chi-square test, Fisher’s exact test, receiving operating characteristic curve (ROC) procedure with maximum Uden-index (sensitivity + specificity-1) for cut-off points, sensitivity, specificity, negative predictive value, positive predictive value, accuracy, KAPPA agreement coefficient, and logistic regression with adjusted odds ratio and 95% confidence interval (ORadj [95% CI]) were used to analyze the data. Adjustment was done using a p < 0.20 in univariate analysis. The significance level was considered 0.05 for all tests. IBM Statistical Package for the Social Sciences, version 22, SPSS Inc., Chicago, Illinois, USA, and MedCalc software Ltd. version 20.015, Belgium, software tools were used.
3. Results
Full-Text: (46 Views)
1. Introduction
Rupture of the membrane refers to the condition in which the membranes of the placenta rupture before the uterine contractions begin; if this occurs before the 37th wk of pregnancy, it is called preterm premature rupture of membrane (PPROM). PPROM occurs in 3% of pregnancies and includes more than 1/3rd of preterm and premature deliveries (1). Infections, up to 50%, play the most important role in PPROM (2). Chorioamnionitis, also known as intra-amniotic infection, is an acute inflammation of the fetal membrane (amniotic sac, chorionic villus, and amniotic fluid) caused by bacterial infection (2, 3). Chorioamnionitis, with a prevalence of 9.7 per 1000 live births (4), is one of the main causes of preterm labor, causing complications for the baby in later life (5).
The diagnosis of chorioamnionitis infections is based on the clinical findings, especially fever. However, laboratory tests contribute to early diagnosis or rule out the disease, especially when the clinical signs and symptoms are unclear. The National Institute of Child Health and Human Development recommended the use of the term “triple I” to address the heterogeneity of this disorder (6, 7). The term triple I refers to “intrauterine infection or inflammation or both and is defined by strict diagnostic criteria”. Although these terminologies are used, they have not been widely adopted (8, 9), so no clear-cut gold standard has been established for detecting chorioamnionitis. Serum amyloid A (SAA) is a major acute-phase reactant, with circulating levels that can increase over 1000-fold in response to inflammation and infection. Beyond its systemic production in the liver, SAA also acts as a local alarm signal within gestational tissues. It promotes labor by stimulating inflammatory mediators like cytokines and prostaglandins, contributes to membrane rupture by breaking down collagen, and may aid placental development by enhancing cell invasion. Consequently, SAA levels rise significantly in both normal parturition and pregnancy complications such as pre-eclampsia and PPROM. This physiological role makes the investigation of maternal serum SAA a promising, minimally invasive diagnostic alternative. Unlike more invasive samples like amniotic fluid or placental tissue, a serum marker is more accessible and rapidly obtainable. While other inflammatory markers like C-reactive protein (CRP) and white blood cell (WBC) count have diagnostic value, SAA's dynamic response and direct involvement in pregnancy-specific pathways offer a potentially superior tool for identifying intra-amniotic infection and inflammation (8). Yet, there are discrepancies about the superiority of SAA, CRP, and WBC in diagnosing the infection (9-11). A study has identified SAA as the most sensitive inflammatory parameter, which is very similar to CRP; however, recent studies have shown that SAA may be superior to CRP in diagnosing bacterial and viral infections (12, 13). Although the importance of SAA has recently been suggested, few studies have investigated its accuracy in PPROM chorioamnionitis. Knowledge of the PPROM etiology has an important effect on the treatment and management of these mothers, prolongation of pregnancy, improvement of the fetal condition, and minimization of the complications of premature fetuses after birth.
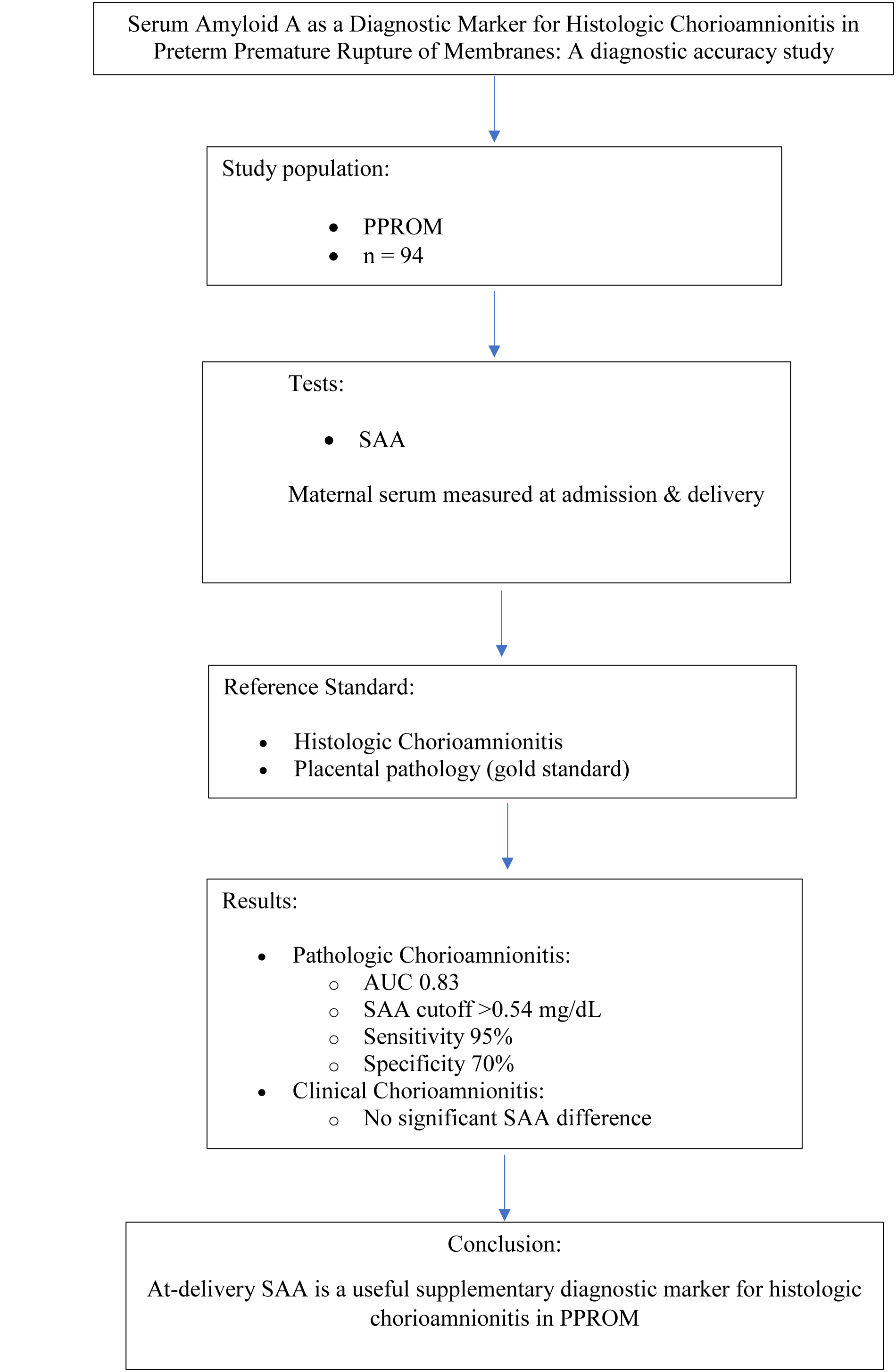
This study primarily aimed to evaluate the accuracy of maternal serum SAA protein levels in diagnosing histologic chorioamnionitis following PPROM. Secondarily, it assessed their accuracy for diagnosing clinical chorioamnionitis; in addition, CRP and WBC diagnostic values were checked clinically and pathologically.
2. Materials and Methods
2.1. Study design and participants
In this prospective diagnostic accuracy study, PPROM women between 24 and 34 wk of gestation who were referred to Namazi, Hafez, and Zeinabiyeh hospitals, Shiraz, Iran from March 2022 to March 2023 were followed until delivery.
Participants were assessed within 24 hr of membrane rupture by a perinatology specialist, and standard PPROM management was started. Routine care consisted of hospitalization, administration of antibiotics (intravenous ampicillin for 48 hr followed by oral ampicillin and azithromycin for 6 days), antenatal corticosteroid therapy with betamethasone for fetal lung maturation, and tocolysis with Nifedipine or Indomethacin during the first 48 hr when indicated. Indomethacin was used exclusively for pregnancies with gestational age < 32 wk, and magnesium sulfate was given for neuroprotection up to 31 ± 6 wk of gestation. Hormonal therapy was provided in cases with documented uterine contractions. Those women with PPROM who were candidates for pregnancy termination due to having the clinical signs of chorioamnionitis or other perinatal complications were followed until delivery. The clinical signs of chorioamnionitis include fever above 38°C, accompanied by at least 2 of the following symptoms: maternal tachycardia (> 100 beats/min), or fetal tachycardia (> 160 beats/min) and tenderness. Maternal blood samples were collected upon admission and again at the time of delivery for measurement of SAA, WBC, and CRP.
After delivery, all placentas were examined for histopathological evidence of chorioamnionitis. Based on the pathology findings, participants were classified into 2 groups: a) pathologic chorioamnionitis group (n = 50) and b) normal placenta control group (n = 44). Pathologic chorioamnionitis was defined as the presence of neutrophilic infiltration within the chorion or amniotic membranes.
Placental tissue, fetal membranes, and chorionic samples were analyzed for SAA, WBC, and CRP levels at the time of delivery.
Data were collected by a gynecology and obstetrics resident, who was supervised by an attending obstetrician-gynecologist. Collected variables included the following maternal characteristics: gestational age, gravidity, parity, mode of delivery, fever, vaginal infection, uterine tenderness, maternal tachycardia, and time of delivery. Neonatal outcomes assessed were the 1-min and 5-min Apgar scores, neonate intensive care unit (NICU) admission, and neonatal sepsis.
The level of SAA in the serum was determined by an ELISA kit (Cusabio Human SAA). The WBC counts were obtained through the Biorex Fars Innovative Diagnosis system. CRP levels were measured by the BT3000 analyzer (Biotecnica, Italy).
2.2. Eligibility criteria
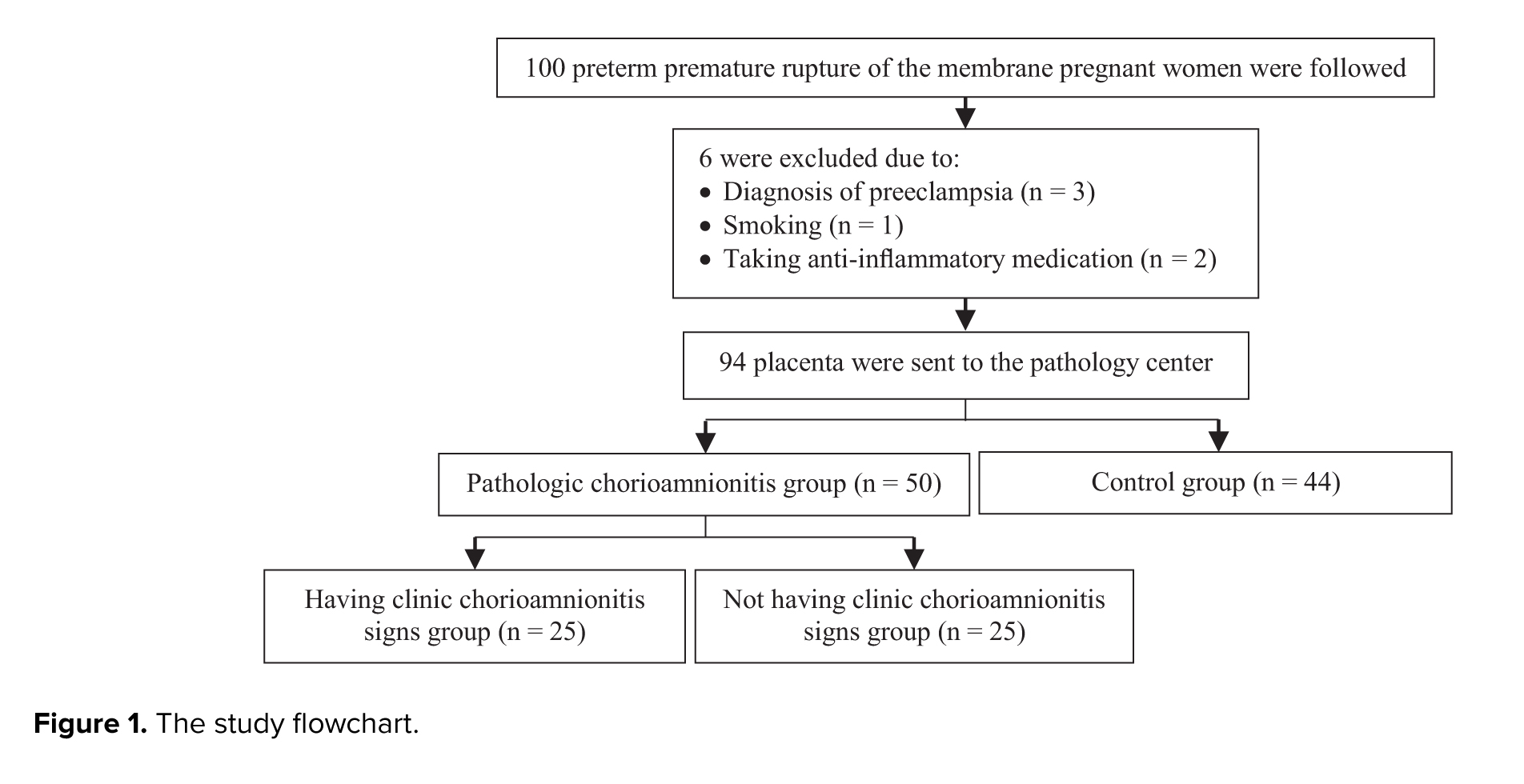
Those candidates having singleton pregnancy with PPROM between 24 and 34 wk of gestational age were included. The exclusion criteria were pregnant women with congenital anomalies, pre-eclampsia, prenatal bleeding, diabetes mellitus, smoking, and drug abuse. Those with maternal diseases, including liver, kidney, heart, immune, and infectious diseases; women with polyhydramnios; history of anti-inflammatory and non-steroidal anti-inflammatory drugs such as aspirin, ibuprofen, naproxen, statins, niacin, and fibrate. Recent surgery, burns, and body mass index < 18 kg/m2 were a few other exclusion criteria (Figure 1).
2.3. Sample size
Using information from Oh et al. study (14), the estimated total sample size was 94 participants, including 50 in the chorioamnionitis group and 44 in the control group. The sample size formula is as follows:
Rupture of the membrane refers to the condition in which the membranes of the placenta rupture before the uterine contractions begin; if this occurs before the 37th wk of pregnancy, it is called preterm premature rupture of membrane (PPROM). PPROM occurs in 3% of pregnancies and includes more than 1/3rd of preterm and premature deliveries (1). Infections, up to 50%, play the most important role in PPROM (2). Chorioamnionitis, also known as intra-amniotic infection, is an acute inflammation of the fetal membrane (amniotic sac, chorionic villus, and amniotic fluid) caused by bacterial infection (2, 3). Chorioamnionitis, with a prevalence of 9.7 per 1000 live births (4), is one of the main causes of preterm labor, causing complications for the baby in later life (5).
The diagnosis of chorioamnionitis infections is based on the clinical findings, especially fever. However, laboratory tests contribute to early diagnosis or rule out the disease, especially when the clinical signs and symptoms are unclear. The National Institute of Child Health and Human Development recommended the use of the term “triple I” to address the heterogeneity of this disorder (6, 7). The term triple I refers to “intrauterine infection or inflammation or both and is defined by strict diagnostic criteria”. Although these terminologies are used, they have not been widely adopted (8, 9), so no clear-cut gold standard has been established for detecting chorioamnionitis. Serum amyloid A (SAA) is a major acute-phase reactant, with circulating levels that can increase over 1000-fold in response to inflammation and infection. Beyond its systemic production in the liver, SAA also acts as a local alarm signal within gestational tissues. It promotes labor by stimulating inflammatory mediators like cytokines and prostaglandins, contributes to membrane rupture by breaking down collagen, and may aid placental development by enhancing cell invasion. Consequently, SAA levels rise significantly in both normal parturition and pregnancy complications such as pre-eclampsia and PPROM. This physiological role makes the investigation of maternal serum SAA a promising, minimally invasive diagnostic alternative. Unlike more invasive samples like amniotic fluid or placental tissue, a serum marker is more accessible and rapidly obtainable. While other inflammatory markers like C-reactive protein (CRP) and white blood cell (WBC) count have diagnostic value, SAA's dynamic response and direct involvement in pregnancy-specific pathways offer a potentially superior tool for identifying intra-amniotic infection and inflammation (8). Yet, there are discrepancies about the superiority of SAA, CRP, and WBC in diagnosing the infection (9-11). A study has identified SAA as the most sensitive inflammatory parameter, which is very similar to CRP; however, recent studies have shown that SAA may be superior to CRP in diagnosing bacterial and viral infections (12, 13). Although the importance of SAA has recently been suggested, few studies have investigated its accuracy in PPROM chorioamnionitis. Knowledge of the PPROM etiology has an important effect on the treatment and management of these mothers, prolongation of pregnancy, improvement of the fetal condition, and minimization of the complications of premature fetuses after birth.
This study primarily aimed to evaluate the accuracy of maternal serum SAA protein levels in diagnosing histologic chorioamnionitis following PPROM. Secondarily, it assessed their accuracy for diagnosing clinical chorioamnionitis; in addition, CRP and WBC diagnostic values were checked clinically and pathologically.
2. Materials and Methods
2.1. Study design and participants
In this prospective diagnostic accuracy study, PPROM women between 24 and 34 wk of gestation who were referred to Namazi, Hafez, and Zeinabiyeh hospitals, Shiraz, Iran from March 2022 to March 2023 were followed until delivery.
Participants were assessed within 24 hr of membrane rupture by a perinatology specialist, and standard PPROM management was started. Routine care consisted of hospitalization, administration of antibiotics (intravenous ampicillin for 48 hr followed by oral ampicillin and azithromycin for 6 days), antenatal corticosteroid therapy with betamethasone for fetal lung maturation, and tocolysis with Nifedipine or Indomethacin during the first 48 hr when indicated. Indomethacin was used exclusively for pregnancies with gestational age < 32 wk, and magnesium sulfate was given for neuroprotection up to 31 ± 6 wk of gestation. Hormonal therapy was provided in cases with documented uterine contractions. Those women with PPROM who were candidates for pregnancy termination due to having the clinical signs of chorioamnionitis or other perinatal complications were followed until delivery. The clinical signs of chorioamnionitis include fever above 38°C, accompanied by at least 2 of the following symptoms: maternal tachycardia (> 100 beats/min), or fetal tachycardia (> 160 beats/min) and tenderness. Maternal blood samples were collected upon admission and again at the time of delivery for measurement of SAA, WBC, and CRP.
After delivery, all placentas were examined for histopathological evidence of chorioamnionitis. Based on the pathology findings, participants were classified into 2 groups: a) pathologic chorioamnionitis group (n = 50) and b) normal placenta control group (n = 44). Pathologic chorioamnionitis was defined as the presence of neutrophilic infiltration within the chorion or amniotic membranes.
Placental tissue, fetal membranes, and chorionic samples were analyzed for SAA, WBC, and CRP levels at the time of delivery.
Data were collected by a gynecology and obstetrics resident, who was supervised by an attending obstetrician-gynecologist. Collected variables included the following maternal characteristics: gestational age, gravidity, parity, mode of delivery, fever, vaginal infection, uterine tenderness, maternal tachycardia, and time of delivery. Neonatal outcomes assessed were the 1-min and 5-min Apgar scores, neonate intensive care unit (NICU) admission, and neonatal sepsis.
The level of SAA in the serum was determined by an ELISA kit (Cusabio Human SAA). The WBC counts were obtained through the Biorex Fars Innovative Diagnosis system. CRP levels were measured by the BT3000 analyzer (Biotecnica, Italy).
2.2. Eligibility criteria
Those candidates having singleton pregnancy with PPROM between 24 and 34 wk of gestational age were included. The exclusion criteria were pregnant women with congenital anomalies, pre-eclampsia, prenatal bleeding, diabetes mellitus, smoking, and drug abuse. Those with maternal diseases, including liver, kidney, heart, immune, and infectious diseases; women with polyhydramnios; history of anti-inflammatory and non-steroidal anti-inflammatory drugs such as aspirin, ibuprofen, naproxen, statins, niacin, and fibrate. Recent surgery, burns, and body mass index < 18 kg/m2 were a few other exclusion criteria (Figure 1).
2.3. Sample size
Using information from Oh et al. study (14), the estimated total sample size was 94 participants, including 50 in the chorioamnionitis group and 44 in the control group. The sample size formula is as follows:
α = type I error = 0.05 (
When n is estimated, it is multiplied by k to estimate m.
2.4. Variable definition and measurement
PPROM (a membrane rupture occurring before 37 wk of gestation, diagnosed by a sterile speculum in the first examination before prescribing any medication to mothers) (yes/no); (16) Chorioamnionitis (acute inflammation of the membranes and chorion of the placenta, typically due to ascending polymicrobial bacterial infection in the setting of membrane rupture) (yes/no); gestational age (the last menstrual period at the first-trimester ultrasound examination) (wk), gravid (number), parity (number), delivery type (normal/cesarean section), fever (yes/no) (temperature above 38oC) (yes/no), vaginosis (yes/no), uterine tenderness (yes/no), tachycardia (yes/no), delivery time (wk), birth weight (gr), 1 min Apgar score (minute), 5 min Apgar score (minute), NICU admission (yes/no), and sepsis (yes/no).
For a definitive diagnosis of chorioamnionitis, the placenta of women who consented was sent to a pathologist for pathologic and histologic analysis. The tissue was fixed in 10% buffered formalin and then embedded in paraffin. Multiple sections were taken from each placenta, including 2 sections from the umbilical cord and one from the membrane roll, and stained with hematoxylin-eosin. The criterion for pathologic chorioamnionitis was the presence of neutrophils in the chorion or the chorion and amnion on the examination of a membrane roll and chorionic plate of the placenta based on Khong et al. (17).
2.5. Ethical Considerations
The Institutional Review Board and the Medical Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran approved this study (Code: IR.SUMS.REC.1399.922). Written informed consent was obtained from all mothers who participated in this study. All ethical principles were in concordance with the World Medical Association Declaration of Helsinki.
2.6. Statistical Analysis
Quantitative and qualitative variables were described as mean ± SD/median (interquartile range: Q3-Q1) and frequency (relative frequency), respectively. The Kolmogorov-Smirnov normality test was used to test normal distribution. Independent sample t test, Mann-Whitney test, Chi-square test, Fisher’s exact test, receiving operating characteristic curve (ROC) procedure with maximum Uden-index (sensitivity + specificity-1) for cut-off points, sensitivity, specificity, negative predictive value, positive predictive value, accuracy, KAPPA agreement coefficient, and logistic regression with adjusted odds ratio and 95% confidence interval (ORadj [95% CI]) were used to analyze the data. Adjustment was done using a p < 0.20 in univariate analysis. The significance level was considered 0.05 for all tests. IBM Statistical Package for the Social Sciences, version 22, SPSS Inc., Chicago, Illinois, USA, and MedCalc software Ltd. version 20.015, Belgium, software tools were used.
3. Results
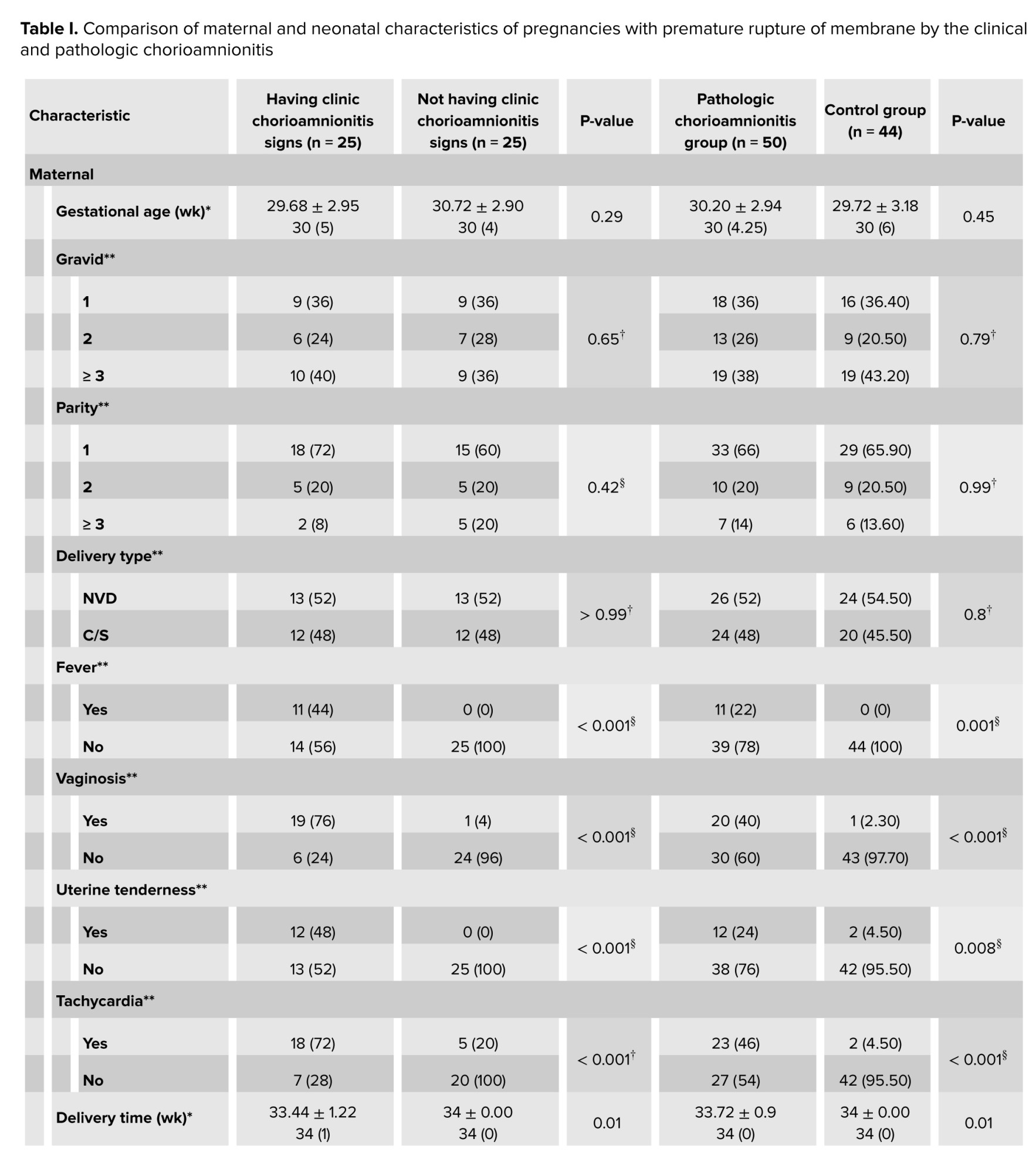
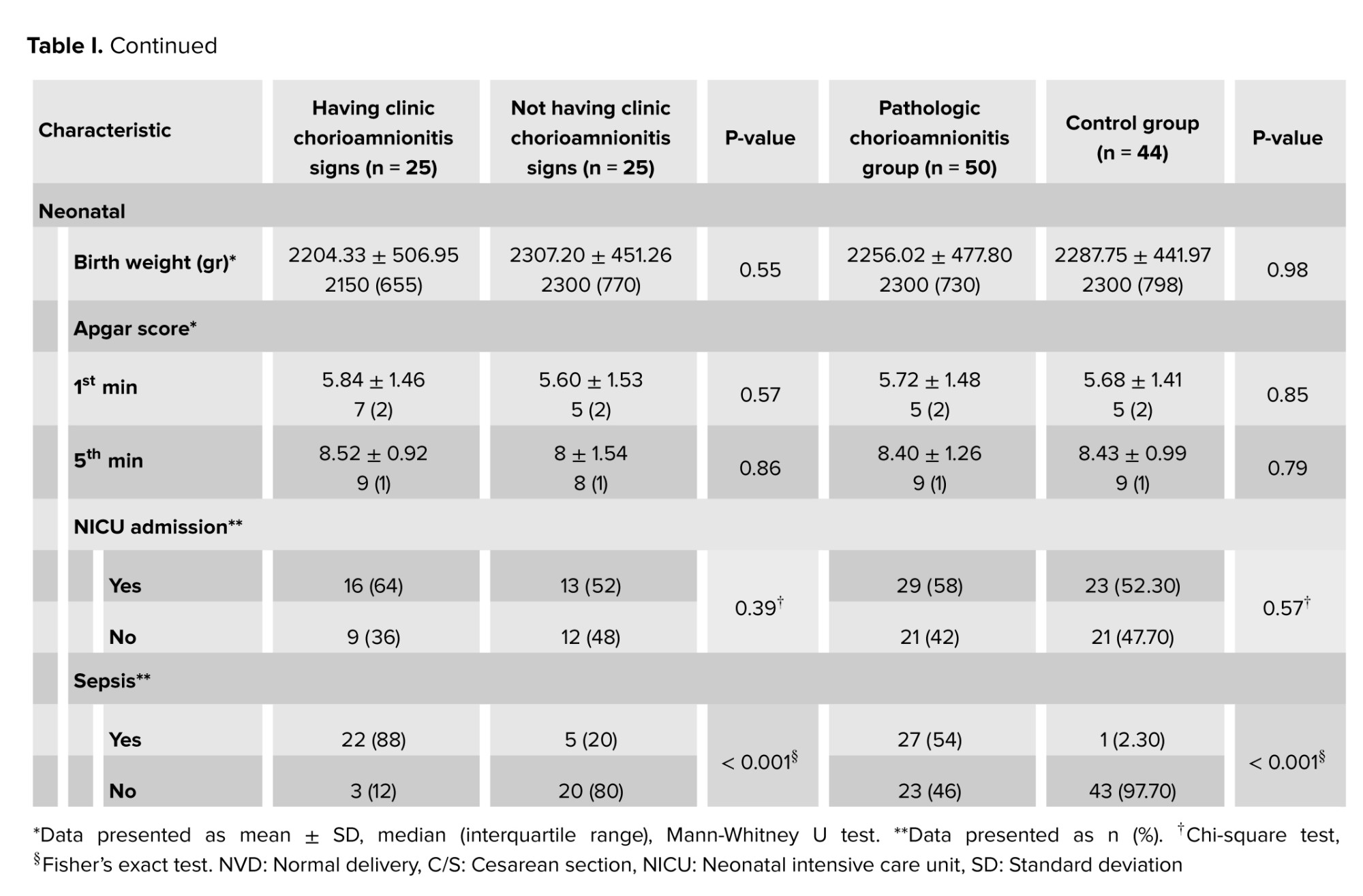
From the 94 participants, 50 (43.20%) were pathologically diagnosed with chorioamnionitis, and 44 (46.8%) belonged to control group. In addition, 50% of women with pathological chorioamnionitis (25/50) were clinically diagnosed with chorioamnionitis, and the remaining 50% (25/50) had no clinical signs of chorioamnionitis. The maternal and neonatal characteristics of pregnancies with PPROM were compared clinically and pathologically in table I.
Clinically and pathologically, no significant differences were observed between chorioamnionitis and their controls regarding gestational age, gravid, parity, delivery type, birth weight, 1 min Apgar score, 5 min Apgar score, and NICU admission. However, fever, tenderness, vaginosis, tachycardia, and neonatal sepsis were significantly more in the chorioamnionitis group. In addition, the delivery time was significantly higher in the control groups compared with the chorioamnionitis groups.
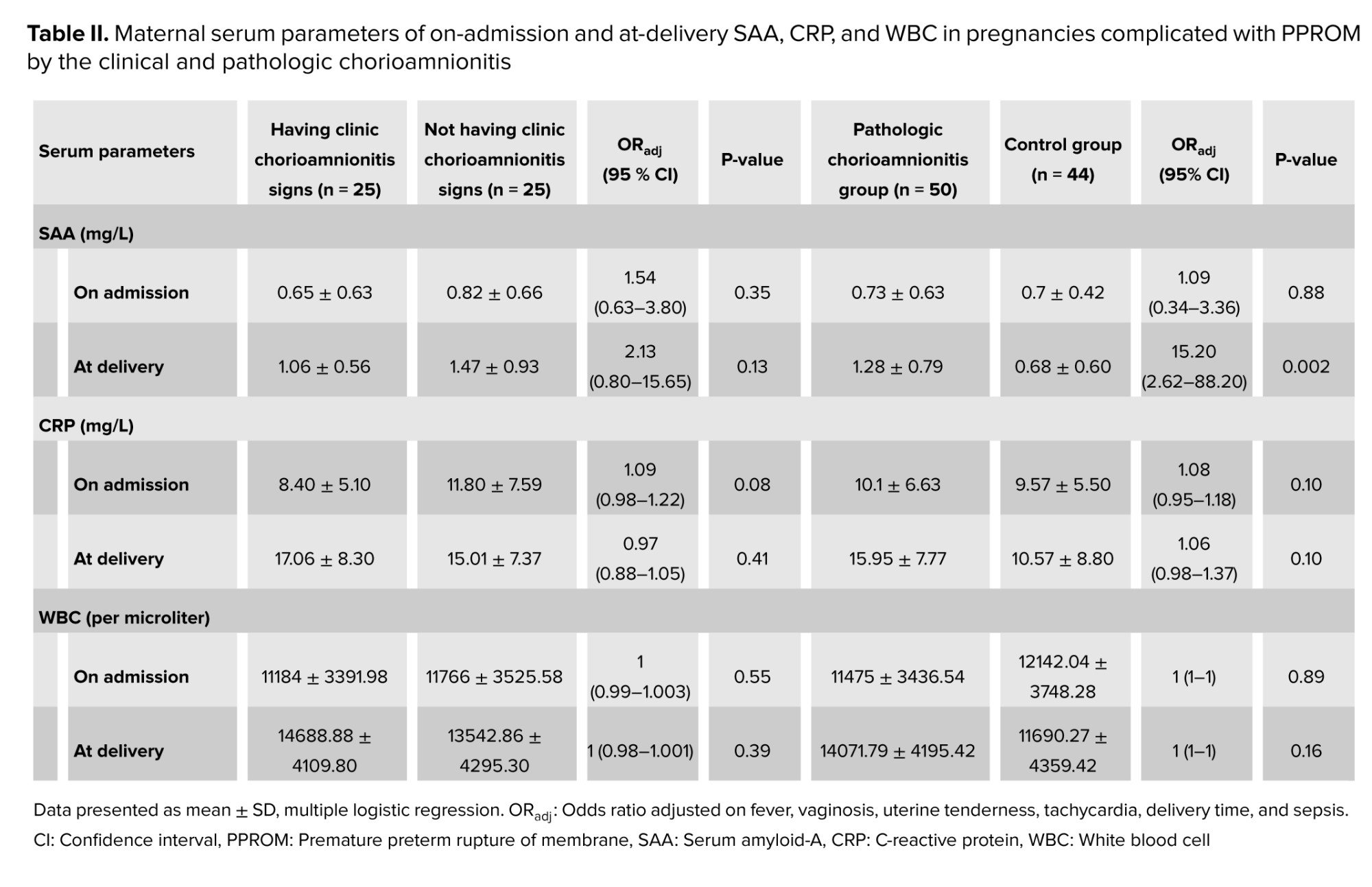
Clinical and pathologic serum features, including on-admission and at-delivery SAA, CRP, and WBC, were compared between chorioamnionitis and their controls, as shown in table II.
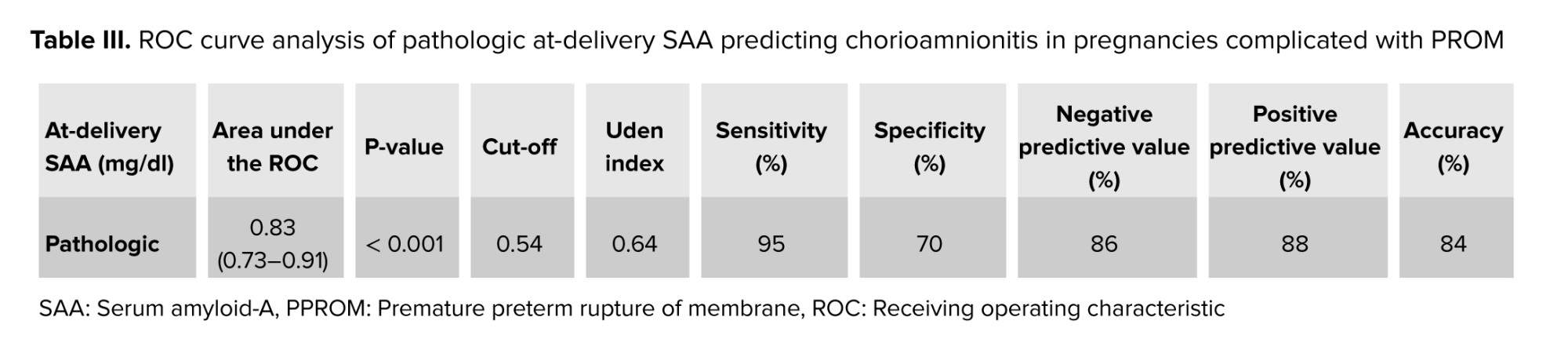
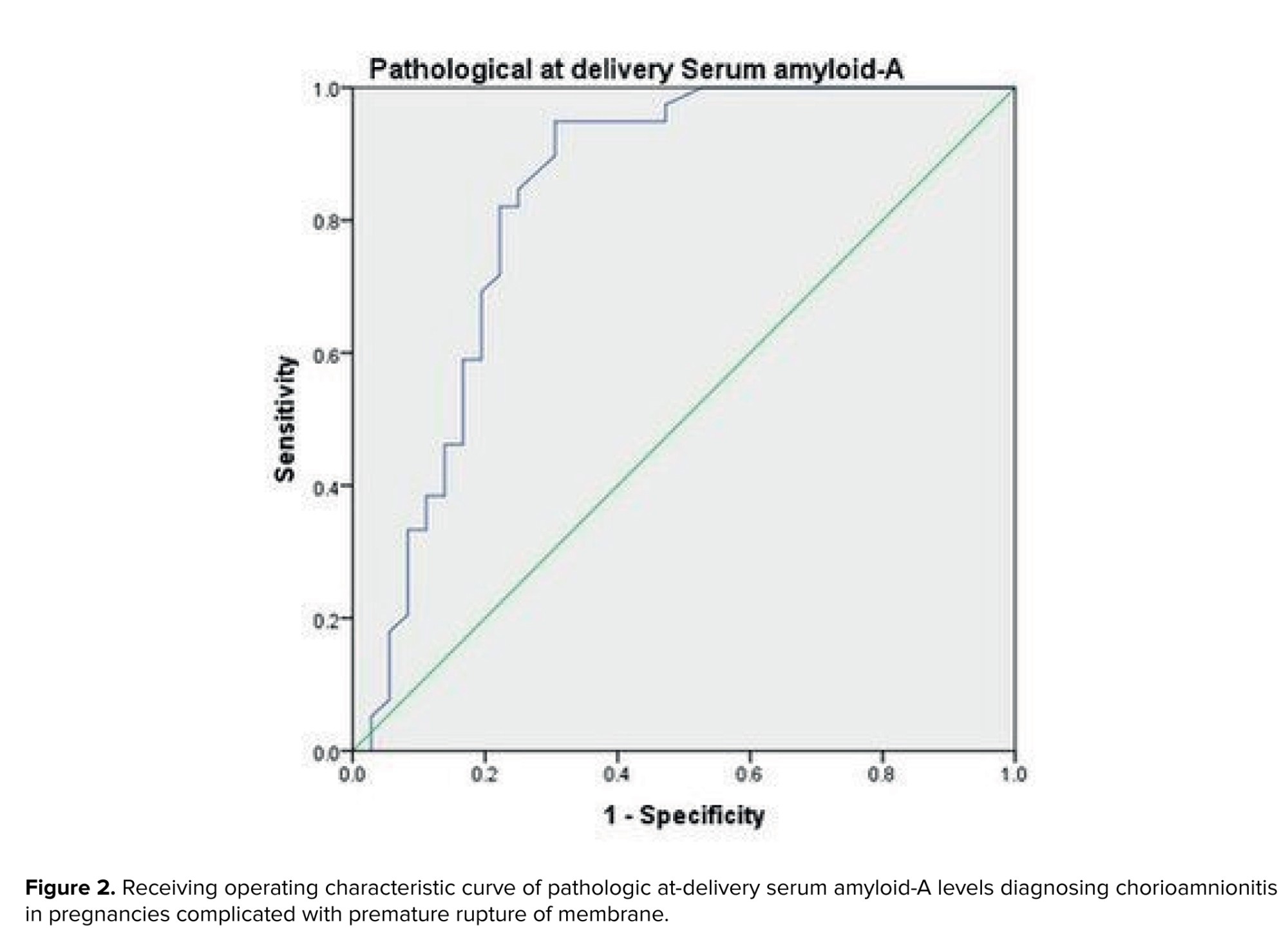
A unit increase in pathological at-delivery SAA would significantly increase the odds of chorioamnionitis by 15.2 in PPROM mothers; however, clinical and pathological on-admission SAA, as well as clinical and pathological on-admission and at-delivery CRP and WBC, were significantly the same. The ROC analysis of pathologic chorioamnionitis diagnosed by at-delivery SAA in PPROM mothers has been shown in figure 2 and table III.
At-delivery SAA was accurate enough in predicting pathologic chorioamnionitis in PPROM mothers (p < 0.001).
Of 94 pregnancies, 50% (25/50) of mothers had both pathologic and clinical chorioamnionitis, and 95.50% (42/44) pregnancies had neither pathologic nor clinical chorioamnionitis. The KAPPA agreement between the clinical and pathologic chorioamnionitis diagnosis between 94 PPROM pregnancies enjoyed moderate agreement of 0.44 (p < 0.001). The rate of false-negative and false-positive clinic chorioamnionitis were 50% (5/50) and 4% (2/44), respectively, demonstrating that a mother with no clinical chorioamnionitis PPROM could have chorioamnionitis one with a 50% chance, even with no clinical signs.
4. Discussion
The present study was designed to evaluate the utility of maternal SAA levels in predicting chorioamnionitis in women with PPROM. Our key finding is that at-delivery SAA demonstrates excellent accuracy in predicting pathologic chorioamnionitis, even in the absence of clinical signs. This suggests SAA may be a superior biomarker for identifying subclinical intra-amniotic infection. While we controlled for key variables like smoking and clinical chorioamnionitis, other maternal inflammatory conditions (e.g., autoimmune disorders and active systemic infections) could theoretically elevate SAA levels and represent potential, albeit unmeasured, confounders.
We first observed only a moderate agreement between clinical and histopathologic diagnoses of chorioamnionitis, underscoring the well-documented limitation of clinical criteria alone (18). As expected, traditional clinical markers such as maternal fever, uterine tenderness, vaginosis, and tachycardia were significantly more prevalent in the clinical chorioamnionitis group (19-21). However, the critical insight from our data is that a significant number of women with confirmed histologic chorioamnionitis presented with no such signs yet exhibited elevated SAA levels. This aligns with a growing body of evidence suggesting that the clinical presentation of chorioamnionitis is often subtle and non-specific, leading to underdiagnosis if reliance is placed solely on clinical examination (22).
The neonatal outcomes further highlight the insidious nature of this condition. The lack of significant difference in Apgar scores and NICU admission rates between groups is likely a reflection of our study population and standard obstetric management. As delivery is routinely expedited in PPROM, especially before 34 wk, the immediate neonatal adaptation (reflected by Apgar scores) may not yet be affected. However, the significantly higher incidence of neonatal sepsis in the chorioamnionitis groups indicates that the infectious process was underway in utero, often manifesting subclinically in the immediate postpartum period (23). This reinforces the necessity for close postnatal monitoring for sepsis in neonates born to PPROM mothers, particularly those with elevated maternal inflammatory markers like SAA.
Our central finding regarding the diagnostic accuracy of SAA places it within a complex and often contradictory landscape of biomarker research. Our results are consistent with several studies that have identified SAA as a sensitive acute-phase reactant. For instance, a study presented that among various markers, SAA showed the most pronounced increase in women with histologic chorioamnionitis, supporting its role in detecting subclinical infection (24). Similarly, a more recent investigation found that SAA had a higher predictive value for early-onset neonatal sepsis than CRP (25).
However, the role of CRP remains a point of contention. Our study found SAA to be a more accurate predictor than CRP, which contrasts with other reports that champion CRP's diagnostic utility (26, 27). This heterogeneity can be attributed to several factors: varying clinical definitions of chorioamnionitis (clinical vs. histologic), differences in study design (prospective vs. retrospective), and, crucially, the gestational age at which biomarkers are measured. The timing of our measurement, "at-delivery", is a particular strength, capturing the inflammatory state at its peak, but it may not be directly comparable to studies measuring markers at the time of PPROM diagnosis.
A potential pathophysiological explanation for SAA's performance is its rapid kinetics. SAA concentrations can increase 1000-fold within 24-48 hr of an inflammatory stimulus, much faster and more dramatically than CRP (28). This makes it exceptionally sensitive for detecting acute insults like ascending infection following PPROM (24). Furthermore, while some studies have shown no increase in fetal cord SAA, suggesting it does not cross the placenta, the maternal inflammatory response itself is a key driver of fetal sequelae. The "maternal SAA response" to intra-amniotic infection may therefore be a more reliable indicator of the fetal inflammatory environment than direct fetal measurement.
Despite the promising performance of SAA, it is prudent to consider it as part of a multi-modal diagnostic approach. A previous study sensibly suggested that CRP should be used as a supplementary test to confirm infection (29). We echo this view but propose that SAA may be the more sensitive initial screening tool. The integrated use of both markers, perhaps combined with sonographic findings and advanced tests like amniotic fluid PCR, could provide a more robust diagnostic algorithm than any single test alone (18).
4.1. Strengths and Limitations
The large sample size and consequently high study power, well-defined study population, assessment of comprehensive background variables, investigating of on-admission and at-delivery SAA, PRC, and WBC factors, and evaluating of clinical and pathological diagnosis of chorioamnionitis were the key points of the current work. As one limitation of the work, SAA, CRP, and WBC were not checked in the cords and in neonates; another limitation was skipping the long-term evaluation of the infants born from high SAA level PPROM mothers for further anthropometric and mental indices.
5. Conclusion
In conclusion, our study strengthens the evidence for maternal SAA as a highly accurate biomarker for histologic chorioamnionitis in PPROM, capable of identifying cases that would otherwise be missed by clinical criteria. The discrepancies between our findings and some CRP-based studies highlight the need for standardized diagnostic criteria and biomarker timing in future research. A prospective, multi-center study measuring a panel of biomarkers (including SAA, CRP, and interlukin-6) at standardized time points from PPROM diagnosis until delivery is warranted to establish a definitive diagnostic protocol. Ultimately, the timely identification of subclinical chorioamnionitis using sensitive markers like SAA can guide targeted antimicrobial therapy and improve neonatal outcomes.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author (marjan.zare@gmail.com).
Author Contributions
A. Faraji, M. Mehraban, and M. Zare contributed to the conception, design, data acquisition, analysis, and interpretation of data for the work. They also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. M. Kasraeian, M. Akbarzadeh-Jahromi, H. Vafaei, and N. Asadi have contributed to the conception of the work; they also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. Z. Oveisi and M. Kasraie contributed to the conception, data acquisition, and interpretation of data for the work; they also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
We would like to acknowledge Dr. Nasrin Shokrpour for improving the quality of the English language in the manuscript. The work has been extracted from a fellowship student thesis in perinatology, Dr. Mitra Mehraban (grant number: 20265), which has been awarded by Shiraz University of Medical Sciences, Shiraz, Iran. No AI was used for writing, editing, or grammar check.
Conflict of Interest
The authors declare that there is no conflict of interest.
Clinically and pathologically, no significant differences were observed between chorioamnionitis and their controls regarding gestational age, gravid, parity, delivery type, birth weight, 1 min Apgar score, 5 min Apgar score, and NICU admission. However, fever, tenderness, vaginosis, tachycardia, and neonatal sepsis were significantly more in the chorioamnionitis group. In addition, the delivery time was significantly higher in the control groups compared with the chorioamnionitis groups.
Clinical and pathologic serum features, including on-admission and at-delivery SAA, CRP, and WBC, were compared between chorioamnionitis and their controls, as shown in table II.
A unit increase in pathological at-delivery SAA would significantly increase the odds of chorioamnionitis by 15.2 in PPROM mothers; however, clinical and pathological on-admission SAA, as well as clinical and pathological on-admission and at-delivery CRP and WBC, were significantly the same. The ROC analysis of pathologic chorioamnionitis diagnosed by at-delivery SAA in PPROM mothers has been shown in figure 2 and table III.
At-delivery SAA was accurate enough in predicting pathologic chorioamnionitis in PPROM mothers (p < 0.001).
Of 94 pregnancies, 50% (25/50) of mothers had both pathologic and clinical chorioamnionitis, and 95.50% (42/44) pregnancies had neither pathologic nor clinical chorioamnionitis. The KAPPA agreement between the clinical and pathologic chorioamnionitis diagnosis between 94 PPROM pregnancies enjoyed moderate agreement of 0.44 (p < 0.001). The rate of false-negative and false-positive clinic chorioamnionitis were 50% (5/50) and 4% (2/44), respectively, demonstrating that a mother with no clinical chorioamnionitis PPROM could have chorioamnionitis one with a 50% chance, even with no clinical signs.
4. Discussion
The present study was designed to evaluate the utility of maternal SAA levels in predicting chorioamnionitis in women with PPROM. Our key finding is that at-delivery SAA demonstrates excellent accuracy in predicting pathologic chorioamnionitis, even in the absence of clinical signs. This suggests SAA may be a superior biomarker for identifying subclinical intra-amniotic infection. While we controlled for key variables like smoking and clinical chorioamnionitis, other maternal inflammatory conditions (e.g., autoimmune disorders and active systemic infections) could theoretically elevate SAA levels and represent potential, albeit unmeasured, confounders.
We first observed only a moderate agreement between clinical and histopathologic diagnoses of chorioamnionitis, underscoring the well-documented limitation of clinical criteria alone (18). As expected, traditional clinical markers such as maternal fever, uterine tenderness, vaginosis, and tachycardia were significantly more prevalent in the clinical chorioamnionitis group (19-21). However, the critical insight from our data is that a significant number of women with confirmed histologic chorioamnionitis presented with no such signs yet exhibited elevated SAA levels. This aligns with a growing body of evidence suggesting that the clinical presentation of chorioamnionitis is often subtle and non-specific, leading to underdiagnosis if reliance is placed solely on clinical examination (22).
The neonatal outcomes further highlight the insidious nature of this condition. The lack of significant difference in Apgar scores and NICU admission rates between groups is likely a reflection of our study population and standard obstetric management. As delivery is routinely expedited in PPROM, especially before 34 wk, the immediate neonatal adaptation (reflected by Apgar scores) may not yet be affected. However, the significantly higher incidence of neonatal sepsis in the chorioamnionitis groups indicates that the infectious process was underway in utero, often manifesting subclinically in the immediate postpartum period (23). This reinforces the necessity for close postnatal monitoring for sepsis in neonates born to PPROM mothers, particularly those with elevated maternal inflammatory markers like SAA.
Our central finding regarding the diagnostic accuracy of SAA places it within a complex and often contradictory landscape of biomarker research. Our results are consistent with several studies that have identified SAA as a sensitive acute-phase reactant. For instance, a study presented that among various markers, SAA showed the most pronounced increase in women with histologic chorioamnionitis, supporting its role in detecting subclinical infection (24). Similarly, a more recent investigation found that SAA had a higher predictive value for early-onset neonatal sepsis than CRP (25).
However, the role of CRP remains a point of contention. Our study found SAA to be a more accurate predictor than CRP, which contrasts with other reports that champion CRP's diagnostic utility (26, 27). This heterogeneity can be attributed to several factors: varying clinical definitions of chorioamnionitis (clinical vs. histologic), differences in study design (prospective vs. retrospective), and, crucially, the gestational age at which biomarkers are measured. The timing of our measurement, "at-delivery", is a particular strength, capturing the inflammatory state at its peak, but it may not be directly comparable to studies measuring markers at the time of PPROM diagnosis.
A potential pathophysiological explanation for SAA's performance is its rapid kinetics. SAA concentrations can increase 1000-fold within 24-48 hr of an inflammatory stimulus, much faster and more dramatically than CRP (28). This makes it exceptionally sensitive for detecting acute insults like ascending infection following PPROM (24). Furthermore, while some studies have shown no increase in fetal cord SAA, suggesting it does not cross the placenta, the maternal inflammatory response itself is a key driver of fetal sequelae. The "maternal SAA response" to intra-amniotic infection may therefore be a more reliable indicator of the fetal inflammatory environment than direct fetal measurement.
Despite the promising performance of SAA, it is prudent to consider it as part of a multi-modal diagnostic approach. A previous study sensibly suggested that CRP should be used as a supplementary test to confirm infection (29). We echo this view but propose that SAA may be the more sensitive initial screening tool. The integrated use of both markers, perhaps combined with sonographic findings and advanced tests like amniotic fluid PCR, could provide a more robust diagnostic algorithm than any single test alone (18).
4.1. Strengths and Limitations
The large sample size and consequently high study power, well-defined study population, assessment of comprehensive background variables, investigating of on-admission and at-delivery SAA, PRC, and WBC factors, and evaluating of clinical and pathological diagnosis of chorioamnionitis were the key points of the current work. As one limitation of the work, SAA, CRP, and WBC were not checked in the cords and in neonates; another limitation was skipping the long-term evaluation of the infants born from high SAA level PPROM mothers for further anthropometric and mental indices.
5. Conclusion
In conclusion, our study strengthens the evidence for maternal SAA as a highly accurate biomarker for histologic chorioamnionitis in PPROM, capable of identifying cases that would otherwise be missed by clinical criteria. The discrepancies between our findings and some CRP-based studies highlight the need for standardized diagnostic criteria and biomarker timing in future research. A prospective, multi-center study measuring a panel of biomarkers (including SAA, CRP, and interlukin-6) at standardized time points from PPROM diagnosis until delivery is warranted to establish a definitive diagnostic protocol. Ultimately, the timely identification of subclinical chorioamnionitis using sensitive markers like SAA can guide targeted antimicrobial therapy and improve neonatal outcomes.
Data Availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author (marjan.zare@gmail.com).
Author Contributions
A. Faraji, M. Mehraban, and M. Zare contributed to the conception, design, data acquisition, analysis, and interpretation of data for the work. They also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. M. Kasraeian, M. Akbarzadeh-Jahromi, H. Vafaei, and N. Asadi have contributed to the conception of the work; they also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. Z. Oveisi and M. Kasraie contributed to the conception, data acquisition, and interpretation of data for the work; they also drafted the work and revised it critically for important intellectual content; they approved the final version of the work to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
We would like to acknowledge Dr. Nasrin Shokrpour for improving the quality of the English language in the manuscript. The work has been extracted from a fellowship student thesis in perinatology, Dr. Mitra Mehraban (grant number: 20265), which has been awarded by Shiraz University of Medical Sciences, Shiraz, Iran. No AI was used for writing, editing, or grammar check.
Conflict of Interest
The authors declare that there is no conflict of interest.
Type of Study: Original Article |
Subject:
Reproductive Pattology
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
